
Abstract
Women are often underrepresented in randomized clinical trials (RCT) of HIV-1 drugs. As a result, determining whether women have different virologic outcomes compared to men is not always possible because the gender-related analyses usually lack statistical power. To address this important public health concern, the Food and Drug Administration's (FDA) Division of Antiviral Products (DAVP) created a database including 20,328 HIV-positive subjects from 40 RCTs in 18 New Drug Applications (NDAs) submitted to the FDA between 2000 and 2008. These RCTs were conducted for at least 48 weeks in duration and were used to support approval of new molecular entity, new formulation, or major label change. To delineate potential gender differences in antiretroviral treatment (ART), we evaluated the percentage of subjects with HIV RNA less than 50 copies per milliliter at 48 weeks. Analyses of the database represent the most systematic review of gender-related ART efficacy data to date. Overall, the meta-analyses did not demonstrate statistically or clinically significant gender differences in virologic outcome at week 48. However, the corresponding subgroup analyses appear to show several statistically significant gender differences favoring males.
Introduction
O
Delineating potential gender differences in response to ART is important to HIV clinical care, research, and drug development. 1 –18 FDA reviewers are uniquely positioned to conduct such analyses because of our access to the data from numerous clinical trials submitted to the FDA and to independently conduct our own analyses. To address the important public health need to evaluate gender-related differences for ARV treatment, we conducted a research project entitled “Women in HIV Trials: A Comprehensive Review and Meta-Analysis” funded by a grant from FDA's Office of Women's Health. The objectives of Part I are: (1) to summarize the proportions of women included in the efficacy trials in NDAs for HIV drugs submitted between 2000 and 2008 and (2) to determine if any significant gender-related findings were identified in medical reviews, statistical reviews and the last approved label for each ART. 19 –46 The objectives of Part II are to conduct meta-analyses of the efficacy and safety outcomes by gender. This article presents the proportion of women included in efficacy trials from 2000 to 2008 and analyzes results of selected efficacy outcomes by gender using meta-analysis methods. Other efficacy and safety analyses are currently ongoing.
Methods
Trial design and population
The selection criteria for eligibility of trials in the meta-analyses were as follows. We identified all randomized clinical trials (RCTs) for treatment of HIV infection submitted to the FDA between 2000 and 2008. The RCTs identified were those used to support FDA approval of a new molecular entity, new formulation, or major label change. The selected RCTs of HIV-1 drugs were pivotal registrational trials of at least 48 weeks in duration and had electronic safety and efficacy data submitted with the application to FDA. Of note, only the sponsor who owns the NDA on file at FDA can submit data to the NDA. Typically the sponsors of trials used to support FDA approval of a new molecular entity, new formulation, or to change a label are pharmaceutical companies. Nonpharmaceutical sponsored trials were not included in the database because these trials were not submitted as part of an NDA. One pharmaceutical company-sponsored pivotal trial was not included because the electronic data were not archived at the FDA. We did not prespecify a specific percentage of women in each trial for inclusion into the database. That is, all available data on women and men were included. No other criteria were used for the inclusion of the trials.
Finally we constructed a database of selected trials and merged the qualified datasets to conduct meta-analyses to identify any differences in efficacy of antiretroviral therapies between women and men. The database was generated based on the Clinical Data Interchange Standards Consortium (CDISC) 47 standard with Study Data Tabulation Model (SDTM) format, which consists of the demographic, discontinuation status, and HIV-1 RNA data. Virologic response rate, defined as proportion of subjects with HIV-1 RNA less than 50 copies per milliliter, was the end point used for the meta-analyses. FDA's primary efficacy evaluation is usually based on the difference in proportions between treatment arms instead of risk ratio or odds ratio. However, in the statistical modeling process, both gender-related efficacy differences between females and males and the corresponding odds ratio were used as the outcome measurements. These analyses were conducted for treatment-naïve (TN) and treatment-experienced (TE) patient populations respectively. We categorized baseline HIV RNA and CD4 cell count using their respective overall median values as the cut-point for the analyses presented. The unit of analysis for the meta-analyses was treatment arm in any trial.
Homogeneity test and models for meta-analysis
For the meta-analysis, the two most commonly used models, the fixed effects model (FEM) and the random effects model (REM) were used. 48 REM is used to overcome the assumption of homogeneity across trial arms.
