
Abstract
Reflecting trends in health care delivery, pharmacy practice has shifted from a drug-specific to a patient-centered model of care, aimed at improving the quality of patient care and reducing health care costs. In this article, we outline a theoretical model of patient-centered pharmacy services (PCPS), based on in-depth, qualitative interviews with a purposive sample of 28 pharmacists providing care to HIV-infected patients in specialty, semispecialty, and nonspecialty pharmacy settings. Data analysis was an interactive process informed by pharmacists' interviews and a review of the general literature on patient centered care, including Medication Therapy Management (MTM) services. Our main finding was that the current models of pharmacy services, including MTM, do not capture the range of pharmacy services in excess of mandated drug dispensing services. In this article, we propose a theoretical PCPS model that reflects the actual services pharmacists provide. The model includes five elements: (1) addressing patients as whole, contextualized persons; (2) customizing interventions to unique patient circumstances; (3) empowering patients to take responsibility for their own health care; (4) collaborating with clinical and nonclinical providers to address patient needs; and (5) developing sustained relationships with patients. The overarching goal of PCPS is to empower patients' to take responsibility for their own health care and self-manage their HIV-infection. Our findings provide the foundation for future studies regarding how widespread these practices are in diverse community settings, the validity of the proposed PCPS model, the potential for standardizing pharmacist practices, and the feasibility of a PCPS framework to reimburse pharmacists services.
Introduction
T
Patient-centered care (PCC) considers the patient as a unique and whole person with biological, psychological, and social needs, rather than as a cluster of diseases. 4 In providing patient-centered care, providers listen to and address patient concerns, respect patients' values, and have compassion. 4 Through direct response to each patient's concerns, PCC aims to empower the patient through shared decision-making, with the goal of improved quality of care, reduced cost of care, increased satisfaction and consistency of care among providers, and humanized and strengthened professional practice. 2,4,5 In short, PCC presents an individualized rather than standardized model of health care delivery, with continued emphasis on evidence-based practice. 2,3,6
PCC works best in an integrated health care system, which facilitates shared responsibility among patients and providers, including pharmacists. 1,5,7,8 Studies have shown that pharmacist involvement in patient care can improve the quality of care that patients receive and optimize patient health outcomes. 9 –16 Pharmacists can implement evidence-based practices to prevent medication errors and adverse drug events, including medication reconciliation of prescription drug lists and comprehensive review of prescription and non-prescription medications. 1,17 Pharmacist interventions that optimize complex regimens, implement adherence programs, and recommend appropriate and cost-effective therapies, can save money on unnecessary medications; prevent avoidable hospitalizations, physician visits and other interventions; and save patients needless suffering. 8,18 –20
Reflecting trends within health care delivery more generally, PCC has emerged as a key principle within pharmacy practice as well. PCC in pharmacy practice traces its root to patient counseling services mandated in the Omnibus Reconciliation Act of 1990 (OBRA ’90) for all Medicaid and Medicare beneficiaries, and most states for all prescriptions. 21,22 PCC within pharmaceutical care involves a transition to a responsive pharmacy practice model that would address a great unmet need for safe and effective drug therapy. 5,7,8 A PCC model of pharmaceutical care marks a shift in pharmacy practice from solely dispensing products to providing patient-centered care that focuses on optimal drug therapy and medication safety. 7
Since 1990, the pharmacy patient care model has expanded to focus on the management of a specific disease state (disease management model), and in recent years, Medication Therapy Management (MTM) services. Although pharmacists in integrated health care systems have provided pharmaceutical care services since 1998, the expansion of pharmacy services began after 2006 when a provision in the Medicare Prescription Drug Improvement and Modernization Act allowed reimbursement of MTM services. 23 MTM is a model of patient care that incorporates techniques of patient counseling and disease management, in an environment of collaboration between patients, pharmacists and other health care providers to achieve appropriate therapeutic goals for the patient. 21,24,25 In providing MTM services, the pharmacist takes responsibility for the prevention, identification and solution of drug-related problems, and is accountable for providing high-quality patient care. 7,21
The expansion of patient-centered services within pharmacy settings has the potential to benefit HIV-infected persons in particular. For many HIV-infected patients, long-term sustained adherence to antiretroviral drugs is a challenge, with adherence declining over time as symptoms diminish and side effects increase. 9 As HIV-infected patients live longer due to improved antiretroviral medications (ARVs), they are more susceptible to other chronic conditions, such as diabetes and heart disease. HIV and age-related comorbidities compound the problems of adherence related to managing complex regimens from multiple providers, and increase the likelihood of adverse drug events that can lead to expensive hospitalizations and death. 8,26,27 Pharmacists experience in disease management of other chronic conditions and the delivery of MTM services can inform the provision of patient-centered services for HIV-infected patients.
