
Abstract

Dear Editor:
Despite the challenges inherent in its screening and detection, acute HIV infection (AHI) is a worthwhile diagnostic pursuit, because these patients 1 are more likely to transmit the virus. 2 Moreover, a recent study has demonstrated personal and public health benefits with early antiretroviral treatment (ART) initiation in reducing clinical events and sexual transmission. 3 To maximize opportunities for secondary HIV prevention, identification of AHI coupled with an outpatient HIV primary care medical visit within three months of diagnosis 4 is essential. However, medical management of AHI is not well characterized. Furthermore, the lack of a commonly accepted operational definition for AHI has hampered efforts to evaluate care or clinician management practices of AHI at a population level. In 2008, the New York City (NYC) Department of Health and Mental Hygiene (DOHMH) developed an AHI surveillance case definition 5 and, since then, has conducted city-wide AHI surveillance. 6 We performed longitudinal follow-up among NYC AHI cases diagnosed in 2008 focusing on entry into care and clinician management practices to improve understanding about secondary HIV prevention.
AHI cases were identified among the subset of all cases of HIV diagnosed and reported to the NYC HIV Surveillance Registry. The registry is maintained through legally-mandated public health reporting of all CD4 and viral load (VL) test results, positive Western blot (WB) tests, and HIV genotypes 7 that are matched to cases in the registry and updated accordingly. We defined AHI to include those individuals reported to NYC DOHMH by August 29, 2009 with a laboratory pattern consistent with recent HIV seroconversion: HIV antibody negative/indeterminate with a detectable VL; negative/indeterminate antibody test followed by a positive WB or a positive nucleic acid amplification test. All laboratory data on AHI cases was obtained from the registry. 7
The “site of diagnosis” was defined as the ordering provider of the laboratory results that first established the HIV diagnosis. The diagnosing site was characterized as “hospital” for patients diagnosed while hospitalized and “non-hospital” for all others including DOHMH sexually transmitted diseases (STD) clinics. The “site of care” was defined as the ordering provider of the first CD4 or VL occurring at least 1 or more days following the diagnosis date. Patients without laboratory results within 12 months of HIV diagnosis date could not be assigned a care site for chart abstraction and were classified as out of care in NYC. Care was categorized as “colocated” if the patient received HIV-related care at a facility affiliated with the diagnosing site. Care was categorized as “non-colocated” if either HIV-related care was not offered by the diagnosing provider or the patient sought care at a site not affiliated with the diagnosing provider.
Chart abstraction occurred more than 1 year from diagnosis at the care site and included (1) classification of both the diagnosing and care site and (2) confirmation that the surveillance laboratory report correlated with timely entry into HIV care (i.e., an outpatient HIV primary care visit within 3 months of HIV diagnosis). 4 The initial medical management decision was categorized as either clinical trial referral, clinician-initiated ART, or clinician monitored without immediate ART initiation based on the Department of Health and Human Services (DHHS) guidelines in place at the beginning of the analysis period. 8 We did not assign a category for patients who entered care more than 3 months after diagnosis (i.e., delayed diagnosis), because they were no longer in the acute phase of HIV infection when the management decision was made. Demographic information and risk data were obtained from the registry and descriptive summary statistics generated. If an AIDS-defining CD4 percentage only was reported, we assumed a CD4 count of 199 cells per microliter. Data analyses were performed using SAS version 9.1.3 (SAS Institute Inc., Cary, NC).
Sixty-three persons were diagnosed with confirmed AHI in NYC in 2008. Figure 1 shows the flow of AHI patients by care entry and clinician management category. Of the 8 excluded patients whose care status could not be tracked, five were classified as out of care in NYC with the following sites of diagnosis: hospital=4; STD clinic=1. Ultimately, 55 patients entered HIV care in NYC. Most (n=38; 69%) were 20–40 years old. Overall, 91% (n=50) were men, of whom 80% (n=44) reported a history of sex with men. Blacks and whites each comprised 29%. Over one third (38%) reported Hispanic ethnicity.
