
Abstract
Churches and other faith-based organizations (FBOs) are a vital resource for HIV prevention and education efforts in African American communities. Few models describe how churches and FBOs have implemented such efforts within their congregations or communities, the challenges they faced, or the changes that resulted from such efforts. This article presents a framework for implementing HIV/AIDS prevention programs in African American churches based upon a qualitative investigation of Project FAITH (Fostering AIDS Initiatives that Heal), an HIV education and stigma reduction demonstration project conducted in South Carolina. Between 2007–2008 in-depth interviews were conducted with 8 pastors, 4 technical assistance providers, and 2 project champions; 22 care team members also participated in focus groups to identify domains associated with project implementation. Data analysis was conducted using a grounded theory approach and inputs, enablers, inhibitors, mediators, and outputs associated with HIV/AIDS prevention programs conducted as part of Project FAITH were identified. Furthermore, the framework includes the influences of public policy and stigma on the faith-based HIV/AIDS prevention programs in this study. The framework calls for the identification of individuals (members of the congregation and church leadership) who are passionate about and devoted to addressing HIV/AIDS, and provides specific mechanisms (i.e., health ministries) through which these individuals can organize, strategies for HIV/AIDS implementation, and areas of technical assistance and capacity building to maximize effectiveness of such efforts.
Introduction
HIV/AIDS
Churches have played a significant role in the development of the African American community 5 and have been regarded as the center of African American life. 6 They have served as centers for spiritual growth and development, political and civic activity, as well as health promotion and disease prevention 7,8 by providing health care and disease prevention programs to their congregations addressing a range of health issues, including increased fruit and vegetable consumption, 9 –11 overall nutrition, 12 breast cancer, 13,14 cervical cancer, 14 and colorectal cancer. 15 However, few churches have addressed HIV/AIDS through long-term sustained health promotion and disease prevention programs.
As the incidence of HIV/AIDS continues to grow in African American communities, the need for trusted, culturally competent community-based interventions continues to grow, with churches in a position to provide local, relevant, and accepted HIV prevention programs. However, unlike for community-based AIDS service organizations, no model or framework exists to help churches or faith-based organizations (FBOs) address the growing incidence of HIV in their communities.
In 2007, Collins and colleagues 16 developed a framework that agencies or community-based organizations (CBOs), whose specific missions were to provide HIV/AIDS prevention programs, could utilize to assess their capacity to implement evidence-based HIV/AIDS prevention programs. Specifically, CBOs could use the framework to assess inputs, catalysts, mediators, and outputs of HIV/AIDS prevention programs. Inputs, according to the framework, included structural factors, such as the organizational environment, governance, and programmatic infrastructure, as well as workforce and professional development and resources and support. Catalysts were defined as factors that affect motivation and readiness to implement HIV/AIDS prevention programs. Mediators included learning from experience and adjusting to the external environment, while outputs were comprised of program services.
Similar to CBOs that provide HIV/AIDS services, churches vary in organizational structure, capacity to implement health programs, and readiness to address HIV/AIDS-related issues in their communities. Unlike CBOs, however, churches do not exist solely to implement health-related programming; their missions are much broader in scope. Moreover, because a framework did not exist in the literature to inform the development of HIV/AIDS prevention programs in African American churches and FBOs, the research team hypothesized that factors influencing and guiding the provision of these services in churches and FBOs likely differed from those in CBOs.
In January 2006, Project FAITH (Fostering AIDS Initiatives that Heal), a state-wide demonstration project of the South Carolina HIV/AIDS Council (SCHAC), was initiated to provide support to churches and FBOs to develop and implement local HIV/AIDS prevention programs for their congregations and communities. Churches submitted proposals, which were reviewed by a committee of public health professionals and community members, describing their history of and capacity to address HIV/AIDS in their communities, as well as goals and objectives for their locally developed HIV/AIDS prevention programs. As a result, HIV/AIDS prevention programs proposed and ultimately implemented by individual churches varied considerably. Twenty-four churches were funded in the first year of Project FAITH and 34 were funded in the second year; SCHAC, other churches, and local AIDS service organizations provided technical assistance to these churches. A team of evaluators were contracted to lead evaluation efforts, and a financial consultant provided support to each church. Due to the high incidence and prevalence rates of HIV/AIDS among African Americans in South Carolina, African American churches were the primary but not exclusive targets of Project FAITH. While all funded churches in the first 2 years of Project FAITH were Christian Protestant denominations, FBOs of any faith were eligible to apply.
