
Abstract
We assessed changes in sexual behaviors from baseline to 12-month follow-up among a multisite cohort of HIV-positive racial/ethnic minority young men who have sex with men enrolled in an outreach, linkage, and retention study. In the 3 months prior to their baseline interview, more than three-quarters of participants (78.5%) reported sex with at least one man (mean: 2.3 partners). Among sexually active participants, 44.2% had one partner; 50.5% had 2–9 partners; and 5.3% had 10 or more partners. Over three-quarters (77.5%) reported engaging in sex with at least one steady partner, 43.5% with at least one casual partner, and 29.5% with both casual and steady partners. Exchanging sex for money, drugs, or other needs was reported by 13.2%. Use of condoms during oral and anal sex increased significantly from baseline to 12-month follow-up (oral sex: 29.1–42.5%, p=0.02; anal sex: 67.8–76.2%, p=0.05). While unprotected anal sex significantly decreased among individuals who were new to care (34.8–18.3%, p<0.0001), it significantly increased among individuals who were previously in care (26.7–37.5%, p=0.03). Overall, exchange sex decreased from 13.3% at baseline to 5.0% at 12 months (p=0.001). Despite reductions in unprotected sexual encounters and exchange sex through one year of follow-up, many participants continued to engage in high-risk sexual behaviors. Retention within this study appeared to be associated with decreases in high-risk sexual behaviors, especially among participants who were new to care, although more research is needed. Future studies should investigate sexual network characteristics and the prevalence of behaviors such as serosorting.
Introduction
R
Unprotected anal intercourse (UAI), especially receptive UAI, is a high-risk sexual behavior that has been shown to greatly increase the risk of HIV transmission. 5,6 Reported rates of engaging in UAI among racial/ethnic minority YMSM are high. More than one-third (37%) of African-American YMSM in the YMS reported UAI in the prior 6 months, and 23.1% of those YMSM who engaged in UAI had unrecognized HIV infection. 7 A study in Chicago of 273 MSM aged 16–24 found that 38.6% of African-American YMSM and 43.6% of Latino MSM reported UAI in the previous 12 months. Additionally, more than one-quarter of African-American (28.7%), and more than one-fifth of Latino YMSM (20.8%) had engaged in commercial sex. 8
Several studies have found that receiving an HIV diagnosis is correlated with a reduction in high-risk sexual behaviors among MSM. 9 –11 In their study, Gorbach et al. found that among MSM recently diagnosed with HIV, the mean number of reported sex partners decreased at the 3-month follow-up following initial diagnosis, 9 and the prevalence of UAI with unknown HIV-status partners decreased from 42% at diagnosis to 23% at 9-month follow-up. 10 Similarly, a study of MSM in San Diego and Los Angeles found that the number of UAI partners decreased following an HIV-positive diagnosis. 11 While providing insight into changes in behavior following an HIV diagnosis, the mean age of participants in all of these studies was approximately 35 years, and only 30% of participants were nonwhite. Thus, these findings might not be generalizable to the post-diagnosis sexual behaviors of racial/ethnic minority YMSM.
The purpose of this article is to describe the sexual behaviors of a multisite cohort of HIV-positive racial/ethnic minority YMSM at baseline and over a 12-month follow-up period. Most participants in this study were newly diagnosed as HIV-positive and were new to care, with a smaller proportion re-engaging in care. We hypothesized that high-risk sexual behaviors among participants would decrease over this time period, due in part to their engagement in site-specific interventions such as case management and support groups. In light of the disproportionate effect that HIV has had on minority communities, findings from this study will aid in understanding how behaviors of HIV-positive racial/ethnic minority YMSM can be addressed to prevent the spread of HIV.
Methods
Participants
Participants were enrolled at eight demonstration sites (Bronx, NY; Chapel Hill, NC; Chicago, IL; Detroit, MI; Houston, TX; Los Angeles, CA; Oakland, CA; and Rochester, NY) funded by the HIV/AIDS Bureau's Special Projects of National Significance (SPNS) program. The focus of the initiative was to provide outreach to HIV-positive racial/ethnic minority YMSM, link them to HIV-related care, and retain them in care; each site implemented its own innovative outreach, linkage, and retention strategies. Methods for this study have been described elsewhere. 12 In order to be eligible to enroll in the study, participants had to be born male; be HIV-positive and not currently in care; have sex with men, or the intent to have sex with men; self-identify as African-American or Latino; be between the ages of 13 and 24 years at the time of the first interview; and be willing and able to provide full written informed consent and a release of information to obtain medical records.
