
Abstract
Although past work has documented relations between HIV/AIDS and negative affective symptoms and disorders, empirical work has only just begun to address explanatory processes that may underlie these associations. The current investigation sought to test the main and interactive effects of HIV symptom distress and anxiety sensitivity in relation to symptoms of panic disorder (PD), social anxiety disorder (SA), and depression among people with HIV/AIDS. Participants were 164 adults with HIV/AIDS (17.1% women; mean age, 48.40) recruited from AIDS service organizations (ASOs) in Vermont/New Hampshire and New York City. The sample identified as 40.9% white/Caucasian, 31.1% black, 22.0% Hispanic, and 6.1% mixed/other; with more than half (56.7%) reporting an annual income less than or equal to $10,000. Both men and women reported unprotected sex with men as the primary route of HIV transmission (64.4% and 50%, respectively). HIV symptom distress and anxiety sensitivity (AS) were significantly positively related to PD, SA, and depression symptoms. As predicted, there was a significant interaction between HIV symptom distress and anxiety sensitivity in terms of PD and SA symptoms, but not depressive symptoms. Results suggest that anxiety sensitivity and HIV symptom distress are clinically relevant factors to consider in terms of anxiety and depression among people living with HIV/AIDS. It may be important to evaluate these factors among patients with HIV/AIDS to identify individuals who may be at a particularly high risk for anxiety and depression problems. Limitations included recruitment from ASOs, cross-sectional self-report data, and lack of a clinical diagnostic assessment.
Introduction
A
One promising area of study may be in better understanding the association between HIV symptoms and increased risk for anxiety and depressive states. 30 –33 This work is driven, in part, by the recognition that as a result of HIV/AIDS and medication regimens used to treat the illness, persons living with the disease often experience a wide range of bodily sensations and related aversive interoceptive perturbation 32 ; common symptoms include fatigue, nausea, chills/sweats, feeling dizzy/light-headed, pain/numbness in the hands and feet, trouble remembering, diarrhea, and sleep difficulties. Many of these symptoms often co-occur and overlap with medication side effects, 31 complicating the isolation of their origin.
Theoretically, these HIV symptoms and related distress are apt to serve as internal stimuli that could trigger greater degress of anxiety and depression symptoms among persons living with HIV/AIDS. Indeed, empirical work supports a relation between HIV symptom distress and anxiety and depression symptoms. 30 –33 Thus, greater degrees of HIV symptoms may be an important trigger for greater degress of anxiety/depressive symptoms. Yet, it is unclear if all persons with HIV/AIDS evidence similar risk for anxiety/depressive symptoms as a result of HIV symptom distress, or whether specific subsets of this population are most at risk due to individual differences.
One cognitive factor that may predispose certain persons living with HIV/AIDS to greater anxiety and depression symptoms is anxiety sensitivity (AS). 34 AS is operationally defined as the fear of anxiety and arousal-related sensations. 35 AS has been conceptualized as a relatively stable cognitive factor that is conceptually and empirically distinct from the actual experience of (negative) emotional states. 36 When anxious or experiencing somatic symptoms, individuals high in AS may become more acutely fearful due, specifically, to beliefs that these anxiety and related bodily sensations (e.g., rapid heartbeat) have harmful personal consequences (e.g., “I am going crazy”). Among individuals without HIV/AIDS, a diverse array of studies, ranging from laboratory to field approaches, indicate that AS is concurrently, incrementally, and prospectively associated with anxiety symptoms and its disorders, and to a lesser extent, depressive states. 37 In fact, past work has found that AS is incrementally related to greater anxiety, somatization, and depression symptoms among persons with HIV/AIDS. 34
Theoretically, HIV symptom distress and AS may interact to confer greater risk for anxiety symptoms. 36 From this theoretical framework, higher levels of HIV symptom distress may be exacerbated by an individual's level of AS, and thereby may be associated with higher anxiety symptoms. Conversely, an individual's HIV symptom distress level may trigger more AS-specific cognitive reactions. Therefore, these processes may, theoretically, function synergistically to confer greater risk for anxiety symptoms. To offer one such illustration, an individual with HIV/AIDS who has high levels of both HIV symptom distress and AS may be at an increased risk of experiencing more severe anxiety symptoms. In terms of depression, previous work has found that under high levels of life stress, AS is more relevant for anxiety versus depression. 38 Thus, individuals who experience high levels of HIV symptom distress and high levels of fear and misinterpretations of symptoms (high AS) may be more likely to endorse anxiety related symptoms than depressive symptoms. As such, this HIV symptom distress-AS interactive model may be most relevant to anxiety states and related psychopathology.