To determine if the gender differences in response rates are constant across treatment arms, we first examined the degree of heterogeneity across treatment arms by using the conventional Cochran Q statistic (Equation 1 in Table 1) and I 2 statistics (Equation 2 in Table 1). 49 –53 We used the I 2 statistics in order to quantify the degree of heterogeneity. If I 2<0, we consider that there is not sufficient evidence to argue against homogeneity and therefore FEM would be appropriate. The overall weighted point estimate for the gender-related efficacy differences based on FEM was then obtained (Equation 3 in Table 1). If I 2>0, then heterogeneity would be considered and REM is used to obtain the overall weighted point estimate (Equation 3 in Table 1). For these homogeneity tests, the gender-related efficacy differences was used as an outcome measurement and the effects of baseline covariates were not adjusted.
Two types of REM (Equations 4 and 5 in Table 1) adjusted by some covariates at baseline were applied: (1) the REM in Equation 4 included gender, baseline age, ethnicity, region, CD4 count (≤or>median value), and HIV-1 RNA (≤or>median value) and (2) the REM in Equation 5 consisted of four additional interaction terms (region by HIV-1 RNA, region by CD4, age by CD4 and age by HIV-1 RNA).
For the main meta-analysis comparing efficacy differences between females and males by treatment arm, point estimates and 95% confidence intervals (CI) for the overall estimated outcome is reported. Comparisons of means between males and females in baseline HIV-1 RNA and CD4 count are based on two-sample t test. p Values<0.05 two-sided for main analysis are considered statistically significant. In addition, 20 subgroup analyses were conducted with respect to age (≤33 years, >33 and ≤42 years, >42 years), ethnicity (Caucasian, African American, Others, or Missing), and geographic region (North America, Central South America, Europe, Others, or Missing) for both gender-related efficacy differences and odds ratio. Among a total of 24 possible subgroups in the TN and TE populations, we excluded the 4 subgroups “Others” and “Missing.” The type I error α=0.0025 was chosen to adjust for multiplicity of conducting 20 subgroup analyses using Bonferroni's method. The point estimates and 99.75% confidence intervals (CIs) for overall outcome measurements in each subgroup were obtained to account for the multiple comparisons. p values<0.0025 two-sided for subgroup analysis are considered statistically significant.
SAS PROC NLMIXED and PROC LOGISTIC were used to conduct the meta-analysis for covariate adjustment. The forest plots were utilized to summarize the meta-analysis results. The point estimates of gender-related efficacy differences (Female minus Male) were plotted as squares in the forest plots and the area of each square was proportional to the sample size in each treatment arm. Also, the horizontal line within the red box in the plots denoted the overall results.
Results
We have successfully created a database from 18 NDAs electronically submitted to the FDA between 2000 and 2008, supporting the approval of a new molecular entity, new formulation, or major label change. The database consists of 20,328 patients from 40 pivotal RCTs of HIV-1 drugs involving 7 drug classes, 16 ARTs, or fixed-dose combinations where treatment durations were at least 48 weeks. Table 2 summarizes the information on the trials and treatment arms. Overall, the forty RCTs include 22 TN trials with 49 treatment arms, and 18 TE trials with 40 treatment arms.
Other dose arms or control not included due to no or limited number of females enrolled.
EFV, efavirenz; ZDV, zidovudine; 3TC, 2′, 3′-dideoxy-3′-thiacytidine; IDV, indinavir; NFV, nelfinavir; DDI, didanosine; D4T, stavudine; ABC, abacavir; FTC, emtricitabine; ATV, atazanavir/r; LPV, lopinavir; FOSAPV, fosamprenavir; RTV, ritonavir; SQV, saquinavir; ART, antiretroviral therapy; bid, twice daily; TDF, tenofovir.
Female enrollment and baseline characteristics
The percentages of females enrolled in each of the 40 RCTs ranged from 8% to 68%. Overall approximately 20% of the 20,328 subjects included in the database were female. Twenty-four percent of subjects in TN trials (n=11,690) were female and 15% of subjects in TE trials (n=8638) were female.