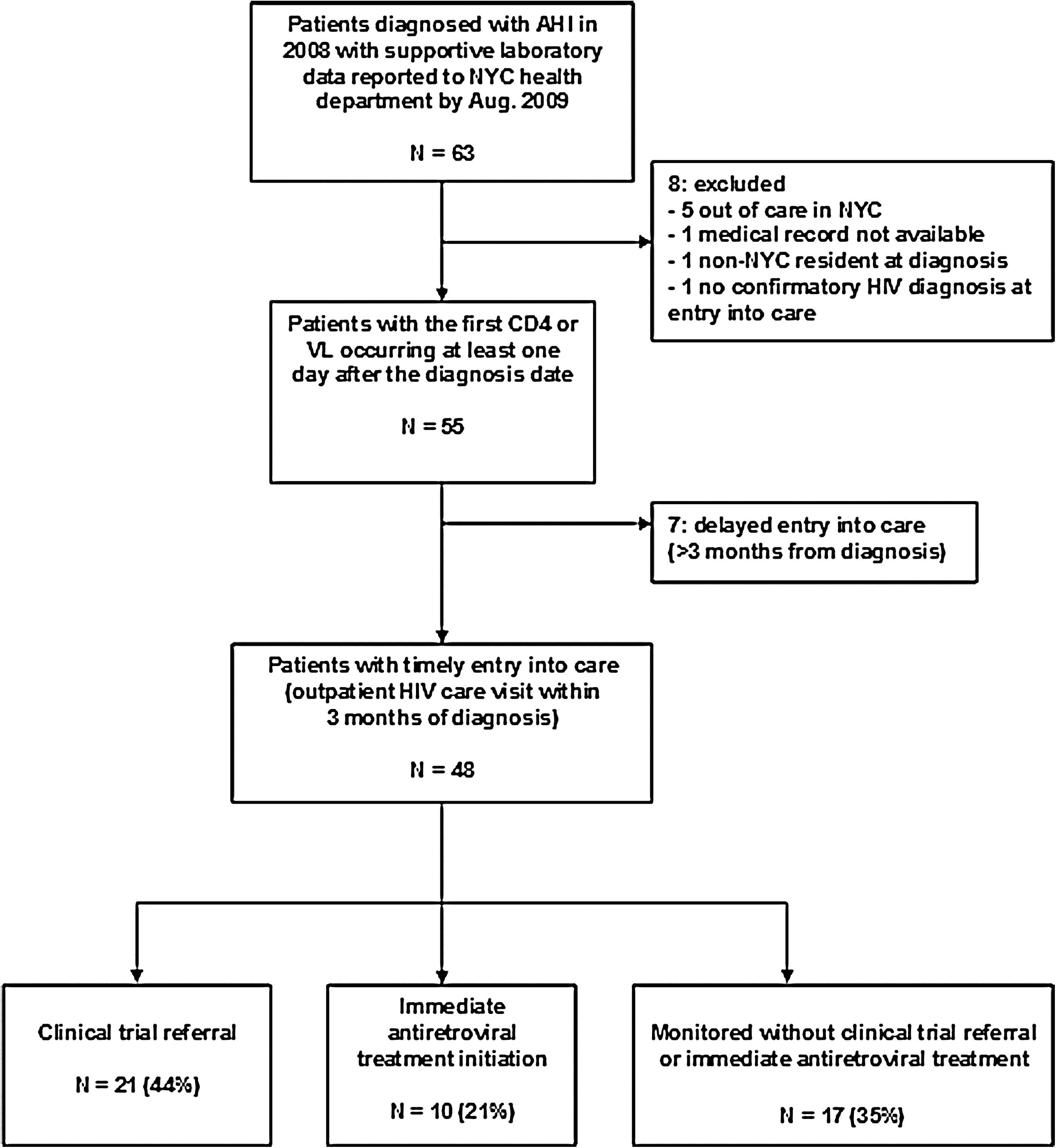
Entry into care and initial clinician management categories for patients diagnosed in New York City (NYC) with acute HIV in 2008.
All 55 patients had a laboratory result reported to surveillance indicating timely entry into care, with most (n=37; 67%) diagnosed in a nonhospital setting including 16 at DOHMH STD clinics. However, chart review confirmed that fewer (n=48; 87%) had actually entered care in a timely manner. Of the 7 with delayed entry, 5 were diagnosed at non-colocated sites (nonhospital=5 including 2 from the STD clinic). A larger proportion of patients diagnosed at sites with colocated care entered care in a timely manner than did those diagnosed at non-colocated sites, but this difference was not statistically significant (93% [28/30] versus 80% [20/25], p=0.22).