The purpose of this study was to develop a framework to guide the development and implementation of HIV/AIDS prevention programs in African American churches. A qualitative study of Project FAITH guided the development of the framework and a grounded theory approach was used to define inputs, enablers and inhibitors, mediators, and outputs in a faith-based context.
Methods
Data for this study were collected by the evaluators through semi-structured in-depth interviews and focus groups with persons who were directly involved with Project FAITH. Focus groups (n=6) were conducted with a stratified sample of care teams, groups who coordinated the HIV/AIDS prevention programs in their churches, and faith-based technical assistance providers (n=2). In-depth interviews were conducted with a stratified sample of pastors (n=8) and project champions (n=2), individuals who worked at the policy level to secure funding for Project FAITH. Separate interview guides were developed for each group of participants based on evaluation results from the first year of Project FAITH and the extant literature.
Open-ended questions addressed multiple domains regarding program implementation including development of the local intervention, church characteristics, successes and challenges, changes attributed to Project FAITH, stigma, experiences in project implementation, lessons learned, organizational changes, and external influences. All funded churches participated in the evaluation of Project FAITH and were aware that they may be selected for a focus group or pastor interview.
To be eligible for this study, a church must have participated in Project FAITH for at least 1 year. Participants were selected using a stratified purposeful sampling strategy 17 based on region in the state (Upstate, Midlands, or Low Country) and church size, which was categorized as small (250 or fewer members) or large (251 or more members). Following stratification, churches were randomly selected to be invited to participate in the study. Care teams and pastors were selected independently, so a church was eligible for both a care team focus group and pastor interview. All focus group and interview guides were approved by the Institutional Review Board at the University of South Carolina, and each participant completed informed consent prior to participation. Focus groups typically lasted between 1 and 2 h, and interviews lasted between 30 and 60 min. Refreshments were provided for focus group participants only; no additional incentives were used. Project FAITH leadership at SCHAC encouraged care teams and pastors selected for a focus group or interview to participate. Focus groups and interviews were scheduled at times and locations convenient for participants and were conducted between August 2007 and May 2008. All pastors and care teams selected agreed to participate. Each participant took part in only one focus group or interview. All focus groups and interviews were audio-recorded and transcribed verbatim.
Analysis
Analytic categories were adapted from the Collins et al. 16 framework and preset broadly as inputs, enablers and inhibitors, mediators, and outputs to guide the framework development. Concepts that emerged during data analysis informed how each category was ultimately defined to remain true to the grounded theory analysis approach. Enablers and inhibitors replaced catalysts from the Collins et al. 16 model to allow exploration of both categories. A multitiered coding process was used 18 and focused on determining lower-level and higher-level concepts and categories. 19,20 Transcripts were initially coded to identify initial emergent concepts and then loaded into QSR NVivo 8 (QSR International, Cambridge, MA) for data management and further analysis. Constant comparative analysis 19 was conducted throughout the analytic process to ensure that themes remained grounded in the data. Concepts were then grouped by level (individual, organizational, or community).
Data were coded by two independent analysts and then presented to an advisory committee of Project FAITH staff and content experts for review. Analysts worked with the advisory committee to build consensus around coding. After consensus was achieved, a framework was developed and presented to project stakeholders for validation.
Results
Demographic characteristics
All participants were African American. Participants in care team focus groups (n=22) ranged in age from 26 to 82 years (mean age=50 years), and the average length of time served on the care team was 2.3 years. Care team members had been members of their current congregations from 3 to 82 years (mean=25 years). Approximately 82% of care team members were female. The mean age of pastors (n=8) was 52 years, and ranged from 39 to 65 years. The average length of time as a pastor was 25 years, and the average length of time serving their current congregations was 12.5 years. Most pastors were male (87.5%). Two project champions, one male and one female, participated in in-depth interviews. These individuals were considered project champions because of their long-term work at the policy level to secure political support and funding for Project FAITH.
Data analysis defined the inputs, enablers and inhibitors, mediators, and outputs for faith-based HIV/AIDS prevention programs that were part of Project FAITH. Policy and stigma emerged as two environmental contexts that influenced the implementation of HIV/AIDS prevention programs in FBOs that participated in Project FAITH (Table 1). Findings were used to develop a framework for faith-based HIV/AIDS prevention programs. Figure 1 shows that framework.