From 2000 to 2008, an overall decrease in the percentage of women enrolled in HIV RCTs was seen. In 2000, the percentage of females was 27% and, with the exception of one year, remained at a relatively constant rate of 20–24% from years 2001 through 2005. However, the percentage of females enrolled decreased to 11%, 11%, and 12% in 2006, 2007, and 2008, respectively. Female enrollment differed significantly by treatment history at baseline: 24% of subjects in TN trials were female compared to 15% of subjects in TE trials. The lower percentages of females from 2006 to 2008 may be explained by the fact that NDA submissions in these years included more TE trials than TN trials compared to 2000–2005.
The mean age (standard deviation) of females at enrollment was 36 (9.3) years. Forty-five percent were 33 years or younger, 33% were between 33 and 42 years of age, and 21% were 42 years or older. In contrast, the mean age of males (standard deviation) was 40 (9.5) years. Twenty-seven percent of males were 33 years or younger, 37% were between 33 and 42 years of age, and 36% were 42 years or older. On average males were older than females at enrollment.
Enrollment also varied among race/ethnic groups. Thirteen percent of Caucasian subjects (n=11,219) and 20% of Hispanic subjects (n=2164) were female. Also, 38% of black subjects (n=3430) were female.
Tables 3 and 4 summarize the baseline HIV-1 RNA and CD4 cell counts for males and females in TN and TE trials, respectively. In TN trials, females had lower mean baseline viral loads compared to males (p<0.0001). Comparable baseline CD4 cell counts were seen for both genders. In TE trials, females had greater mean baseline CD4 count compared to males (p=0.0016). No significant differences were seen between females and males for baseline HIV-1 RNA.
Gender-related efficacy differences by treatment arm
Figures 1 and 2 show results for the gender-related efficacy differences analyses from the TN and TE populations, respectively. Five arms (10%) in TN population and four arms (10%) in TE population favored males significantly (p<0.05). Three arms (6%) in TN population and no treatment arms in TE population favored females. Overall estimated gender-related efficacy differences (95% CI) values are −1.34% (−4.54%, 1.87%) and −2.13% (−5.56%, 1.30%) for TN and TE populations, respectively, indicating overall no clinically or statistically significant gender differences.
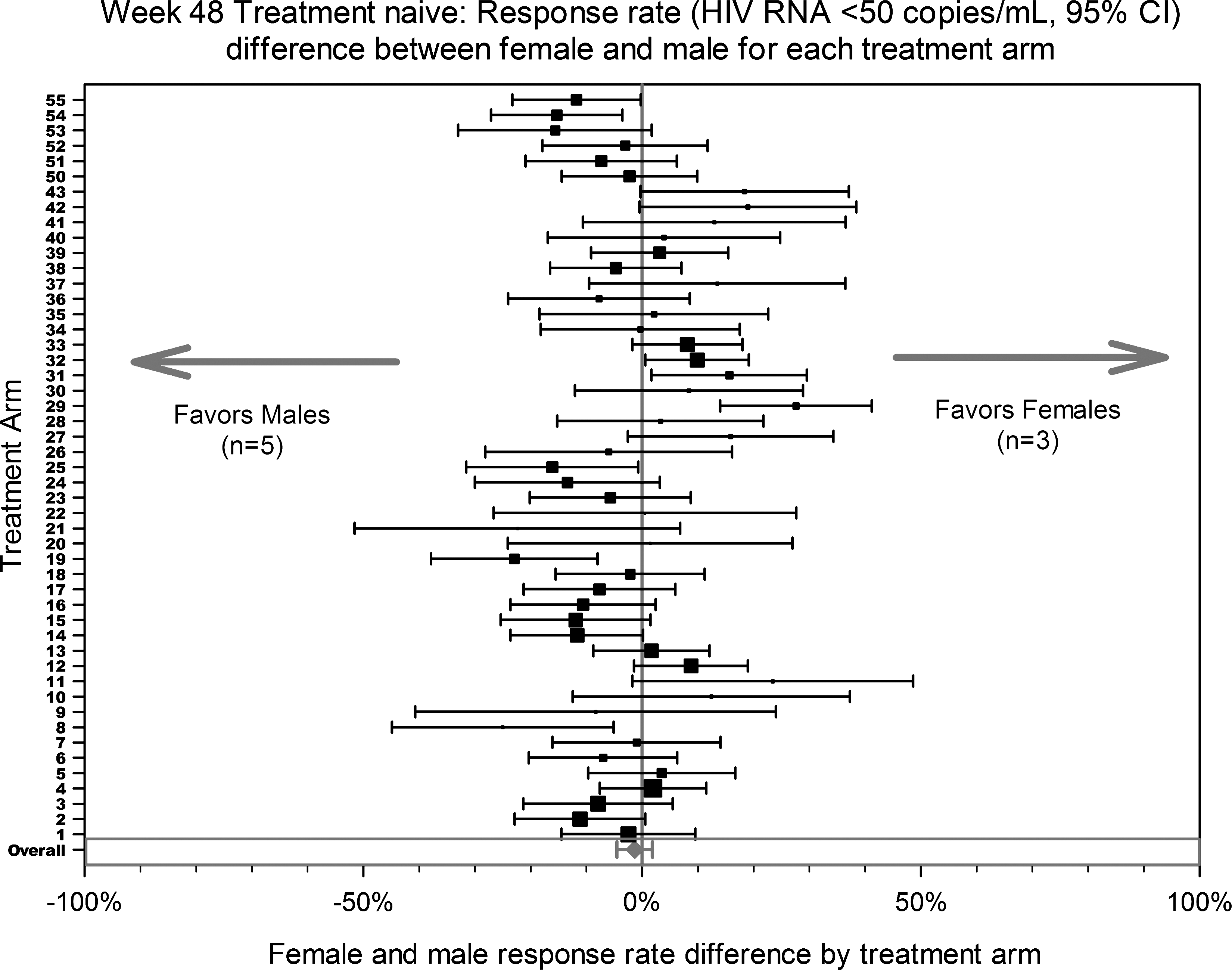
Gender-related efficacy differences by treatment arm for treatment-naïve trials. CI, confidence interval.
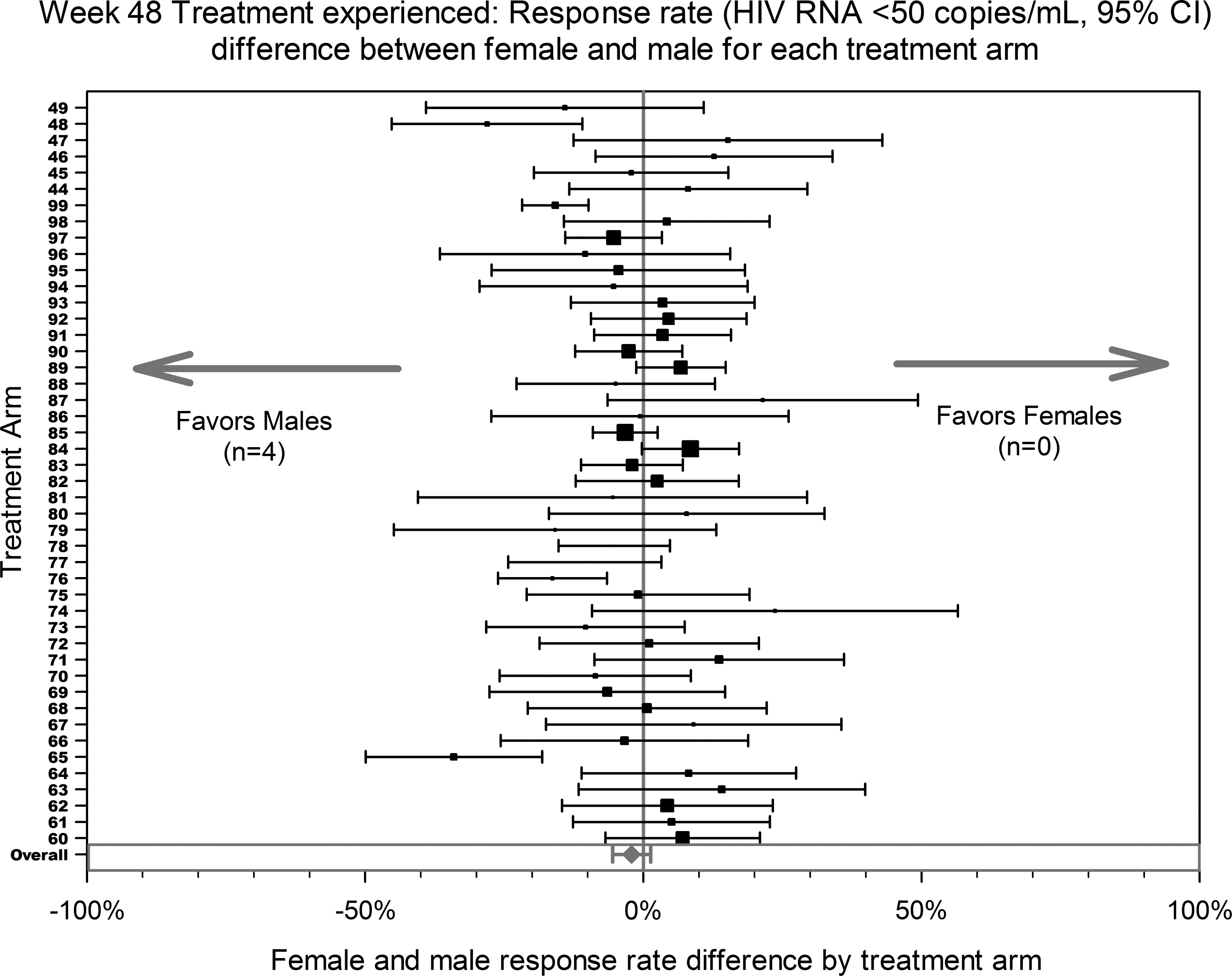
Gender-related efficacy differences by treatment arm for treatment-experienced trials. CI, confidence interval.