The present investigation sought to test the singular and interactive relations of AS and HIV symptom distress in regard to symptoms of panic disorder (PD) social anxiety disorder (SA) and depression among adults living with HIV/AIDS. We chose these particular anxiety symptom dimensions for several reasons: (1) there are elevated rates of PD and SA among people living with HIV/AIDS; 1,39 (2) empirical work suggests that SA and related symptoms are associated with poor HIV management 39 and sexual risk behaviors (i.e., unprotected insertive anal intercourse) among people living with HIV/AIDS, 20 and (3) a body of research underscores clinically significant relations between AS and PD among individuals without HIV/AIDS 40 and rates of PD are elevated among those with HIV/AIDS compared to the general population (11–16% versus 2–3%). 41,42 It was expected that HIV symptom distress and AS would both be independently and positively related to PD, SA, and depressive symptoms. In addition, it was predicted that the interaction between HIV symptom distress and AS would be significantly related to anxiety symptoms, such that HIV symptom distress would be related to anxiety symptoms at high levels of AS, but not at low levels of AS. This prediction was driven by theory 36 and empirical data 34 suggesting that AS may have the most deleterious emotional effects when operating in a context of high internal stress (e.g., bodily sensations). Moreover, as an important test of the incremental validity of this theoretical perspective, it was predicted that the interactive effect of HIV symptom distress by AS would be observed above and beyond the generalized tendency to experience negative affect states (negative affectivity) as well as severity of HIV disease. That is, the interactive process would not simply be better accounted for by a more (basic) generalized tendency to experience negative mood states or a more severe disease state. Furthermore, to test the specificity of this interactive association for anxiety vulnerability factors, it also was hypothesized that a similar pattern of findings would not be evident for depressive symptoms. The logic underlying this prediction was that the purported HIV symptom distress-AS effects should theoretically be unique to an anxiety model and not apparent generally for any negative mood states (e.g., depressed affect).
Methods
Participants
Please see Table 1 for participant demographic characteristics. Participants included 164 adults (mean [M] age=48.40, standard deviation [SD]=9.57, observed range=19–73; 17.1% female) with HIV/AIDS. The race/ethnic composition of the sample was 40.9% white/Caucasian, 31.1% black, 22.0% Hispanic, and 6.1% mixed/other (e.g., Native American, French, West Indian). Half of the sample identified as gay, 36.6% as heterosexual, and 12.2% as bisexual. Although the majority (69.5%) reported having a high school degree or higher level of education, 75.6% reported being unemployed. Accordingly, more than half (56.7%) reported an annual income less than or equal to $10,000. Half of the participants reported a diagnosis of HIV while 47% reported a diagnosis of AIDS (3% did not indicate which diagnosis they had). On average, participants reported living with HIV for 15 years (M=15.23, SD=6.39).
M, mean; SD, standard deviation.
Participants were eligible to participate if they were at least 18 years old, had a diagnosis of HIV/AIDS, and had the mental capacity to give informed written consent, which was assessed by the ability to read through the consent form and explain the study purpose. No participants were excluded from participation. Of note, one participant's data was not included in the analyses because the response pattern was indicative of random responding (i.e., endorsed the same value on every item on each questionnaire).
Measures
Demographic (e.g., age, gender, race/ethnicity) and medical information, including participant HIV/AIDS status, disease stage (indexed by most recent CD4+ T cell count), and month and year of diagnosis were self-reported by participants.
Positive and Negative Affect Scale (PANAS). 43 Trait-like negative mood was assessed using the well-established 20-item PANAS. For each of 20 adjectives (e.g., “irritable”), participants indicate on a 5-point Likert-type scale (1=very slightly to 5=extremely) the degree to which the descriptor typifies how they generally felt during the past year. Only the negative affectivity scale (PANAS-NA) was used in this study as a global index of the trait-level propensity to experience negative affect symptoms. The PANAS-NA has demonstrated excellent internal consistency in clinical and non-clinical populations (range of α coefficients: 0.85 to 0.93) including persons with HIV/AIDS, 34 test–retest reliability (e.g., r=0.71 for 2 months to r=0.43 for 72 months), as well as convergent and discriminant validity in relation to multiple measures of state-level affect, trait-level mood, and personality. 44 The PANAS-NA evidenced good internal consistency among the present sample (Cronbach α=0.89).