Procedures
Eligible participants were administered a standardized questionnaire by trained interviewers at each site. Data were collected between June 1, 2006 and August 31, 2009. Analyses were limited to information collected during visits that occurred within 14 months following enrollment into the study. All data were entered into a secure web-based data portal maintained by an evaluation center at The George Washington University (GWU). All instruments and protocols were approved by local institutional review boards (IRBs) and by the GWU IRB.
Measures
Participants reported demographic characteristics such as age, race/ethnicity, sexual orientation, and education.
Sex was defined in this study as “touching of genitals, mutual masturbation, oral sex, vaginal sex, or anal sex.” Frequency of sexual acts (e.g., insertive anal sex, receptive oral sex) in the last 3 months was assessed using a series of four questions: (a) “With how many men?”; (b) “How many were with a one-night stand or a person you had sex with only once?”; (c) “How many were with a lover, steady partner, or boyfriend [or girlfriend]?”; (d) “The last time you had sex, did you/your partner use a condom?” Participants were also asked about age at MSM sexual debut and engaging in sex in exchange for drugs or money.
Participants were asked about frequency of alcohol use in the last 2 weeks. Additionally, they were asked about ever use of drugs (e.g., marijuana, methamphetamines, poppers, heroin) and use in the last three months. Number of drugs used was collapsed into three categories (no drug use, used one drug, and used two or more drugs) excluding marijuana use.
Depressive symptomatology was measured using the Center for Epidemiologic Studies Depression Scale (CES-D), a self-report scale consisting of 20 items, each of which is rated based on a 4-point scale. 13 CES-D scores range from 0 to 60, with a score of 16 or greater considered indicative of significant depression.
Statistical analysis
At each site, participants received interventions, most of which involved a risk reduction component, and thus follow-up data will reflect the effect of these interventions. If more than one visit fell within the follow-up window, the average of the continuous responses was used for analysis. For categorical variables, the value from the first follow-up visit was used. Univariable analyses were conducted on baseline sexual behaviors. Correlates with baseline condom use were examined using bivariable analyses to generate Chi-square statistics and associated probabilities. A correlate was considered to be significant if p<0.05. Generalized estimating equations (GEE) with autoregressive correlation matrices and robust estimators of variance were used to investigate significance of trends over time. SAS v.9.1 (SAS Institute, Cary, NC) was used for all analyses.
Results
Baseline demographics and sexual characteristics
Study participants' ages ranged from 15 to 24, with a mean age of 20.4 years (n=363; SD=1.9). Two-thirds of the participants (66.7%) identified as African-American, with the remainder identifying as either Latino (21.5%) or multiracial (11.9%). Nearly three-quarters (71.1%) had at least a high school degree, and 43.3% had at least some college education. The majority of participants (67.2%) had never been in HIV care, while 32.8% reported prior care experience but were currently out of care.
For this sample, the mean age at MSM sexual debut was 14.5 years, with a slightly earlier mean age for heterosexual debut (14.1 years). Nearly one-fifth of participants (18.7%) reported first having sex with a man before the age of 13.
More than three-quarters of participants (78.5%) reported having sex with at least one man in the 3 months prior to their baseline interview. The mean number of male sex partners for this same time period was 2.3 (SD=3.4) (Table 1). Of the 285 participants who reported engaging in sex in the prior 3 months, 44.2% had only one partner; 50.5% had 2–9 partners; and 5.3% had 10 or more partners, with one participant reporting 30 partners. More than three-quarters (77.5%) reported engaging in sex with at least one steady partner, and 43.5% had at least one casual partner, with 29.5% (n=84) reporting sex with both casual and steady partners in the prior 3 months.
Although very few racial/ethnic minority YMSM reported engaging in sex with a woman in the past 3 months (n=22; 6.3%), nearly half of the sample (46.4%) reported engaging in sex with a woman in their lifetime. About one-quarter of the participants (22.6%) identified as heterosexual or bisexual, and a significantly larger proportion of bisexual young men (20.3%) reported sex with a woman in the past 3 months compared to gay men and men who reported “other” as their sexual identity (e.g., multiple identities, “I'm me,” “trisexual”) (1.3% and 8.9%, respectively; p<0.0001).