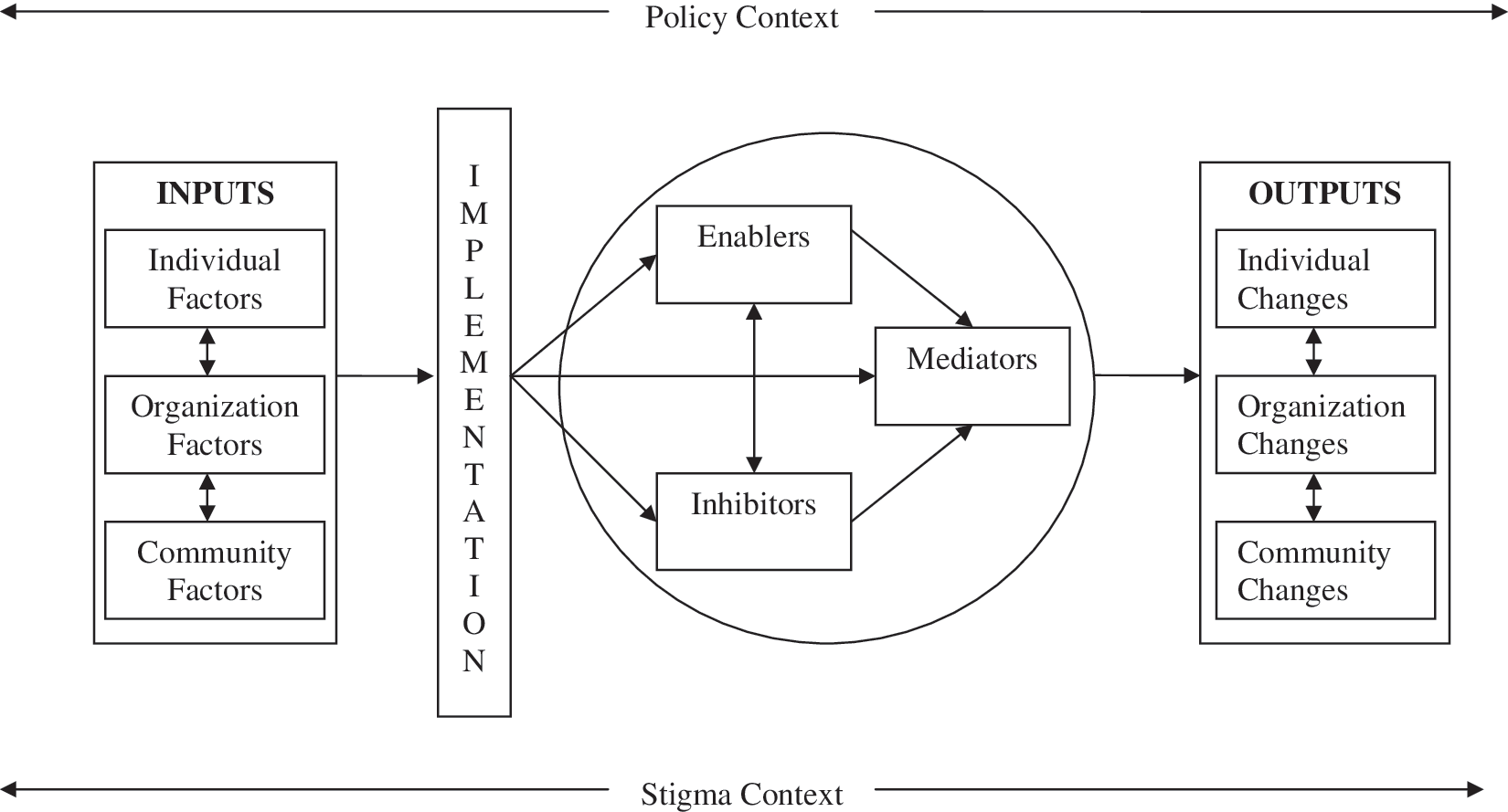
Framework for faith-based HIV/AIDS prevention programs.
FBO, faith-based organization.
Inputs
Inputs were elements present before an HIV/AIDS prevention program was developed or implemented in the church. Individual-level inputs were personal characteristics of HIV/AIDS prevention program leaders, which included: working in a health-related profession, desire to help the community, desire to do more in the church, personal impact of HIV/AIDS, commitment to the church and the fight against HIV, and willingness to take chances.