Anxiety Sensitivity Index-3 (ASI-3). 45
The ASI-3 is an 18-item measure on which respondents indicate, on a 5-point Likert-type scale (0=very little to 4=very much), the degree to which they fear the potential negative consequences of anxiety-related symptoms and sensations (e.g., “It scares me when my heart beats fast”). The sum of all item responses yields the total ASI score, which ranges from 0 to 72. The ASI-3 has demonstrated good psychometric properties. 45,46 The ASI-3 is composed of one higher-order factor (AS-Total) and three lower-order factors: Physical, Psychological, and Social Concerns. 45 In the present investigation, the total score was employed, as it captures the various facets of the construct. The ASI-3 demonstrated high levels of internal consistency in terms of the total score (Cronbach α=0.95) and individual subscales (AS-cognitive α=0.93, AS-physical α=0.90, AS-social α=0.83) among the present sample.
AIDS Clinical Trials Group Symptoms Distress Module (ACTG-SDM). 32
The ACTG-SDM, was used to measure distress related to HIV symptoms. Participants rate on a 5-point Likert-type scale (0=I do not have this symptom to 4=It bothers me a lot) the extent to which each of 20 commonly experienced symptoms with HIV/AIDS (e.g., muscle aches, nausea) is bothersome. This scale has demonstrated good construct validity with relations to physical and mental components of health-related quality of life independent of CD4+ T cell count and HIV viral load 32 and associations with the ability to tolerate distress, 47 as well as perceived stigma. 48 The ACTG-SDM demonstrated high levels of internal consistency in the current sample (Cronbach α=0.92).
Inventory of Depression and Anxiety Symptoms (IDAS). 49
The IDAS is a 64-item measure that assesses symptom dimensions of depression and anxiety disorders. The IDAS contains 10 specific symptom scales: suicidality, lassitude, insomnia, appetite loss, appetite gain, ill temper, well-being, PD, SA, and traumatic intrusions, and, two broader scales: general depression and dysphoria. The IDAS subscales have demonstrated sound internal consistency across multiple clinical and nonclinical populations (range of α coefficients: 0.72–0.92), test–retest reliability (e.g., r=0.79 for 1 week) as well as convergent and discriminant validity in relation to the multiple measures of depression and anxiety. 49 The current study utilized the PD, SA, and general depression subscales. All three subscales demonstrated good internal consistency among the present sample (Cronbach α=0.88, 0.78, 0.91, respectively).
Procedure
Participants were recruited from local AIDS service organizations (ASOs) and hospital-based medical clinics in Vermont and New Hampshire, and an ASO in New York City (NYC). Slightly more than half of the participants (58.5%) were recruited from NYC. Interested persons contacting the research clinic at the University of Vermont (Anxiety and Health Research Laboratory) or the ASO in NYC, and who self-reported having a diagnosis of HIV or AIDS, were scheduled for an in-person appointment. Participants were then told that they would be asked to report their most recent CD4+ T cell count and viral load at the appointment (to reduce error in reporting). Eligible persons came into the research clinic or their ASO and were informed about the study. After consenting to participate, participants completed a battery of self-report measures and were compensated $25 for their time. This study was approved by the institutional review board of the University of Vermont.
Data analytic strategy
Descriptive statistics and bivariate correlations among continuous variables were first examined. Criterion variables included the IDAS-based subscales of (1) PD, (2) SA, and (3) depression. Hierarchical regression analyses were subsequently conducted with the criterion variables. Age, gender, race/ethnicity, CD4 T cell count, recruitment site, and negative affectivity were entered at step 1 as control variables. The main effects of AS and HIV symptom distress were entered at step 2, and the mean centered interaction term of AS and HIV symptom distress was entered at step 3. To interpret significant interactions, simple slope tests were performed using the macro created by Hayes and Matthes. 50 The form of the interactions were graphed according to the recommendations of Cohen and Cohen, 51 which includes computing symptom values by inserting specific values for each predictor variable (e.g., one-half standard deviation above and below the mean of the predictor variables) into the regression equations associated with the described analysis.