Despite evidence from pilot studies that pharmacists' interventions promote adherence to ARVs, little is known about the nature of these services and interventions in community pharmacy settings. To understand pharmacists' patient-centered practices, we interviewed 28 pharmacists working in diverse pharmacy settings. We explored the range of pharmacy services and interventions with HIV-infected patients in different pharmacy settings. Based on pharmacists' interviews and a review of the literature on patient centered care and MTM services, we developed a model of patient-centered pharmacy services (PCPS). In this article, we provide the theoretical and empirical framework of the model, and then highlight policy implications and areas for further research.
Methods
Recruitment
We used purposive sampling methods to identify three pharmacy organizations (two retail-chain pharmacy organizations and one specialty-only pharmacy organization) in the midwestern United States. The retail-chain pharmacy organization had specialty-only, semispecialty, and nonspecialty pharmacies. Specialty-only pharmacies serve a narrow range of patients with chronic conditions that take expensive drugs, require intensive care, and are among the most expensive to treat. 28 Semispecialty pharmacies deal with both specialty and regular drugs, while nonspecialty pharmacies fill regular prescriptions that do not require specialized administration.
The specialty-only, semispecialty, and nonspecialty pharmacies represent the range of community pharmacy settings where HIV-infected patients fill their antiretroviral medications.
We recruited 28 pharmacists and pharmacy managers working in specialty, semispecialty, and nonspecialty pharmacies, to identify their procedures for providing care to HIV-infected patients at different stages of treatment including, newly diagnosed, those stabilized on therapy, and those struggling with adherence. Participants who completed the interview were given a small gift to compensate them for their time and contribution to the study. The study procedures were reviewed and approved by the Medical College of Wisconsin's Institutional Review Board.
We sought permission for the study by contacting the corporate office for each pharmacy organization. One retail-chain pharmacy organization declined to participate in the study. We proceeded with two pharmacy organizations (one specialty-only pharmacy and one retail-chain pharmacy). We identified four states in the midwestern region for the study based on the distribution of the two organizations' pharmacy networks and the HIV-infected population. We contacted the District Supervisors in charge of each metropolitan city who identified the pharmacies for the study, and provided us with the contact information of the pharmacy managers.
We then initiated contact with and invited each pharmacy manager to participate in the study. We conducted a telephone screening to ensure that participating pharmacies met eligibility criteria (i.e., pharmacy filled prescriptions for HIV-infected patients). The managers were also asked to provide the name of one pharmacist serving HIV-infected patients. We contacted each pharmacist, and invited them to participate in the study. All the managers and pharmacists contacted met the study eligibility criteria (i.e., were licensed pharmacists and provided services to HIV-infected patients) and consented to participate in the study.
We conducted pilot interviews at both pharmacy organizations in August 2009. The objective of the pilot study was to test the appropriateness of the interview questions and refine the final interview guide. The final phase of the study began in September 2009 and ended in October 2009. Each manager and pharmacist was interviewed individually at his/her pharmacy location. We asked pharmacists to describe their procedures and the services they provided in general, and did not ask pharmacists to say “yes” or “no” to each specific practice. We covered the following topics in the interviews: barriers to adherence from their perspective, how they addressed these barriers, other strategies they used to promote patient adherence, and the facilitators and challenges they faced while promoting adherence to antiretroviral medications. We also asked managers to provide general information on their pharmacy and patient demographics. The majority of pharmacists were Caucasian (26). Pharmacists were equally divided across gender, position, and pharmacy practice settings. More than half of the pharmacists interviewed (16) had over 5 years of post licensure experience. Pharmacist characteristics are summarized in Table 1.