Nearly three-quarters of participants (72.5%) had engaged in oral sex with a man in the past 3 months, of which more than two-thirds (69.6%) had engaged in both insertive and receptive oral sex. Overall, 70.8% did not use a condom at last oral sex encounter, and there was no difference in lack of condom use during insertive or receptive oral sex. Slightly fewer than three-quarters of participants (71.5%) had engaged in anal sex with a man in the past 3 months. Almost half (45.3%) had engaged in both insertive and receptive anal sex, while 38.2% engaged only in receptive anal sex and 16.5% engaged only in insertive anal sex. Almost one-third (32.2%) did not use a condom during their last episode of insertive or receptive anal sex, and slightly fewer racial/ethnic minority YMSM did not use a condom during their last act of insertive compared to receptive anal sex (26.2% vs. 30.7%, respectively). Not using a condom at last anal sex was significantly associated with not using a condom at last oral sex (p<0.0001).
Exchanging sex for money, drugs, or other needs in the prior 3 months was reported by 13.2% of participants (n=48). Nearly three-quarters (64.8%) of those reporting exchange sex had sex in exchange for money. Other reasons for exchanging sex were to obtain drugs (18.8%), housing (16.7%), transportation (10.4%), or food (8.3%).
In our assessment of factors that may be associated with condom use at last oral or anal intercourse (demonstration site, education, race/ethnicity, age, sexual orientation, having previously been in HIV care, drug/alcohol use, age at MSM sexual debut, exchange sex, or depression as measured by CES-D), none were significantly associated with condom use during last oral or anal intercourse (Table 2).
Row percents unless otherwise noted.
Column percents.
Follow-up
More than two-thirds of participants (70.0%) had at least one follow-up visit. There were 161 racial/ethnic minority YMSM who completed a 3-month follow-up visit, 173 who completed a 6-month follow-up visit, and 141 who completed a 12-month follow-up visit; 109 racial/ethnic minority YMSM had only a baseline visit. Participants who had follow-up visits were not significantly different from participants with only a baseline visit based on education, race/ethnicity, sexual orientation, substance use, and CES-D score. Additionally, there were no significant differences in baseline sexual behaviors. Approximately 70% of participants who were new to HIV care and participants who had previous care experience were retained within the study (70.1% vs. 69.8%, respectively), which was not a significant difference. However, participants with follow-up visits were significantly younger than those with only a baseline visit (20.1 vs. 20.9 years, respectively; p=0.002).
Although there was no change in the proportion of participants who reported sex with other men after enrollment into the study, reported high-risk sexual behaviors decreased over time. The mean number of male sexual partners decreased from 2.3 at baseline to 1.5 at the 12-month follow-up, with the largest drop occurring between baseline and the 3-month follow-up (Fig. 1). This trend was consistent across engagement in all sex acts with other males.