Results
Descriptive data and bivariate correlations
Means, standard deviations, the observed range, and bivariate correlations among study variables are reported in Table 2. The AS-total score and individual AS subscales were positively and significantly related to panic (range of observed r=0.36 to 0.46, p<0.001), social anxiety (range of observed r=0.43 to 0.52, p<0.001), and depression scores (range of observed r=0.37 to 0.51, p<0.001). HIV symptom distress was positively and significantly related to panic (r=0.46, p<0.001), social anxiety (r=0.41, p<0.001), and depression scores (r=0.51, p<0.001). HIV symptom distress and AS-total scores were positively and significantly related to one another (r=0.30, p<0.001; 9% shared variance). PANAS-NA scores were positively and significantly related to the criterion variables (range of observed r=0.46 to 0.67, p<0.001), HIV symptom distress (r=0.47, p<0.001), AS-total score (r=0.49, p<0.001), and AS-subscales (range of observed r=0.40 to 0.52, p<0.001). Age was negatively and significantly related to the criterion variables (range of observed r=−0.17 to −0.20), but was not significantly associated with any of the other predictor variables. HIV disease stage, as indexed by CD4 T cell count, was not related to the predictor or criterion variables.
Note: * p<0.05, ** p<0.01, *** p<0.001.
Positive and Negative Affect Scale-Negative Affectivity (Watson et al., 1988); bAIDS Clinical Trials Group Symptoms Distress Module (Justice et al., 2001); cAnxiety Sensitivity Index-3 (Taylor et al., 2007); dInventory of Depression and Anxiety Symptoms (Watson et al., 2007).
Hierarchical regression analyses
See Table 3 for a summary of hierarchical regression analyses. For PD scores, demographic variables entered at step 1 accounted for a significant portion of variance (R 2=0.33, p<0.001), with significant contributions made by race/ethnicity (β=0.22, p=0.01) and negative affectivity (β=0.42, p<0.001). At step 2, the main effects of HIV symptom distress and AS-total score accounted for an additional 10% of variance (p<0.001), with both predictors making significant contributions (β=0.32, p<0.001 and β=0.18, p=0.03, respectively). At step 3, the interactive effect accounted for an additional 4% of variance (p=0.001).
Inventory of Depression and Anxiety Symptoms (Watson et al., 2007).
Gender coded as 1=male 2=female.
Recruitment site coded as 1=Vermont/New Hampshire 2=New York City.
Positive and Negative Affect Scale-Negative Affectivity (Watson et al., 1988).
AIDS Clinical Trials Group Symptoms Distress Module (Justice et al., 2001).
Anxiety Sensitivity Index-3 (Taylor et al., 2007).
Mean centered interaction term.
Regarding SA scores, demographic variables entered at step1 accounted for a significant portion of variance (R 2=0.41, p<0.001), with a significant contribution made only by negative affectivity (β=0.57, p<0.001). At step 2, the main effects of HIV symptom distress and AS-total score accounted for an additional 8% of variance (p<0.001), with both predictors making significant contributions (β=0.16, p=0.03 and β=0.27, p=0.001, respectively). At step 3, the interactive effect accounted for an additional 2% of variance (p=0.02).
For depression scores, demographic variables entered at step 1 accounted for a significant portion of variance (R 2=0.51, p<0.001), with significant contributions made by age (β=−15, p=0.02), sex (β=0.20, p=0.005), and negative affectivity (β=0.61, p<0.001). At step 2, the main effects of HIV symptom distress and AS-total score accounted for an additional 6% of variance, with both predictors making significant contributions (β=0.23, p=0.001 and β=0.16, p=0.03, respectively). At step 3, the interactive effect did not account for any additional variance (−R 2=0.00, p=0.96).