Data analysis
Interview transcripts were imported into MAXQDA (Verbi Software Version 10, Marburg Germany), a qualitative software program for text-based data management and analysis. Analysis was conducted in multiple stages. First, all 28 transcripts were read and coded to identify broad themes related to pharmacists' procedures for providing care to HIV-infected patients in a typical visit. After identifying these broad themes, we reviewed the literature on patient-centered care models in general, and the pharmacy literature on patient counseling, disease management, and MTM in particular to identify additional elements of patient-centered care. In categorizing patient-centered pharmacy services, we made a distinction between pharmacy services and pharmacist services. Pharmacy services are provided by an organization or institution and include activities associated with filling a prescription and not direct patient care. 25 By contrast, pharmacist services include clinical interactions between a pharmacist and patient, such as patient education and drug regimen review. 25 A final coding scheme was then developed that combined patient-centered services mentioned by study participants with those identified in the pharmacy literature. Then, through an iterative process of analyzing interview transcripts and reviewing the related literature, we developed a model of PCPS. The goal of our analysis was to identify the key elements of a general model of PCPS in pharmacy settings. Therefore, our analysis did not explore differences in PCPS delivery in the various pharmacy settings.
Results
All 28 pharmacists and pharmacy manager interviews were conducted by the first author and took between 40 and 100 min. While most pharmacists (61%) reported dealing with specialty patients (HIV, oncology, and organ transplant), only 36% of pharmacists identified HIV as constituting the majority of their business. In terms of patient ethnicities, 40% of the pharmacists reported that the majority of their patients were Caucasian; 33% had mostly minorities, and 27% had racially diverse patient populations. Most of the pharmacists (75%) provided care to HIV-infected patients of low socioeconomic status and on public health insurance.
We identified five elements of patient-centered pharmacy services: (1) addressing patients as whole, contextualized persons; (2) customizing interventions to unique patient circumstances; (3) empowering patients to take responsibility for their own health care; (4) collaborating with clinical and nonclinical providers to address patient needs; and (5) developing sustained relationships with patients. While pharmacists in specialty and semispecialty settings tended to provide more services than those in nonspecialty settings, no pharmacists interviewed provided the entire range of services that make up the PCPS model.
Below, we outline each of these elements from a theoretical perspective, highlight the tools and strategies pharmacists used to achieve these goals, and then provide an empirical framework to operationalize PCPS in practice. The theoretical and empirical PCPS model is summarized in Fig. 1.
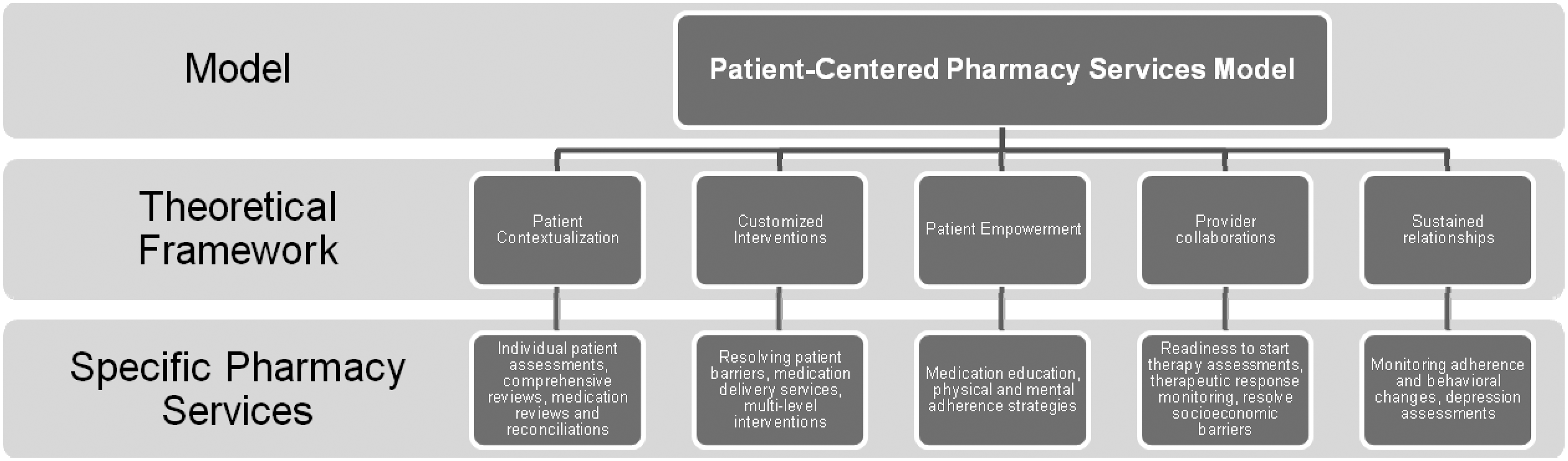
The patient-centered pharmacy services model.