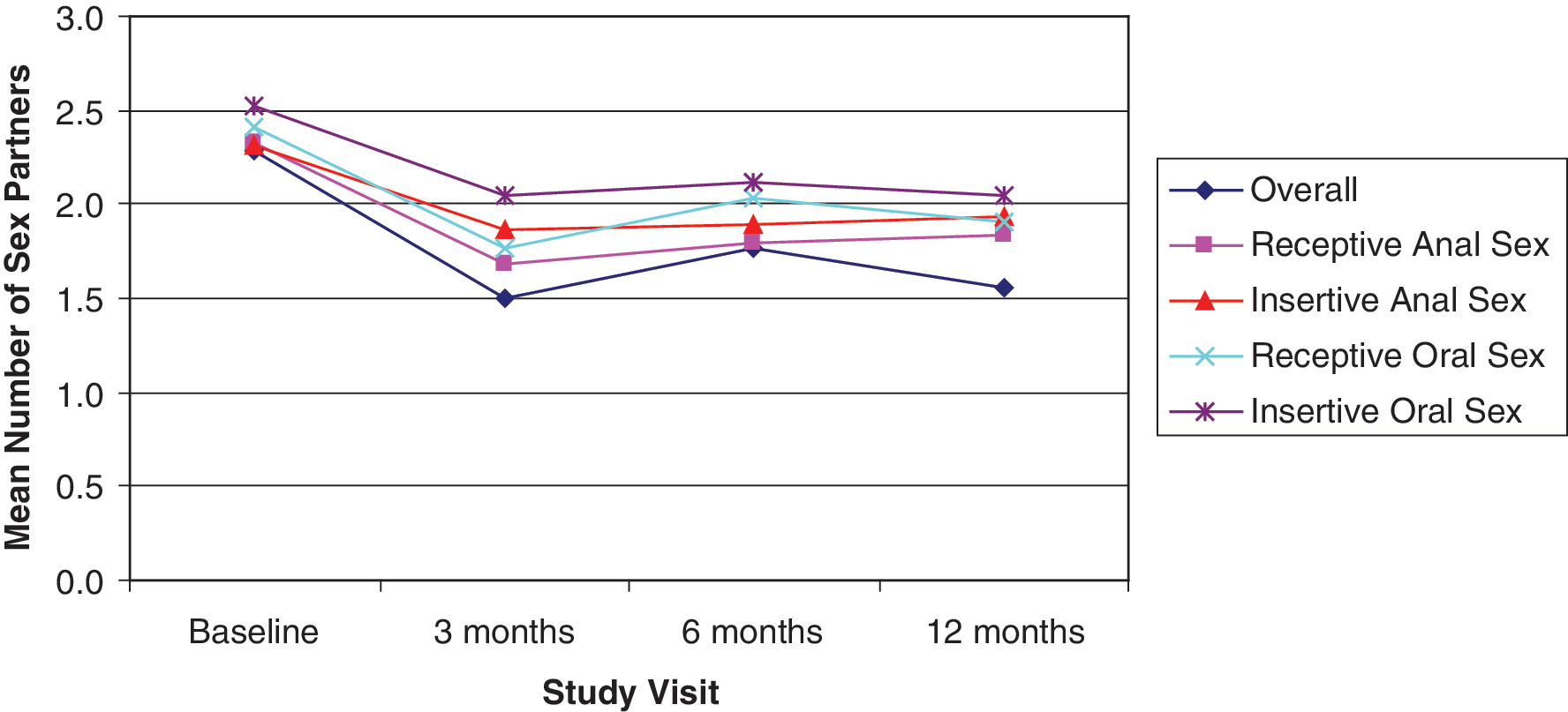
Mean number of male sex partners by sex act at baseline and follow-up among minority YMSM from 8 US sites, 2006–2008.
The proportion of racial/ethnic minority YMSM who reported insertive or receptive oral sex did not significantly change over time, although both increased slightly at the 3-month follow-up visit (Fig. 2). Interestingly, the proportion of participants who reported any acts of insertive anal sex increased from baseline to the 3-month follow-up and remained close to 65% from 3 to 12 months, although this change was not significant. Conversely, the proportion of participants who reported any acts of receptive anal sex decreased from baseline to follow-up, although this pattern was inconsistent throughout follow-up visits.