Interpretation of the observed significant interactions
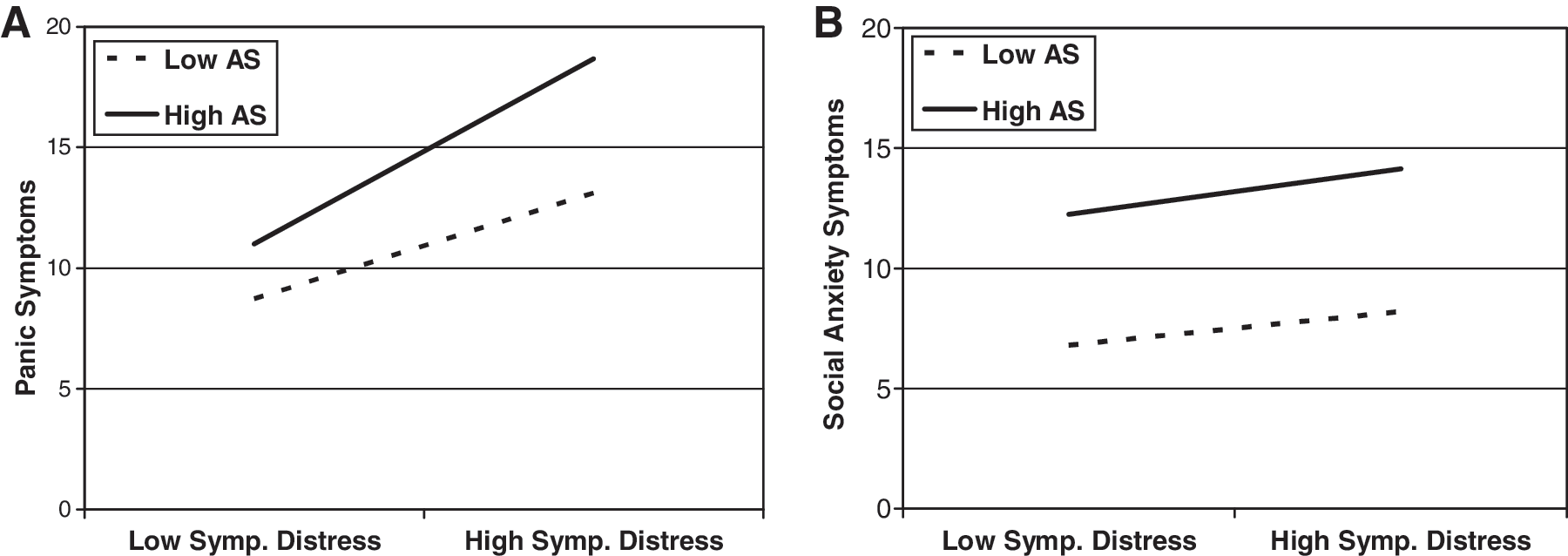
We then conducted simple slopes tests to interpret examine the form of the significant interactions. As shown in Fig. 1A, HIV symptom distress was positively related to PD at high levels of AS (b=0.18, t=5.31, p=0.00), but was not related to PD at low levels of AS (b=0.04, t=1.24, p=0.26). Similarly, as shown in Fig. 1B, HIV symptom distress was positively related to SA only at high levels of AS (b=0.07, t=3.24, p=0.00), and not at low levels of AS (b=0.003, t=0.11, p=0.92). In other words, HIV symptom distress was only related to PD and SA at high levels of AS.
(
Post hoc examination of individual AS subscales
Identical hierarchical regression models testing the interaction between HIV symptom distress and individual AS-subscales in relation to panic, social anxiety, and depression symptoms were explored. For panic symptoms, there were significant interactive effects between HIV symptom distress and all of the AS-subscales (AS-physical: total R 2=0.45, interaction term β=0.18, p=0.01; AS-cognitive: total R 2=0.48, interaction term β=0.23, p<0.001; AS-social: total R 2=0.45, interaction term β=0.17, p=0.01). For social anxiety symptoms, there were significant interactive effects between HIV symptom distress and AS-social (total R 2=0.53, interaction term β=0.17, p=0.007) and a trend towards significance with AS-cognitive (total R 2=0.48, interaction term β=0.12, p=0.06). There were no significant interactive effects between HIV symptom distress and AS-subscales in terms of depression symptoms.
Discussion
There is a growing body of research documenting significant relations between HIV/AIDS and anxiety and depression. 1,2,7 However, limited work has examined vulnerability factors that may place people living with HIV/AIDS at risk for these emotional problems. To begin to address this gap in the existing literature, the current study sought to examine the main and interactive effects of AS and HIV symptom distress in relation to symptoms of PD, SA, and depression.
Consistent with prediction, HIV symptom distress significantly interacted with AS in regards to symptoms of PD and SA. The size of the observed (incremental) interactive effects were 4% and 2% of variance (respectively) above and beyond the variance accounted for by demographic variables, HIV disease stage, negative affectivity, and the significant main effects (Table 3). Given the magnitude of variance accounted for at steps 1 and 2, it is noteworthy that the interactive effects enhanced the model's predictive power at all. 52 Inspection of the form of the interactions was in accord with the a priori theoretical formulation. Specifically, HIV symptom distress was only related to symptoms of PD and SA at high levels of AS (Fig. 1A and B). Thus, the observed interactive effect of HIV symptom distress and AS appears to be relevant for both PD and SA symptoms. Individuals with high levels of AS and HIV symptom distress may be more likely to misinterpret HIV-related symptoms as anxiety and catastrophize symptoms, which in turn, may lead to and maintain anxiety and perhaps HIV-related symptom distress. Future work is needed to assess this interactive effect in relation to other forms of anxiety psychopathology (e.g., generalized anxiety disorder, posttraumatic stress disorder). These data broadly highlight the importance of assessing distinct anxiety-relevant emotional states among the HIV/AIDS population and suggest that there may be a clinically relevant interplay between HIV symptom distress and cognitive factors (AS) in regard to specific anxiety symptoms (i.e., PD, SA).