Gender-related efficacy differences by subgroups of age, region, and ethnicity
Figures 3 –5 display the overall results (point estimates and 99.75% CIs) for the subgroups defined by age, region, and ethnic groups. Four subgroups were not displayed due to small sample sizes. Among a total of 20 subgroups, statistically significant gender-related efficacy differences were seen only for Caucasians in the TN population (Fig. 5) and for North America in the TE population (Fig. 4), both favoring males.
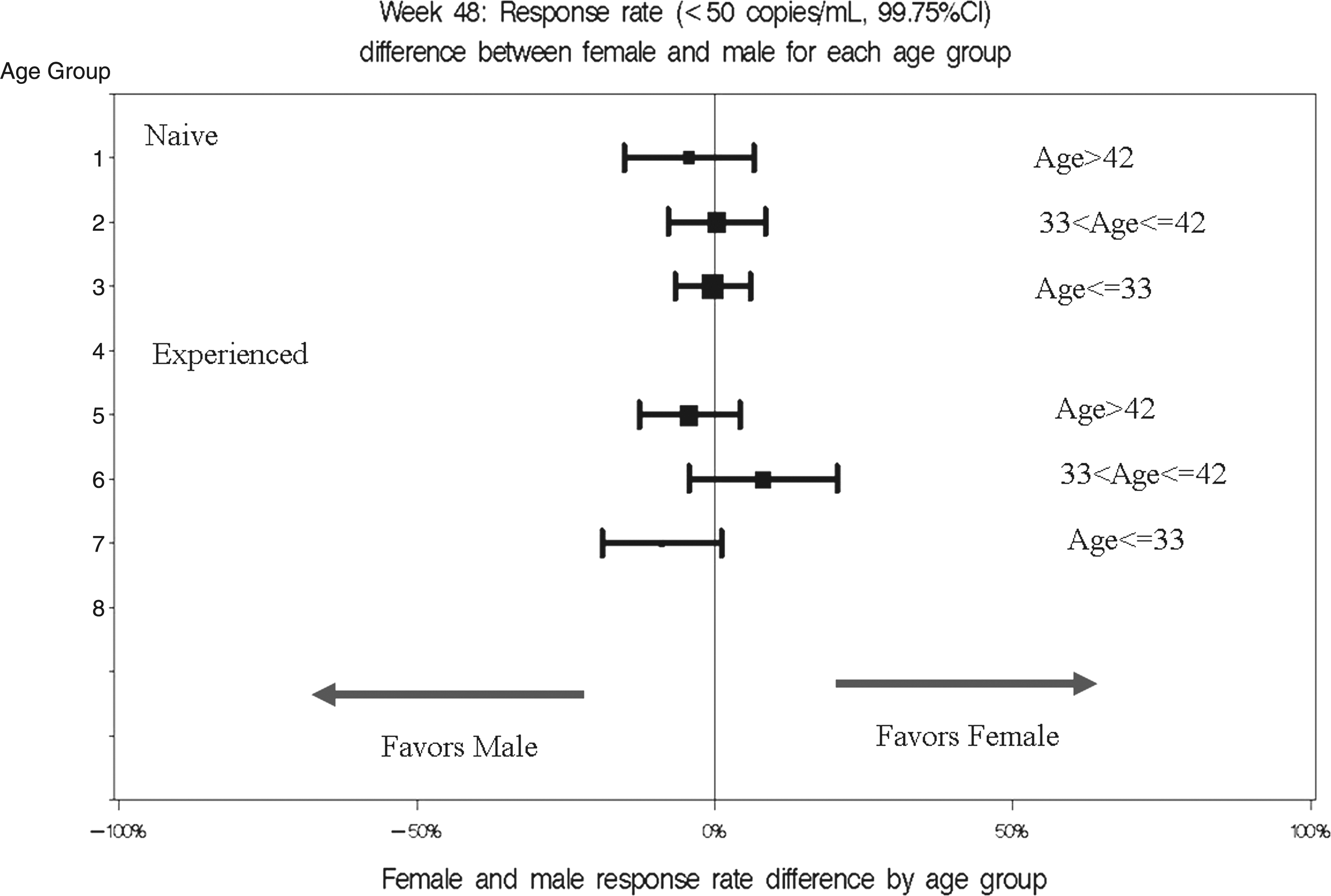
Gender-related efficacy differences by treatment arm for each age group. CI, confidence interval.