Element #1: Identify patient's contextual factors
Contextualization is the process of identifying individual circumstances in which people experience health and illness, including socioeconomic and psychological factors that can dominate, and in many cases overshadow, their health care needs. 29 –31 Socioeconomic and environmental factors include income, general and health literacy, lifestyle, social support network, and housing environment that may influence adherence to therapy. Psychological factors include mental health comorbidities (anxiety, depression) that can affect a persons' willingness and ability to confront their HIV diagnosis, and cope with their HIV-status and the chronic, lifelong demands of therapy. 32,33 Contextualizing patients can help identify multiple risk factors for nonadherence in order to prioritize interventions and services to particular patient circumstances.
Pharmacists used a range of strategies to understand the social contexts of their patients and the potential implications for medication adherence. These strategies reflected both pharmacy setting and whether a patient was newly diagnosed with HIV or stabilized on ARV therapy. Pharmacists conducted individual patient assessments and comprehensive reviews at the start of therapy to understand patients' individual circumstances. Many pharmacists reported asking nonjudgmental, open-ended questions instead of general questions. In particular, pharmacists reported not asking patients the question “Do you have any questions for the pharmacist?” Noting that patients may not know the right questions to ask, pharmacists reported asking specific questions such as whether they were experiencing specific side effects associated with a medication they were taking, their daily routine and how they were taking their medication, and the number of doses missed in the previous week. Pharmacists used information from these assessments to develop intervention strategies to address patient adherence issues.
In practice, many pharmacists used a proactive approach to anticipate, identify, and resolve adherence barriers before a newly diagnosed patient began ARVs treatment: When there is a patient that is new to meds, we will go up to the clinic and counsel the patient. We will be looking at all of the different barriers to adherence. So we will ask people about jobs: Is there anything about the job that might include certain drugs to be on. Lifestyle issues: Are they homeless? Do they have a refrigerator? How many people do you live with know your status? Questions about depression, questions about adherence to other regimens. We are trying to get a picture of the patient and do everything in our power to make sure that the regimen that is designed is going to work for that patient. [Pharmacy Manager 28 years]
In addition to eliciting patients' social context through these assessments, pharmacists also recognized that contextualizing patients required understanding their medical history more broadly, including past and current medication history. In addition to conducting a drug utilization of current medications on file, a few pharmacists reported reviewing patients' physical medication inventory to identify expired and contraindicated medications: We do medication reconciliation where we have patients bring in all of their meds, over the counter and herbals. Whatever they are taking, we want it all in. We want to be able to sit down with a patient and go through their medications. We have found that patients don't realize that they may be taking something that may be contraindicated with their antiretrovirals. They may have duplicate medications, all sorts of stuff. You never know until you see it all together. [Pharmacy Manager 28 years]
Patients who take numerous medications can get confused about which ones to take and in what order. Pharmacists can enhance adherence by helping patients identify the medications they should take and plan their medication dosing schedule. Finally, pharmacist medication review and reconciliation activities that identify expired and contraindicated drugs can prevent medication errors and adverse drug events.