Many of the individuals who took the lead at Project FAITH churches worked in a health-related profession (e.g., some were nurses, some worked in AIDS service organizations) and had knowledge of the disease and the extent to which it was a problem in their community. One care team member noted, “…it's because I was able to talk about it [HIV/AIDS] more freely,” that she was able to take the lead. Leaders also expressed the desire to help their communities through empowerment or extending outreach and filling the HIV/AIDS prevention gap at their churches; one care team member stated, “We need for communities to be empowered to save ourselves.” Many knew someone living with or who had died from HIV/AIDS and were committed to their churches and HIV/AIDS prevention, so much so, they were willing to take chances and advocate for HIV/AIDS prevention, even when other congregants were resistant. For example, one pastor said, “If you check my record with this church in my 30 years here, I've been first in a lot of things…I try things that are against the grain.”
Organizational level inputs included buy-in, preexisting infrastructure, cues to action, and actions undertaken to facilitate implementation. Buy-in was defined as the level of readiness and individual actions that facilitated the adoption or implementation of the HIV/AIDS prevention program. Leadership buy-in extended beyond the pastor and included buy-in from other church leaders (e.g., deacons and lay leaders), although one care team member observed that, “The pastor has got to be the keystone.” Congregation buy-in was demonstrated through motivation to address HIV/AIDS. One pastor noted, “The congregation themselves, they were ready and motivated, the spirit was right, and their heart was there.” Congregants demonstrated support for the program by continuing to tithe to support the HIV/AIDS prevention program, as summarized by one care team member who stated, “…if they decide they don't like what's happening, they decide not to tithe.”
Preexisting infrastructure was defined as having existing organizational structures (i.e., having the capacity to implement an HIV/AIDS prevention program); a history of addressing health-related issues (e.g., cancer, diabetes, or hypertension); existing resources (including human resources); and participating in existing collaborations with other FBOs or AIDS service organizations. One care team member pointed out, “You need to have infrastructure from a core group of people if you don't have a health committee. That's one of the things that's really important,” while a pastor observed, “I realize there are members of my congregation that have gifts and talents that I cannot touch. So in the areas where I need them, I utilize them.” Regarding collaboration, a care team member stated, “We started with HIV/AIDS through partnerships with other agencies.”
Participants reported that learning about Project FAITH and the associated funding opportunity served as cues to action for them to organize and seek funding. One care team member said, “We would not have come together had it not been for the funding.” Participants also reported that a growing, collective understanding of the need for HIV/AIDS prevention services and general health services functioned as a cue to action in this study. “A need for better health is so paramount here,” stated one care team member.
Specific actions taken by churches to prepare for their faith-based HIV/AIDS programs included participating in preintervention trainings, deciding to start small, and developing clear goals and objectives. In this study, preintervention training was most often the FAITH summit, a half-day workshop led by Project FAITH staff to prepare for the grant making process. Other trainings included those offered by organizations on basic HIV/AIDS information. Participants in this study advised retrospectively that starting small and developing clear goals and objectives were critical to implementing a manageable HIV/AIDS prevention program. A care team member observed that, “Sometimes we have high in the sky ideas, and it's not doable,” while another noted that, “Once we came up with the things we needed, we had to try to narrow them down. That's where goals and objectives came into play.”
The role of the church emerged as a community level input. Participants believed that the trust of the community was vital to providing effective HIV/AIDS prevention programs. One care team member said, “The church has always been a place we can go for information, especially when it came to things like health. It was trusted there.” Another care team member articulated the role of the church as a change agent in the community, “We know [when] the church take[s] an active role, change can occur.”
The presence of inputs prepared each church to begin program implementation. Following the initiation of the program, enablers and inhibitors operated reciprocally to push the program forward or hold the program back. Mediators were the actual process of implementing the program. Enablers, inhibitors, and mediators were presented together in the framework to demonstrate that they occurred simultaneously during program implementation.
Enablers and inhibitors
Enablers were characteristics of individuals and the environment that facilitated the implementation of the faith-based HIV/AIDS prevention program after funding was awarded; inhibitors functioned as barriers to program implementation. At the individual level, participants described those who engaged in program implementation as dedicated, determined, and faithful. One care team member commented, “You can hear it in their voices, there is concern about the programs we're putting together and how we're doing them.”