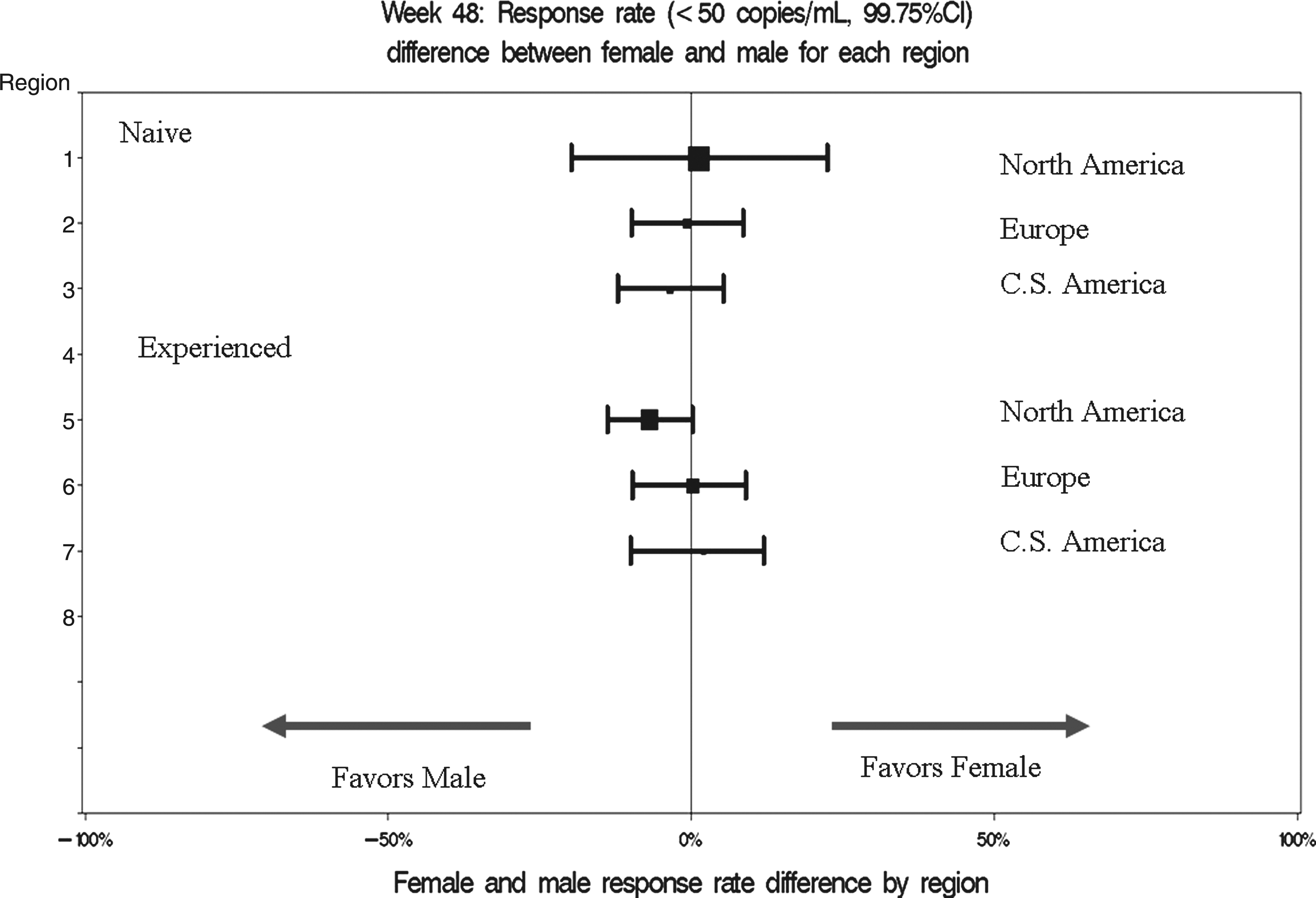
Gender-related efficacy differences by treatment arm for each region. CI, confidence interval.