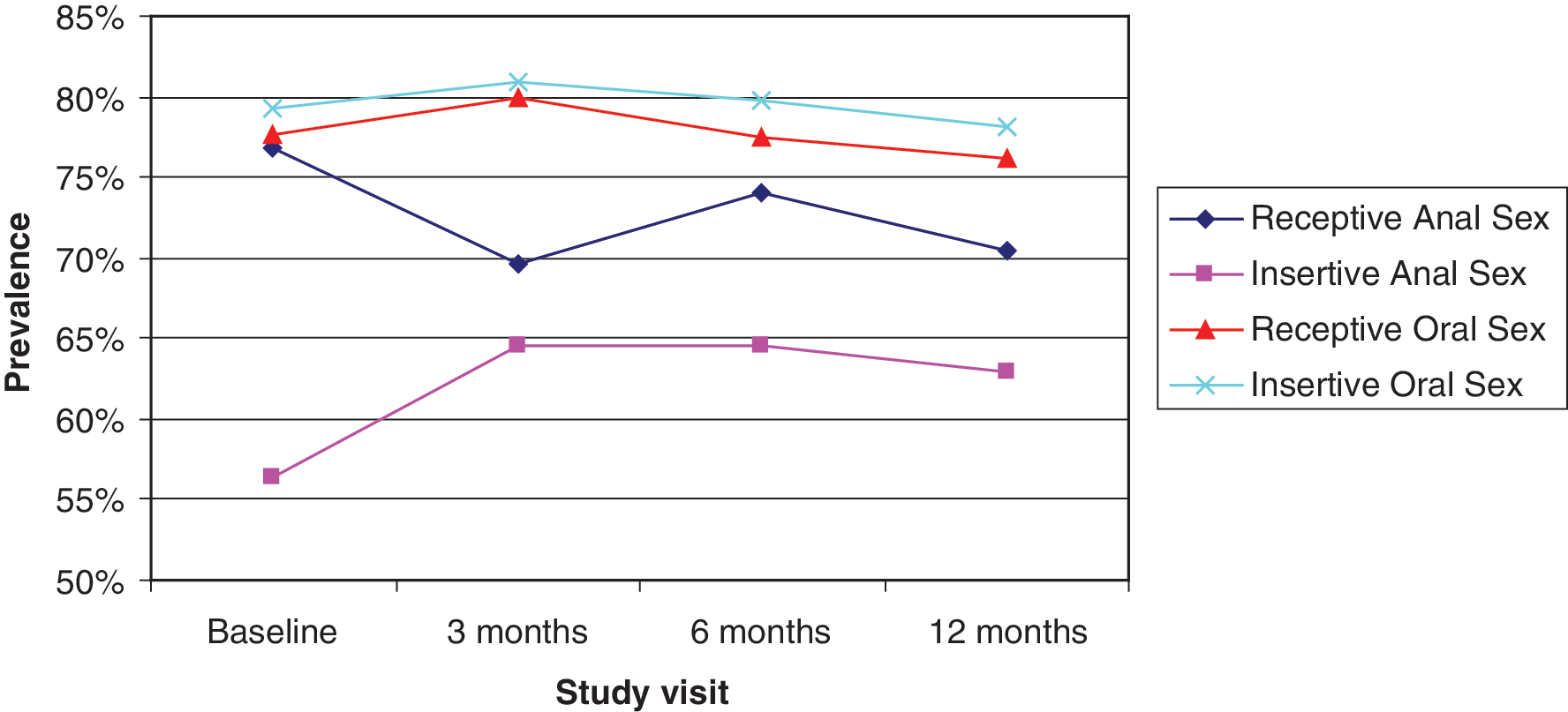
Prevalence of types of sex within cohort at baseline and follow-up among minority YMSM from 8 US sites, 2006–2008.
No condom use at last anal sex significantly decreased over time, dropping from 32.2% at baseline to 23.8% at 12-month follow-up (p=0.05, Fig. 3). Similarly, no condom use at last oral sex also fell from 70.8% at baseline to 57.5% at 12-month follow-up (p=0.02).
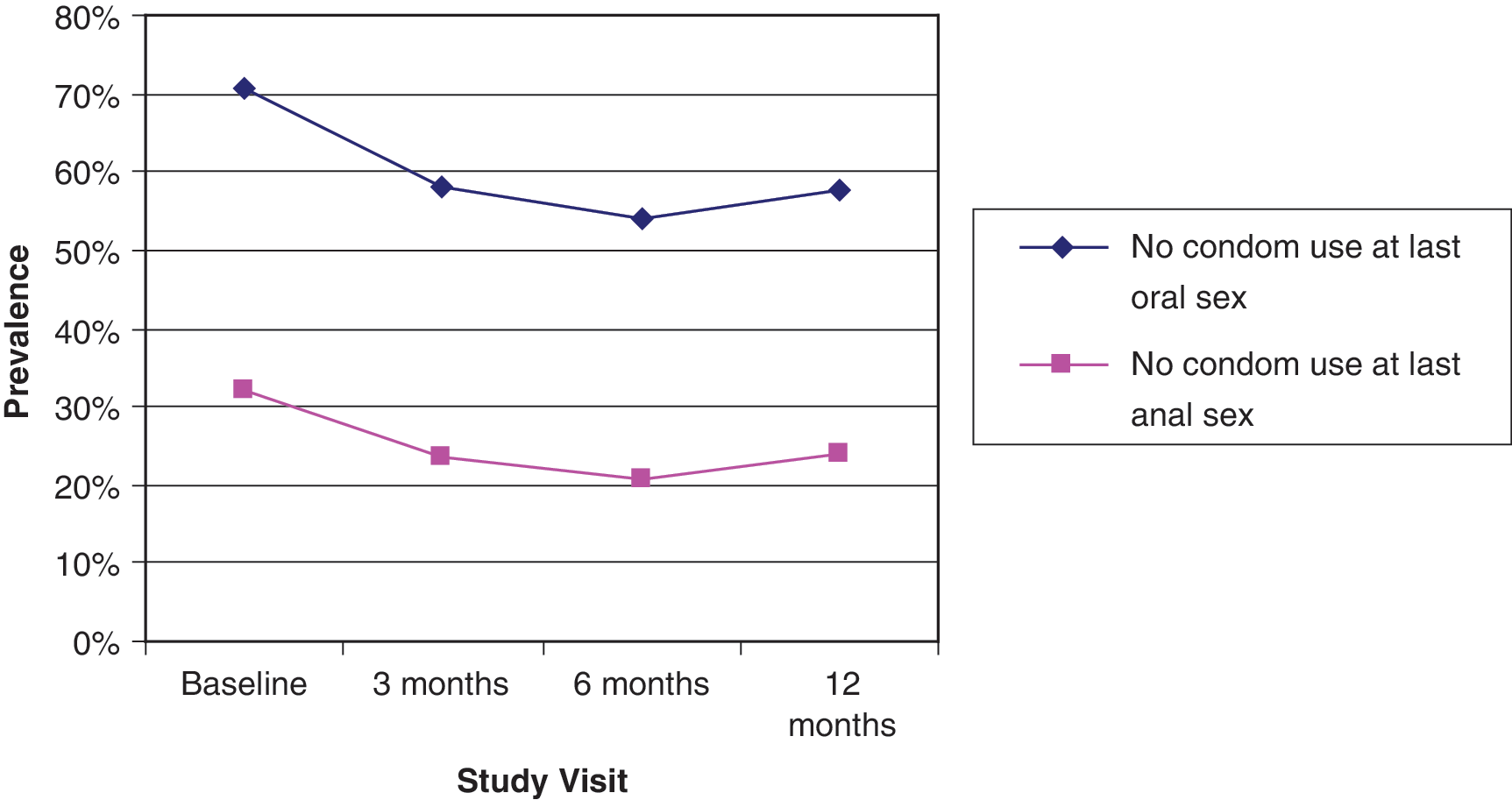
Prevalence of no condom use by type of sex at last sex at baseline and follow-up among minority YMSM from 8 US sites, 2006–2008.
When the data were stratified by whether participants were new to or re-engaging in HIV care, those new to care had a decrease of nearly 20% in no condom use at last oral sex at 3-month follow-up (p=0.01), while no condom use remained steady among individuals who had previously been in HIV care (Table 3). While not using condoms at last episode of anal sex significantly decreased among individuals who were new to care (34.8% to 18.3%, p<0.0001), it significantly increased among individuals who were previously in care (26.7–37.5%, p=0.03).
Reports of exchange sex decreased throughout the follow-up period, from 13.3% at baseline to 6.8% at 3-month follow-up, to 5.8% at 6-month follow-up, and to 5.0% at 12-month follow-up. Overall, the decrease from 13.3% to 5.0% was significant (p=0.001).
Discussion
The majority of this sample of racial/ethnic minority YMSM was sexually active upon study enrollment, and many participants reported engaging in high-risk behaviors such as having multiple sex partners, not using condoms during sexual encounters, and having exchange sex. Reported condom use during both oral and anal sex was low, although condom use during anal intercourse was approximately twice as prevalent as condom use during oral intercourse. While condom use during any sex act is encouraged, usage during anal sex is imperative since anal sex poses a higher risk of HIV transmission than other sex acts. 5,14 Although most participants had taken steps to prevent the potential HIV transmission through anal sex, the risk of transmission remained among the 32.2% of participants who did not use condoms. Prevalence of UAI among participants was similar to that found among other samples of racial/ethnic minority YMSM, although these studies included HIV-negative individuals. 7,8 Within this study, condom use during anal or oral sex did not differ significantly based on race/ethnicity, age, or educational attainment, which is consistent with findings from other studies. 8
While it is likely that reductions in engagement in risky sexual behaviors were associated with retention in the study, this cannot be fully assessed since longitudinal behaviors of participants who were not retained are unknown. However, this conclusion is consistent with findings from another study among HIV-positive youth, which found significant decreases in unprotected sex acts. 15 Due to differences in intervention strategies utilized at each site (e.g., youth case management, support groups), we cannot exactly determine what aspects of the interventions may have helped to bring about decreases in high-risk sexual behavior, although many sites incorporated risk reduction strategies into their interventions.