Element #2: Customize interventions to unique patient circumstances
A patient-centered approach to care identifies and incorporates both biomedical and contextual issues during patient encounters to develop an appropriate treatment plan. 30 Knowing the patient as a person and incorporating the patient's illness experience and the psychosocial context is part of optimal diagnosis and treatment of his/her disease, and contributes to the healing process. 30,34 Pharmacists customized their interventions to accommodate each patient's unique circumstances and lifestyle by using information from comprehensive assessments and by understanding the context of HIV within their lives.
Many HIV-infected patients face multiple barriers to adherence, and therefore require a multidimensional approach to providing care. In one extreme case, a pharmacy manager with nine years experience described how he addressed multiple issues faced by an uninsured patient who had recently relocated, lacked stable housing, had not received care from a HIV physician, and did not have recent lab tests. The pharmacist referred the patient to an HIV physician, helped him apply for Medicaid, advanced him ARVs at no cost, and loaned him a cooler to store his medications.
Specialty and semispecialty pharmacies typically provide medication delivery services to a patient's location of choice (home, local pharmacy). However, some patients may not get their medication on time. One pharmacist for example described a situation in which he was able to abruptly leave a meeting in order to get medications to a patient: He wasn't able to come and get his medications during the day. I was in a meeting, it was 7:30 at night and I was talking back and forth to him, stepping out of the meeting occasionally to talk to him. Finally I just left the meeting, came down to the pharmacy, transferred his prescription from another pharmacy, filled it for him, and then drove it to his house and handed him the medication. Since that day that patient has been so grateful to us and does not want to go to any other pharmacy partly because of that effort I made. I didn't care what I was doing personally at that moment; all I cared about was that patient. [Pharmacy manager 2 years]
This pharmacist felt that making sure the patient had his medications was of utmost importance, even though it inconvenienced him. As a result, the pharmacist was able to win the patients' trust and loyalty, and may have made a difference in that patient's adherence to therapy.
Another pharmacy manager with 3 years experience chose to provide her patients with information on other medical services instead of referring them to a toll free information hotline. The pharmacy manager considered voice-activated phone service too impersonal, and felt that she would serve her patients better by directly providing the information they needed. An important dimension of the pharmacists' ability to provide patients with customized interventions are corporate policies and workplaces that enable pharmacists to quickly respond to individual patient needs.
Element #3: Empowering patients to take responsibility for their own health care
Empowerment is a process that recognizes an individual's ability to meet his or her own needs, solve his or her own problems, and mobilize personal and environmental resources to promote self-efficacy, assert control, and support for his or her own health. 31 In particular, providers' ability to deliver information about antiretroviral medications, understand the problems patients face when taking medications, and help them solve these problems has been shown to increase the odds of patient adherence by 25%. 35 Promoting self-management of patients with chronic illness can change health behaviors, improve health outcomes and result in fewer hospitalizations. 36 Pharmacists empowered patients to manage their own therapy by providing them with medication-specific education, teaching them mental and physical adherence strategies, and equipping them with adherence tools. Pharmacists identified patient education as a key tool of empowerment.
In general, pharmacists conduct individualized, medication-specific education for patients starting therapy, changing therapy, and those who had problems adhering to therapy. Many pharmacists tailored the scope and detail of patient education based on their assessment of patients' knowledge about HIV infection and ARVs. Many pharmacists thought HIV physicians adequately educated their patients. For these patients who did not require comprehensive medication education, pharmacists focused their efforts on filling gaps in patient knowledge and reinforcing adherence messages received from other providers. Depending on patient knowledge and literacy levels, education activities ranged from simple instructions on how and when to take medications to more comprehensive education on HIV disease management. Comprehensive medication education included the following topics: the purpose of each medication, how and when best to take it, special storage instructions, the common side effects associated with the drug and their expected duration, how to manage side effects using over-the-counter medications and nutrition, when to call the doctor, the importance of adherence and its relationship with drug resistance and clinical outcomes (e.g., CD4+ cell counts). Other empowerment strategies included helping patients identify places to visibly store medications so they would remember to take them, establishing a medication schedule so that patients took the medication at the same time each day (such as just before a particular television show), providing adherence tools (timers and pill organizers), and enrolling patients in automatic refill programs.