Notably, also as predicted, there was no significant interaction for HIV symptom distress and AS in terms of depressive symptoms. This pattern of findings suggests that AS has a unique explanatory role for anxiety vulnerability in the context of HIV symptom distress. Future work is need to examine the clinical utility of AS in terms of vulnerability for depression among people with HIV/AIDS.
In terms of main effects, it is noteworthy that both AS and HIV symptom distress were incrementally related to PD, SA, and depressive symptoms; contributing 10%, 8%, and 6% of unique variance, respectively. Here, HIV symptom distress was significantly positively associated with each of the criterion variables, such that higher levels of HIV symptom distress were related to higher levels of PD, SA, and depression symptoms. These findings are consistent with past work related to HIV symptom distress and vulnerability for anxiety/depression. 30 –33 Also as expected, AS was positively related to each of the outcome variables. That is, individuals reporting higher levels of AS reported higher PD, SA, and depression symptoms. Moreover, these effects were not attributed to a generalized tendency to experience negative emotional states (PANAS-NA) or severity of HIV/AIDS. These AS-anxiety/depression main effect findings replicate and extend previous relations observed among people with HIV/AIDS. 34
Although not the primary aim of the study, at least two additional findings warrant brief comment. First, AS and HIV symptom distress were empirically distinguishable from one another (r=0.30, p<0.001; sharing 9% of variance). Thus, these two constructs are distinct, though related, explanatory factors for emotional symptoms among persons living with HIV/AIDS. Second, there was consistent evidence that negative affectivity was robustly related to each of the dependent measures. These findings are consistent with past work 44 and again, underscore the explanatory role of a tendency to experience negative affect states in models of anxiety-depression vulnerability. 53
Based on the present findings there are at least two key clinical implications. First, the results suggest that AS and HIV symptom distress are clinically relevant factors to consider in terms of anxiety and depression among people living with HIV/AIDS. It may be important to evaluate these factors among patients with HIV/AIDS to identify individuals who may be at a particularly high risk for anxiety and depression problems. Second, targeting AS and HIV symptom distress via cognitive–behavioral or pharmacologic interventions may be clinically useful in reducing anxiety and depression.
The current findings should be considered in light of several limitations that might be addressed by future work relevant to this line of inquiry. First, the current investigation was cross-sectional in design and thus the direction and causal nature of these relations cannot be interpreted within the context of the current study. Future work might examine these relations prospectively to elucidate the directional effects of the observed relations. Second, the findings from the current study may have been influenced by shared method variance as a result of utilizing self-report measures to assess the main study constructs. A useful next step may be to assess these relations utilizing multimethod approaches, such as a laboratory assessment of reactivity to emotion provocation tasks or examining these relations in real-time using ecological momentary assessment. 54 Third, we did not use a structured clinical interview for the present study to ascertain lifetime or current psychiatric diagnoses. Future work, building from the present results, may benefit from such an assessment approach as a way to further contextualize the types of psychiatric problems characterizing an HIV/AIDS sample. Fourth, the sample was recruited primarily through ASOs, which may represent a relatively well-connected group of individuals in terms of social support, care coordination, and health awareness. Future work should expand recruitment efforts to include a more representative sample of people living with HIV/AIDS. Finally, the current study was limited to examination of one, albeit clinically relevant, cognitive vulnerability factor (AS) for anxiety and its interaction with HIV symptom distress. There may be other anxiety risk factors that may add additional unique explanatory value in terms of anxiety among people living with HIV/AIDS (e.g., pain-related anxiety). 55
Overall, the current study uniquely extends the literature on anxiety and depression vulnerability among people living with HIV/AIDS. Future investigations are needed to examine these relations prospectively and to determine the clinical utility of AS reduction programs for persons with HIV/AIDS who may be at particularly high risk (e.g., high AS and high HIV symptom distress) for anxiety and depression.
Footnotes
Acknowledgments
This project was funded by a McNeil Prevention and Community Psychology grant awarded to Dr. Gonzalez and a University of Vermont Undergraduate Research Endeavors Competitive Award granted to Mr. Parent.
Author Disclosure Statement
No competing financial interests exist.