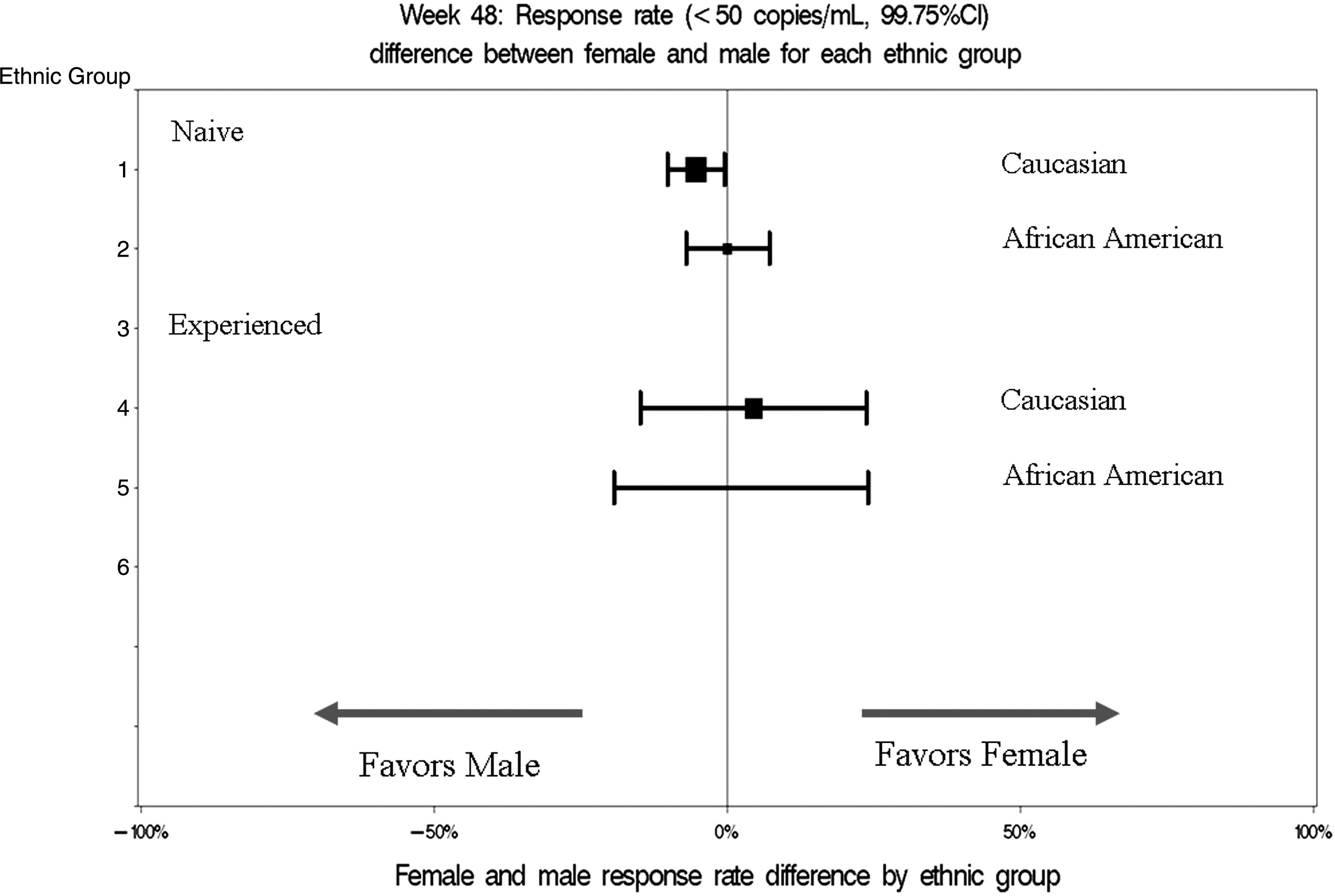
Gender-related efficacy differences by treatment arm for each ethnic group. CI, confidence interval.