One pharmacist described the importance of combining medication education with adherence tools to promote patient self-efficacy in HIV-infection management: A patient was taking their medications wrong because they just didn't understand the directions on the bottles. The patient got started on Prezista, Norvir and Truvada a month and a half ago. He wanted his Truvada refilled but not the other two. So I asked him, “What is going on? Why are you doing this?” He was forgetting to take one of his Prezista because he was taking one in the morning and one at night, instead of both in the morning. So he had extra pills of his Prezista and didn't understand why. The Norvir he was keeping in the fridge and was forgetting to take it. He wasn't using a pillbox and he wasn't remembering to take the Norvir. So I quickly explained to him, “Ok, the Norvir is very important. This is what it's doing for you. It's ok to take it with Truvada. This is designed to be once a day regimen. The Norvir can be out of the fridge for a month. Just make sure it's in a stable environment.” I sent him a pillbox this morning and got him on track with his medications. [Pharmacist 1 year]
Because this patient did not know that Norvir® (Abbott Laboratories, Abbott Park, IL) can be stored at room temperature, he kept it refrigerated, and thus physically separated from his other medications. In turn, he repeatedly failed to take Norvir®. The pharmacist identified the patient's suboptimal therapy and educated him on how to take his medications.
Empowerment involves a combination of strategies that include medication education, and physical and mental adherence reminder tools to enhance patient self-efficacy in treatment.
Element #4: Collaborate with clinical and nonclinical providers to address patient needs
Collaboration among providers facilitates coordination of care and ensures that patients have access to the resources they need in a timely manner. 37 An important aspect of collaboration is sharing patients' medical history among providers. 37,38 Interventions that coordinate a patient's care can enhance that patient's experience with the health care system, improve the quality of care and health outcomes, and reduce the cost of care, especially among those patients with many medical problems and health care providers. 37
To maximize adherence, pharmacists collaborated with clinical providers (e.g., HIV specialists and nurses), and nonclinical providers (e.g., case managers). A few pharmacists reported working with HIV physicians to conduct readiness to start therapy assessments for newly diagnosed HIV-infected patients, help identify appropriate ARV regimens, and monitor therapeutic response to therapy for patients struggling with adherence.
The few pharmacists with access to laboratory results monitored patients' adherence and therapeutic outcomes, including CD4+ cell counts, and kidney and liver functions. One pharmacist made therapeutic recommendations that may have prevented a potential medication error and averted an adverse drug event: If I know that they are not doing well adherence-wise, I go and check their labs. For most of my patients I have the luxury that I can go double check. I mean there are things like clinic interventions we get to do. Like for instance, two different patients this last week got their dose adjusted for their Truvada for the renal issue but they did not dose-adjust anything else. So we are going through their profile, getting their labs, calculating out their creatinine clearance and then having to go [to the physician] and say, “You forgot this and this and this. We should probably dose [this medication] down if there is a kidney issue.” [Pharmacy Manager 11 years]
Pharmacists also reported working with nonclinical providers to address insurance-related paperwork, housing issues, and social support for isolated patients. One pharmacist we interviewed described the importance of communication between healthcare providers: Because the same patient may tell a different story to me, a different story to the peer educator, a different story to their case manager, and a different story to the doctor. So between all of us, we can try and figure out what is going on with the patient. [Pharmacist 3 years]
Provider collaborations are important in identifying problems that the patient may be experiencing, as well as facilitating patient access to needed services that affect treatment: We have the [local AIDS service organization] that we work with. They are the largest case manager group [in the city] and so we refer our patients to them. If there is a medication that isn't covered, we will involve Ryan White. We provide a direct connection—instead of going through the front door with all of these programs, I know people I can call and say “Hey, my patient is so and so, and their insurance isn't active.” It will be taken care of that day rather than 5 or 6 days later. So it's more of behind the scenes stuff. [Manager 5 years]
As noted earlier, pharmacists' ability to communicate directly with other providers' facilitated continuity of care through information flow, and helped patients navigate the health care system.