Most enablers existed at the organizational level and included technical assistance, support of the national level church (denomination), visible leadership support, congregation acceptance, and integration with other programs. Technical assistance needs included both the need for on-going workshops and trainings (e.g., STD/HIV conferences and “HIV 101”) and the need for direct technical assistance to the organization (on topics such as fiscal management and materials development and tailoring). One technical assistance provider noted the importance of “being there to support them, actually supplying information for them, boards, and the stuff that they needed.” Participants articulated that in all cases their national level denomination supported, either actively or passively, their HIV/AIDS prevention initiatives. Visible leadership support of the prevention program was important by building support within the congregation for the HIV/AIDS prevention program. A pastor stated that, “Without a doubt, the driving force behind those sorts of initiatives [HIV/AIDS programs] in our ministry, in our church, is the pastor talking about it, particularly not just to the young people but to the entire congregation.” Similarly, acceptance of the program among congregations was evidenced by their presence at program events, as explained by one pastor, “The people…once they get involved, they see that this [HIV/AIDS] is part of life.” The HIV/AIDS prevention programs were integrated with other programs to make them more acceptable to congregation members. Most often, they were integrated into health fairs or other health ministry activities that covered multiple health topics. One care team member said, “It was fit in with the other health care so people just thought it's another part.”
While inhibitors did not prevent implementation of the HIV/AIDS prevention programs, they acted as barriers to implementation. At the individual level, inhibitors included leadership resistance, competing commitments for program implementers, and apathy. Participants reported that some leaders were resistant to HIV/AIDS prevention programs in their own churches, and they further reported that leaders in other churches did not allow HIV/AIDS prevention programs. A care team member commented, “We have a few deacons…they won't speak out for AIDS,” and another stated that, “In some churches if the pastor doesn't want it, there's nothing getting it.” Competing commitments also emerged as an inhibitor, as many of the same individuals who implemented the HIV/AIDS prevention program served on multiple ministries and had other commitments both within and outside of the church. A technical assistance provider observed, “We didn't have the kind of time that we needed because everybody's doing everything.” Apathy emerged as an inhibitor in two ways: first, some congregation members and program implementers did not want to complete surveys and reporting forms required by Project FAITH, and second, general apathy was characterized by some individuals' unwillingness to hear or talk about HIV/AIDS in a faith setting. A pastor said, “There's very few people really talking about AIDS. You know, no one wants to talk about it.”
Organizational inhibitors emerged as either deficits or congregation resistance. Deficits were defined as the lack of resources or the lack of participation. Participants indicated that although funding was provided by Project FAITH, they often lacked enough funding or worried about future funding. One pastor explained, “…the threat of how and the financial means to do that ministry…even if we wanted to do it, how do we do it with such limited funds?” Further, some participants indicated that other resources, such as transportation, presented a barrier to full implementation. Low participation in some events was reported and affected the motivation of care team members and decreased the reach of the program, as explained by a care team member, “You don't want someone coming in to be a presenter and nobody shows up.” Push-back and lack of awareness of the role of the care team defined congregation resistance. Participants reported that some congregation members did not want HIV/AIDS discussed in their churches and were unable to disassociate HIV/AIDS with sexual behaviors. A care team member observed, “They did not want conversations about HIV at my church…the old guard is still in control.” Many congregation members did not understand the role of the care team and viewed them as groups of HIV-positive persons or homosexuals; “They think I'm HIV-positive,” stated one care team member, while another noted that “I've spoken to some men, but they think if you're part of the care team, then you're gay, you're homosexual.”
Mediators
Mediators were factors that influenced the delivery of the HIV/AIDS prevention program and included process-oriented strategies for implementing programs or increasing the acceptance of the program by the congregation. Like enablers and inhibitors, mediators existed at the individual and organization levels. Concepts that defined individual level mediators were knowledge and modeling of behaviors supportive of HIV-positive persons. Knowledge included individuals' level of knowledge about basic HIV/AIDS facts. Participants reported that many congregation members had low levels of HIV/AIDS knowledge and that their programs were influenced by having to provide basic education. Similarly, congregation members held on to beliefs in myths about HIV/AIDS, particularly concerning how it was transmitted (e.g., drinking after an HIV-positive person, being sneezed on, HIV as a “white, gay” disease, casual contact). One pastor stated that, “…there is misinformation. There are still folks who have not opened their ears to even hear and similarly distanced themselves from wanting to hear.” Participants reported that old myths were difficult to overcome and often challenged the credibility of the program. A care team member noted, “People still thought you could catch it [HIV] through kissing someone, holding hands. And really I thought we had progressed beyond that, but after talking with people, I saw we had not.” Low levels of knowledge about HIV/AIDS and belief in myths were categorized as mediators because they influenced, in many cases, the credibility of the program. Before focusing on HIV prevention skills, programs had to increase HIV/AIDS knowledge and work toward discounting long-held and powerful beliefs in myths in order to be viewed as credible by congregants.