Figure 1 shows the initial medical management category for patients with timely entry into care. Receiving care in a hospital was not associated with management decision. Overall, 44% of patients were referred to a clinical trial. Of those managed by clinicians, 10 (37%) received ART with the median time from AHI diagnosis to ART initiation of 16.5 days (interquartile range [IQR]: 5.0–32.0). The time from AHI diagnosis to ART initiation was significantly lower for patients receiving colocated care site compared to those receiving non-colocated care (7.0 versus 39.5 days [median], p=0.01).
Of all patients who had timely entry into care, 92% (n=44) had at least one CD4 count or percentage only reported within 90 days of diagnosis. All 48 who entered timely care had an initial VL reported, of which most (n=32; 67%) were greater than 100,000 copies per milliliter. If the DHHS guidelines 8 for treatment initiation (CD4<350) were applied to the clinician-managed patients (n=27), 15 (56%) would have been treatment-eligible, of whom 6 (40%) were initiated on ART. Using CD4 cutoff treatment eligibility suggested by HPTN 052 results (CD4<550), 85% (23/27) patients would be eligible for ART.
Overall, most AHI cases were diagnosed in nonhospital settings and entered HIV care quickly; however, they were more likely to do so if the diagnosing and care sites were collocated. 4 As expected, clinicians' AHI management practices varied considerably, reflecting the variability in recommended approaches in DHHS guidelines. 8 Because these AHI diagnoses were made in New York City, where multiple randomized clinical trials (RCTs) are actively seeking to enroll AHI-diagnosed patients, the proportion of patients enrolling in RCTs is likely to be higher than would be found in most other areas of the United States. Of the patients managed by clinicians, only 37% were initiated on ART with patients at a colocated site starting treatment within a week of their diagnosis compared to over a month for those diagnosed at a non-colocated site. Given the variability in treatment initiation of AHI patients and, when started, its timeliness, in 2008 we were not experiencing the full benefits of AHI diagnosis to community-wide prevention efforts. This will only come from a streamlined management approach that includes rapid initiation of ART (HPTN 052) in conjunction with the counseling and partner services activities already in place, consistent with aggressive application of the 2011 DHHS treatment guidelines. 9
We found that many of our NYC AHI diagnoses were made through AHI screening programs in DOHMH STD clinics. Despite the lack of colocated HIV care, a strong partnership with a HIV care facility ensured timely linkage to care and clinical trial referral for most STD diagnosed patients. This is of particular importance for public health efforts to increase AHI testing. As other jurisdictions incorporate AHI testing within their STD clinics, they must ensure that the effort and expense of AHI case identification is matched with successful and rapid entry into care and, ideally, treatment, in order to realize the full benefits of early HIV diagnosis. Equally, providers in the community who diagnose AHI must also ensure entry into care. We found that most patients who did not make it into care within 12 months (out of care in NYC) were diagnosed in the inpatient unit. This raises concern as to whether these patients understood their diagnosis and need to engage in care. Moreover, patients diagnosed in the inpatient setting may need additional support and counseling to ensure that they understand the importance of follow-up care during this critical phase of HIV transmissibility.
Although surveillance laboratory reports have been used as a proxy for entry and continuity of care, 10 findings suggest that the use of CD4/VL reports to public health overestimates entry into care, as blood work may be done prior to the HIV primary care evaluation especially for those patients diagnosed on the inpatient unit. In addition, continuity of care for AHI patients may be underestimated if they are referred to an AHI clinical trial that utilizes a nonclinical, research laboratory for CD4/VLs which are exempted from public health reporting for HIV. Given the importance of monitoring entry and continuity of care for all HIV-infected patients whether newly infected or not, current restrictions of not allowing the use of the HIV registry for clinical purposes must be reconsidered. 11
Footnotes
Acknowledgments
Chart abstractions were also conducted by Jason Livingstone. We would like to thank the NYC DOHMH Public Health Advisors who conducted the initial chart reviews.The authors do not have a commercial or other association that may pose a conflict of interest. This research was supported in part by CDC cooperative agreement # U62/CCU223460-05-4.