Element #5: Sustain relationships with patients
Patient–provider relationships can directly influence patients' access to medical providers and indirectly affect their willingness to adhere to their medications. Good patient–provider relationships characterized by a caring attitude, responsiveness, access, and respect can foster patient trust, influence adherence to treatment and lead to better clinical results and higher patient satisfaction. 33,35,39
Many pharmacists monitored patient adherence and response to therapy on a regular basis. Monitoring activities ranged in intensity depending on the duration of time the patient was on treatment. For newly diagnosed HIV-infected patients, monitoring began within a few days of starting treatment: Just because they leave here with their medication doesn't mean that they will start it that day. So we call them 5 to 7 days later, just to see if they have started their medications or are having side effects that we can help them through. Then we will call them again in a week and kind of review the same things, and then 2 weeks after that. Then it's month end when they usually come back for follow up with their doctor. [Pharmacist 2 years]
For patients already stabilized on therapy, monitoring was done during routine monthly phone calls to set up medication refill deliveries.
Many pharmacists reported that their patients had been coming to the pharmacy for years. These pharmacists had developed personal friendships with their patients and knew their name, family, work and housing situation, and other important information. These personal friendships enabled pharmacists to monitor the patient's behavioral changes: The more you get to know [the patient], even if they are not admitting it, you can often tell changes in their mood and if they seem really down. I'm not afraid to ask them “Are you depressed?” “Do you feel like you are hearing stuff?” I've actually had to do a suicide assessment in the lobby because the patient was obviously so bad. [Pharmacy Manager 11 years]
This pharmacist had a personal relationship with his patient that allowed him to ask personal questions, and personal knowledge of the patient to identify behavioral changes that suggested the patient might be depressed.
Discussion
Our study findings confirm observations in the literature that pharmacists routinely provide services that are above and beyond patient counseling services mandated by law, and Medication Therapy Management (MTM) services for Medicare Part D beneficiaries. We defined these above and beyond services as patient-centered pharmacy services (PCPS). We presented a model of PCPS that has similarities and differences with the MTM model. At the core, providing PCPS involves contextualizing the patient as a whole person and not a cluster of diseases, and empowering them to take responsibility for their own health care by intervening to prevent and resolve adherence barriers and self-manage their HIV infection. Like MTM, the basket of patient-centered pharmacy services includes comprehensive patient assessments for newly diagnosed HIV-infected patients at the start of therapy, monitoring adherence for patients stabilized on therapy, and interventions and referrals to other providers for patients struggling with adherence.
The theoretical PCPS model developed and presented in this paper differs from the MTM model in several ways. First, the two models are conceptually different. The PCPS model we propose places the patient at the center of service provision. By contrast, MTM places the patients' medication regimens at the center. Second, PCPS are potentially available to all patients and are provided on an as-needed basis. In contrast MTM services are provided under contractual relationships with third-party payers (e.g., insurance companies, employers) that specify beneficiary eligibility criteria (e.g., multiple chronic conditions, high prescription drug expenditures). Third, while the PCPS model we outlined did not incorporate the documentation of patients' therapeutic goals, the MTM service model requires pharmacists to help patients set therapeutic goals and document medication-related action plans (MAPs).
Each element of the theoretical PCPS model has specific pharmacy practices including conducting comprehensive reviews, individual patient assessments and medication reconciliation, providing medication delivery services and conducting multilevel interventions, patient education about their medications, physical and mental adherence strategies, readiness-to-start therapy assessments, therapeutic response monitoring, case manager referrals for insurance-related issues, and monthly monitoring phone calls. As noted earlier, these pharmacy practices have proven efficacy in promoting adherence to treatment.