Modeling was a second individual level mediator that emerged. Individual actions of church leadership or lay members included leading by example and outward displays of compassion. Modeling behaviors supportive of HIV/AIDS education or persons living with HIV/AIDS influenced the acceptability of the program and worked to change attitudes toward persons living with HIV/AIDS. One pastor explained, “I'll shake someone by the hands with AIDS just to prove that I can shake your hand. But, you know, a lot of pastors…haven't gotten to that point.”
At the organizational level, mediators emerged into three concepts: the message, keeping the program in a faith-based context, and visibility of HIV-positive persons. The message was defined as crafting the core theme (creating a culturally appropriate theme to resonate with the intended audience), adjusting its communication (tailoring the theme for different audiences, most often gender or age specific audiences), expressing the theme from the pulpit, and focusing on truth. One care team member discussed the importance of being “diplomatic in the choice of words we use,” and another spoke about the importance of learning “the language of the youth.” Participants believed that the power of delivering the message from the pulpit could not be understated and was central to mediating HIV/AIDS prevention in their churches. Further, participants articulated that the message must be straight-forward and focused on the truth (i.e., provide accurate information although it may conflict with long-held beliefs). A care team member summarized, “When our pastor do[es] it from the pulpit…you're really reaching people because whatever the pastor say[s], folks [are] going to take that in.” A technical assistance provider offered, “Let's tell the truth for what it is so we can educate the next generation that's coming up.”
The ability to keep the program grounded in a faith-based context further mediated implementation. A concern expressed by participants was navigating how to discuss sexual behaviors in a church setting. Participants discussed the necessity of using caution and sensitivity; however, they believed that it was possible to discuss sexual behaviors in a church setting. Being open to new ideas at the organization level further defined the faith-context. The openness of congregation members to explore faith-based responses to HIV/AIDS and the use of innovations (e.g., wrapping condoms in paper before distributing them at a health fair) were components of the faith-context. A care team member observed, “A lot of churches struggle between where you draw the line between compassion and endorsing a particular sort of behavior. That's where Christians as a whole struggle…and some churches are still trying to find that balance.” Participants attributed the visibility of an openly HIV-positive person to making congregation members more accepting and influencing attitudes. A technical assistance provider noted the importance of “having someone come in who is HIV-positive to let them see…it's not a matter of how you were infected, it's that you are infected. Let them see the face of AIDS.”
Outputs
Outputs were the tangible or intangible changes in churches or communities that participants attributed to their HIV/AIDS prevention programs. At the individual level, participants reported that congregation members showed an increase in HIV/AIDS-related knowledge, more positive attitudes toward discussing HIV/AIDS and toward HIV-positive people, an increased level of comfort in discussing HIV/AIDS in a faith setting, decreased HIV/AIDS-related stigma, and a desire to know more about HIV/AIDS. A care team member observed, “I think our congregation is more receptive and more understanding and more willing to help. Along with that comes the realization that there are going to be health issues, and some of those health issues may be HIV/AIDS.” Baseline HIV/AIDS related knowledge and stigmatizing attitudes held at Project FAITH churches are reported elsewhere. 21
At the organizational level, outputs emerged as increased capacity in the FBO and increased programming. Increased capacity was defined as organizational empowerment (belief that the organization could do more effective programming), new or altered physical spaces (including designated information areas and care team office spaces), and increased capability to do ministry (beyond HIV/AIDS ministry). One care team member expressed the ability “to think outside the box and also do a lot of things that we had only hoped to do at the beginning.” Increased programming was defined by an increase in the number of participants in HIV/AIDS prevention programming, the development of new programs, and more HIV testing activities provided by Project FAITH churches.
Participants reported that HIV/AIDS-related knowledge and attitudes improved in their communities as well as in their congregations, as summarized by a pastor, “The information has been given to us and we also transferred it to the community.” Furthermore, they reported that new collaborations were formed as a result of Project FAITH; they were able to bring more churches on-board and also formed new collaborations with AIDS service organizations. One pastor pointed out that, “We are getting more churches to collaborate with us.”