Findings show that racial/ethnic minority YMSM who were newly engaged in care made significant reductions in high-risk behaviors, whereas those who returned to care after being out of care for at least 6 months, or demonstrated intermittent adherence to prior appointments, showed no change over time. This is a key finding, and demonstrates the importance of retaining this population in care once they receive an HIV diagnosis. Racial/ethnic minority YMSM who are lost to care are likely to be harder to re-engage, and thus may make fewer changes in their high-risk sexual behaviors once re-engaged in care. It is also possible that those youth who re-engaged in care made changes in their behavior when initially engaged in care, and thus required fewer behavior changes than those who were new to care. Despite the fact that participants who re-engaged in care had a higher prevalence of condom use at baseline, the difference was not significant. While racial/ethnic minority YMSM who returned to HIV primary care were more likely to be Latino, report a sexual identity other than gay/homosexual or bisexual, and be older than participants who were new to care, these factors were not found to be significantly associated with the decrease in high-risk sexual behaviors over time, and therefore do not fully explain the differences between these two groups.
Limitations
Study participants consisted of HIV-positive racial/ethnic minority YMSM who were willing to take part in the study and enter into HIV primary care. Therefore, data are missing on HIV-positive racial/ethnic minority YMSM who are not in care and who are potentially engaging in more high-risk behaviors. Additionally, data for follow-up visits are limited to participants who returned for at least one visit following enrollment. Racial/ethnic minority YMSM who returned for subsequent visits might be different from those who were only seen once, although there were no significant differences in age, race/ethnicity, level of education, sexual identity, or engagement in HIV care between these two groups.
Seropositioning (strategic positioning during anal intercourse in which the HIV-positive individual is the receptive partner) 16 and serosorting (having UAI only with someone of the same serostatus) 16 could not be assessed because information on the HIV status of participants' sexual partners was not collected. In addition, viral load and presence of sexually transmitted infections (STIs) was not assessed. These factors are also important in determining one's risk of transmitting HIV and would increase understanding of the level of risk involved with engagement in these sexual behaviors.
Data were collected through face-to-face interviews, which made several biases possible. There was a potential for inter- and intra-interviewer differences, especially between sites. However, all interviewers were extensively trained and monitored to minimize any differences in survey administration. Since these interviews involved personal questions about sexual behaviors, there was also the possibility of social desirability bias, in which participants would under-report high-risk sexual behaviors. All sites reported that participants were extremely comfortable with staff members who administered the surveys, thus increasing the likelihood that participants would truthfully report their behaviors.
Conclusion
Although this cohort of racial/ethnic minority HIV-positive YMSM engaged in several high-risk sexual behaviors at baseline, the prevalence of exchange sex and unprotected oral and anal intercourse decreased over the subsequent 12 months. This finding is encouraging, and lends credence to the necessity of linking this population into care immediately following an HIV diagnosis and retaining them over time in order to reduce high-risk behaviors. Despite reductions in exchange sex, number of sexual partners, and unprotected sex through one year of follow-up, a substantial number of participants continued to engage in high-risk sexual behaviors. Thus, services specific to the needs of racial/ethnic minority YMSM should be developed to encourage retention in care and maintenance of ongoing secondary prevention risk reduction.
Future studies on the high-risk sexual behaviors of HIV-positive racial/ethnic minority YMSM should include issues such as seropositioning and serosorting, since these behaviors have not been extensively studied in this population. In addition, subsequent research should investigate the sexual networks of this population to understand how the close ties within the community may facilitate the spread HIV.
Footnotes
Author Disclosure Statement
No competing financial interests exist.