As presented, the PCPS model may not apply to all pharmacists or pharmacy settings. Some of the examples provided in the PCPS model reflect an extreme level of pharmacist involvement in patient care. Not all pharmacists provided services in the same breadth (i.e., range of services provided) and intensity (i.e., amount of time spent with each patient). While many pharmacists reported monitoring adherence and addressing barriers, only a handful conducted comprehensive assessments for newly diagnosed HIV-infected patients. Pharmacists cited various reasons for not providing services including lack of time, not enough staffing, and not being reimbursed for providing these services. Our finding that provision of PCPS is variable across pharmacy settings is consistent with evaluations of MTM services. 27
Our study findings have important policy implications. First, pharmacists can play an important role in promoting access to care by resolving barriers, monitoring patients' response to therapy, and facilitating continuity of care through collaborations with other providers. Pharmacists can play a central role in improving the health outcomes of HIV-infected patients struggling to adhere to therapy, through customized interventions and collaborations with other providers. Second, PCPS can be targeted to HIV-infected patients depending on health care needs, and applied in community pharmacy settings with varying degree of breadth and intensity. In busy, nonspecialty settings where pharmacists are time constrained, PCPS may be limited to trying to identify and focus on poorly adherent patients and referring them to a specialty pharmacy. Third, in order to review patient's medication regimen for appropriateness and safety, pharmacists need access to the patient's complete medication history and clinical outcomes (CD4+ counts, viral load). Many pharmacists reported they did not have access to this important patient information. Fourth, PCPS is potentially a time consuming process that would require service provision that exceeds drug dispensing. Without specific reimbursement for nondispensing services, there may be no incentive to spend additional time providing them. 3,40 As noted above, this finding has implications particularly for patients receiving care in settings where pharmacists are the most time-constrained.
Our proposed PCPS framework has implications for the design of quality performance metric measures required to implement incentive-based reimbursement initiatives such as Pay-for-Performance. These incentive-based reimbursement initiatives require that providers take greater responsibility for the quality of care, and are rewarded for actions that enhance patient outcomes. 3,37,41 In order to implement an incentive-based reimbursement system, performance metrics are needed to track outcomes, evaluate effectiveness, identify quality gaps and areas for improvement, and allow for comparison of performance across pharmacy settings. 37,41 -43 Applying value-based pay-for-performance would align pharmacy reimbursement to evidence-based practices, including monitoring phone visits and medication reconciliation activities that prevent medication errors and adverse drug events. 37,42
Our study findings should be interpreted in light of the following limitations. The PCPS model we describe is meant to provide a lens for understanding pharmacy practice more holistically, and is not intended to be a set of practices that each pharmacist can and will be able to implement. As noted earlier, some pharmacists do not have the resources to provide the level of care required by the PCPS model. In addition, we did not observe pharmacists' procedures and interactions with HIV-infected patients to confirm that these services were provided as reported. Our findings are based on self-reports by pharmacists and may have self-presentation bias. As in other studies that rely on self-report of past behavior, poor recall of procedures and processes may bias study findings. Last, the proposed theoretical PCPS model is based on findings from a small purposive sample of pharmacists. Before the PCPS model can be considered an established model, more quantitative studies are needed to examine the representativeness of pharmacists' practices that constitute the model.
Conclusion
We found that pharmacists are providing a wide range of services to promote antiretroviral adherence among HIV-infected patients on a routine basis. However, we do not know the extent to which these services are being provided, and the factors associated with the provision and non-provision of these services. Because of the proliferation of patient-centered pharmacy services in community pharmacy settings since Medicare Part D was implemented in 2006, it is important to understand whether these services contribute to high-quality care. 27,44
As more pharmacists provide patient-centered pharmacy services, there is a need to address the variation in the range of these services and the inability to measure pharmacist practices and patient outcomes. As noted by others, more research is needed to identify pharmacy quality performance metrics that can be used for standardizing patient-centered pharmacy services, assess the impact of these services on patient outcomes and health care costs, and potentially justify reimbursement by third-party payers. 45 Other health care professions have developed quality improvement initiatives, measurements, and report cards that the pharmacy profession can use to model their own pay-for-performance initiatives. 40,41,46 Standardization and consistent application of patient-centered pharmacy services will allow stakeholders to evaluate the quality of pharmacy services, and cement pharmacists' leadership in promoting patients' safe and effective medication use.
Footnotes
Author Disclosure Statement
No competing financial interests exist.