Policy and stigma
HIV/AIDS prevention programs in this study existed within an environment characterized by the contexts of policy and stigma. From its inception, Project FAITH was a state-level legislative initiative that resulted from years of advocacy and preparation. Once funded, there was no guarantee that funding would continue for the initiative, and advocacy became an integral task for churches. Participants in this study articulated that legislative policy, particularly funding, affected their programs from inception and continued to affect their programs throughout the Project FAITH implementation process. A project champion noted, “One of the things I've found in this effort…is a lack of sustained effort on the part of people who are concerned. They win a small victory and they think it's over. They don't understand that the process continues.” Participants feared that an abrupt end to funding would derail their efforts for a long time. Support through the legislature worked to increase the legitimacy of the programs at the local level in addition to providing the resources necessary to implement them, as characterized by a program champion, “We have to position ourselves…to compete for scarce dollars every year.”
Participants reported that stigma existed as denial (that HIV/AIDS affects the community), linkage of HIV/AIDS to homosexuality, fear of HIV/AIDS or people living with HIV/AIDS, and blaming an individual for being HIV-positive. A care team member characterized HIV as a “secret still for some people,” while another related it to “don't ask, don't tell.” The linkage to homosexuality further propagated stigma, as characterized by a pastor who said, “If they look like they're gay or something like that, they got to have AIDS.,” while a care team member observed that, “Some people think it's only gay folks getting it.” Fear was a salient part of stigma in this study. One pastor explained, “I've seen the stigma of…hugging, embracing somebody, shaking hands, stand-offish. Those kinds of thing I've seen in people, especially if they know the person is infected.” Similarly, a pastor described the view of someone living with AIDS as “they must have done something wrong.” Participants reported that many congregation members would not discuss or support HIV/AIDS prevention in their FBOs due to stigma.
Discussion
African American churches have a great deal of influence in African American communities, which situates them well to provide locally developed, culturally appropriate HIV/AIDS prevention programs. Similar to previous studies, 5 –8 we found that the church was a trusted organization within the African American community, even when addressing HIV/AIDS. The importance of these findings cannot be overstated; as the epidemic continues to affect African Americans at higher rates than other racial and ethnic groups.
The contexts of policy and stigma that emerged in this study reinforce the need to support African American churches in the provision of long-term sustainable solutions in their communities to address the HIV/AIDS epidemic. At the policy level, community members must rally around issues related to HIV/AIDS in order to influence policy makers. In many communities, policy makers are often unaware of or in denial regarding the extent to which HIV/AIDS affects their constituencies. As leaders of community opinion and action, churches can play a critical role in influencing policy. Thus, churches should focus specific attention on identifying and training their leaders and members to be effective advocates for their communities. Such advocacy efforts could directly affect access to financial resources, which are critical to implementing faith-based HIV/AIDS prevention programs.
HIV/AIDS-related stigma has been observed in various communities, particularly African American communities, 22 –25 and related to religious intensity and the association of AIDS with marginalized, particularly homosexual, individuals. 26 Unsurprisingly, the most salient social context that influenced implementation of HIV/AIDS prevention programs in African American churches in this study was stigma. Participants reported that stigma not only created barriers to or challenges for faith-based HIV/AIDS prevention programs, it was associated with community members' denial that HIV/AIDS existed in their communities. Fear of contracting HIV and of persons living with HIV/AIDS played an important role in manifested stigma in this study, as was the belief that HIV/AIDS was a “homosexual disease.” Churches have the opportunity to address HIV-related stigma, particularly by providing accurate information about HIV/AIDS within their community and dispelling myths. Messages from the pulpit, coupled with changes in the physical environment like bulletin boards, bulletin inserts, and information pamphlets, are necessary first steps to reduce HIV/AIDS-related stigma in faith settings. However, churches must also create an environment of understanding and acceptance where sexual minority persons are treated as valued members of the church and community, rather than as outsiders who “aren't to be talked about.”
Findings from this study demonstrated that having dedicated individuals with previous HIV/AIDS experience and the desire to help their church and community were essential to the implementation of faith-based HIV/AIDS prevention programs. Further, both religious leaders and congregation members needed to buy-in and contribute to the program for it to be successful. Having a preexisting infrastructure, such as a health ministry, into which an HIV/AIDS prevention program could fit was important, as were opportunities for churches and care teams to engage in technical assistance and skills building.