Odds ratio with covariate adjustment
The models in Equation 4 were used to adjust for baseline covariates including age, region, ethnic groups, baseline HIV-1 RNA, and CD4 cell counts. Also, the odds ratio was the outcome measurement in the models. Based on 20 subgroup analyses, no statistically significant gender differences were seen with the exception of one statistically significant gender difference observed for the Caucasian subgroup in the TN population (p=0.001) favoring males.
The models in Equation 5 were utilized to evaluate some important interaction terms in addition to those in Equation 4. Statistically significant differences were observed for region by baseline viral load interaction in TN trials (p=0.0001) and for region by baseline CD4 count interaction in TE trials (p=0.0303). These findings indicate that regional effects may differ by median baseline HIV-1 RNA or CD4 subgroups.
Discussion
The estimated number of women living with HIV is 15.5 million and represents nearly one half of the HIV-positive population worldwide. 18 However, according to many researchers and patient advocates, female enrollment in HIV clinical trials has been suboptimal. Because the individual randomized HIV-1 drug trial lack statistical power to conduct appropriate subgroup analyses relating to potential gender differences, the FDA created a comprehensive database from the 40 RCTs of HIV-1 drugs submitted to the FDA during the years 2000–2008. Our project represents the most comprehensive review of gender-related ART efficacy information to date. Although women represent a large proportion of the HIV infected population worldwide, we found women only represented approximately 20% of the subjects in RCTs submitted to the FDA during 2000–2008.
We conducted many meta-analyses including both FEM and REM to explore any potential gender differences with respect to the efficacy outcome measurements (gender-related efficacy differences and odds ratio). Our data show ARTs were equally efficacious in men and women on average, although this does not preclude that some individual treatments may have true gender differences. The gender-related efficacy differences analyses at Week 48 without adjustment of covariates show no clinically or statistically significant gender differences. However, based on 20 subgroup analyses with respect to age, region, and ethnicity, we found more treatment-naïve Caucasian males achieved HIV RNA less than 50 copies per milliliter compared to treatment-naïve Caucasian females. Similarly, more treatment-experienced males in North America achieved HIV RNA less than 50 copeis per milliliter compared to treatment-experienced females in North America. Overall, the meta-analyses on odds ratio with covariate adjustment did not show any statistically significant gender differences. The corresponding subgroup analyses appeared to show one statistically significant gender difference for Caucasian subjects in the TN population (p=0.001) favoring males. Overall analyses with baseline interaction terms indicated that regional effects may differ by median baseline HIV-1 RNA or CD4 subgroups.
Although we conducted systematic analyses by ART types (TN and TE), other limitations for such analyses are noted. Data from the RCT of HIV-1 drugs may be complicated by the fact that trial subjects in each arm took three or more HIV-1 drugs, resulting in many different combination treatment regimens. Bias could not be avoided because the database only consists of successful RCTs submitted to the FDA as these trials were used to support approval. Bias may also be introduced due to statistical methodological restrictions.
Our future work includes investigating specific ARTs or ART regimens that may lead to the gender differences in outcome measurements. Other statistical modeling techniques such as Bayesian meta-analyses may be considered.
Footnotes
Acknowledgments
This work was supported by the funding from the FDA Office of Women's Health. Preliminary data analyses were previously presented at the 16th Conference on Retroviruses and Opportunistic Infections, Montreal, Canada, February 8–11, 2009 (Poster 987b). We gratefully acknowledge the expert advice provided by Fraser Smith, Office of Biostatistics, Center for Drug Evaluation and Research, Food and Drug Administration, Silver Spring, Maryland.
The views expressed are those of the authors. No official support or endorsements by the US Food and Drug Administration is provided or should be inferred.
Author Disclosure Statement
No competing financial interests exist.