While these inputs were similar to those of community based organizations, 16 they are inherently different because buy-in from both the congregation and church leadership had to be achieved prior to the adoption of the program. Furthermore, most churches had little or no experience in addressing HIV/AIDS and care teams that led HIV/AIDS prevention programs were primarily composed of volunteers rather than paid staff members, unlike at CBOs. Moreover, the broad mission of churches at times made it difficult to focus on a discrete health issue, such as HIV/AIDS. Therefore, the adoption and implementation of future HIV/AIDS prevention programs must be undertaken with care and respect for the church as an institution.
An examination of the enablers, inhibitors, and mediators expressed by participants in this study provides some understanding of how HIV/AIDS prevention programs operate in faith-based settings. During the implementation phase of a church-based HIV/AIDS prevention project, enablers were critical to ensure the program functioned effectively and worked to counteract inhibitors to implementation. We found that inspiring, passionate, dedicated people had to be present for the program to thrive. Organizational enablers such as visible leadership support, congregation acceptance, program integration, and the availability of financial support fostered program implementation. Although we cannot determine the degree to which support from the national-level denomination was necessary, all churches in our study indicated that they either had active or passive support from their national offices. HIV/AIDS prevention program planners should consider strategies for engaging churches at the national denomination level.
As expected, apathy regarding HIV/AIDS and denial that HIV/AIDS existed within communities were reported among some congregants and leaders. Consistent with previous research, faith-based HIV/AIDS prevention programs must receive technical assistance and capacity building at the organizational level. 27,28 Technical assistance should include training for both formal and to lay leaders (e.g., ministers, care team members). Furthermore, technical assistance should focus on increasing the HIV/AIDS-related knowledge of those in leadership roles (e.g., “HIV 101” or “HIV and the Law” trainings) and include skills for capacity building at the organizational level (e.g., grant management, program planning, implementation, and evaluation).
Mediators, or primary strategies adopted by churches to address HIV/AIDS, and build acceptance of it. Strategies included educational programs addressing myths and modeling supportive behaviors toward HIV-positive individuals. In particular, culturally-specific and tailored messages for various audiences were necessary for programs to be accepted, and religious and program leaders needed access to accurate HIV/AIDS information and messages grounded in theology. These findings were consistent with other faith-based HIV/AIDS projects regarding the willingness of religious leaders to adopt creative strategies grounded in the guiding principles of their respective faiths. 27 Further, findings from this study demonstrate that faith- and community-based organizations experience similar mediators, which Collins et al. characterized as learning from experience and adjusting to the external environment. 16 While the CBO model included structural variables as mediators, our findings indicated that structural variables (namely policy and stigma) were particularly salient in the faith environment and should be categorized independently.
Outputs that resulted from Project FAITH may help other FBOs identify the types of activities that can be accomplished successfully and plan achievable goals and objectives for their programs. Participants in this study believed that their HIV/AIDS prevention programs were successful in increasing knowledge, changing attitudes about and comfort discussing HIV/AIDS, and decreasing stigma in their churches. Churches also increased their ability to provide HIV testing, which has been identified as an area of emphasis in HIV prevention. 4 Diffusion of program outcomes to the larger community was another outcome reported by Project FAITH churches, which affirms the reach of the church into the larger community.
The framework presented here is the first to explain the process of implementing HIV/AIDS prevention programs in African American churches, based upon the experiences of churches participating in Project FAITH. Thus, there are several limitations to this framework. First, findings from this study are limited to churches that self-selected to participate in both Project FAITH and this study. Churches in this study already had ministries to address HIV/AIDS in some capacity. Therefore, they may be different from churches that have not actively addressed HIV/AIDS in their congregations or communities. The framework presented here reflects the experiences of African American, Christian, protestant denominations in South Carolina and may not be generalizable to non-Christian or non-African American FBOs or FBOs in regions other than the Southern United States. Future research should investigate the applicability of this framework in FBOs of non-Christian faiths, in other regions of the United States, and whose membership consists of different races or ethnicities.
Regardless of its limitations, we believe that this framework may be useful to churches and FBOs, as well as CBOs and public health agencies interested in working with FBOs, to develop and implement faith-based HIV/AIDS prevention programs. In particular, the framework calls for the identification of individuals (members of the congregation and church leadership) who are passionate about and devoted to addressing HIV/AIDS, and provides specific mechanisms (i.e., health ministries) through which these individuals can organize, strategies for HIV/AIDS implementation, and areas of technical assistance and capacity building to maximize effectiveness of such efforts.
Footnotes
Acknowledgement
This study was based on a project funded by the South Carolina General Assembly.
Author Disclosure Statement
No competing financial interests exist.