
Abstract
Most patients (80–90%) newly diagnosed with HIV are started on the antiretroviral regimen efavirenz, emtricitabine, and tenofovir (EFV/FTC/TDF). Existing studies of patient tolerability, however, are limited. We compared symptom experiences of patients on EFV/FTC/TDF, and the subsequent impact on health-related quality of life, with those of patients on other combination antiretroviral therapy (cART). We conducted a cross-sectional analysis of the Veterans Aging Cohort Study from February 2008 to August 2009 to compare the symptom experiences of patients on EFV/FTC/TDF vs. other cART, unadjusted and then adjusted for treatment characteristics, and comorbid disease severity. We then assessed the association between EFV/FTC/TDF use and health-related quality of life. Among the 1,759 patients in our analytic sample, EFV/FTC/TDF use was associated with fewer symptoms than was other cART. The use of EFV/FTC/TDF was independently associated with health-related quality of life, and this association was at least partially explained by symptom burden.
Introduction
S
Despite its wide use and support, studies assessing tolerability of EFV/FTC/TDF are limited in their applicability to the general HIV-infected population. For example, study samples are younger with less advanced HIV disease and fewer comorbid illnesses. 13,15 –17 They also had relatively short follow-up. 15 –17 Alhough our previous work demonstrates that provider report is inadequate at capturing patient experiences, 10 only rare studies specifically report how adverse event data was collected 28 and rarely assess patient-centered outcomes, such as health-related quality of life (HRQoL). 15 To better understand patient experiences on EFV/FTC/TDF among an older HIV-infected population with comorbid disease, we compared symptom experiences of patients on EFV/FTC/TDF to those of patients on other antiretroviral agents and the subsequent impact on HRQoL.
Methods
Study overview
The Veterans Aging Cohort Study (VACS) is an ongoing longitudinal, multi-site study of HIV-infected and HIV-uninfected veterans, as previously described. 29 Participating sites are Los Angeles, California; Manhattan/Brooklyn, New York; Bronx, New York; Houston, Texas; Atlanta, Georgia; Baltimore, Maryland; Pittsburgh, Pennsylvania; and Washington, D.C. Data sources include the electronic medical record, the administrative record, and patient survey data. For the purposes of this analysis, we used data collected during Follow-Up 4, from February 2008 to August 2009.
Participants and procedures
Patients were approached during their regularly scheduled appointments at the Infectious Disease Clinic and asked to self-complete a written questionnaire, which included measures of symptom burden. Patients who were willing to participate and were able to provide written informed consent were enrolled in the study; there were no exclusion criteria. Permission to access their medical record and re-contact them was part of the consent process. Annual follow-up, including patient surveys, had been performed. All study sites, including the study coordinating center, received approval by their respective Internal Review Boards. Our analytic sample was restricted to patients prescribed any cART for at least 3 months with available symptom, pharmacy, and adherence data.
Independent variable: EFV/FTC/TDF vs. other cART
Using the Pharmacy Benefits Management Data, part of the electronic medical record, we were able to extract all antiretroviral agents that patients were prescribed in the 30 days prior to completing the survey. Patients were defined as being on cART if they were prescribed at least three antiretroviral agents, excluding low dose ritonavir. Patients who were prescribed EFV/FTC/TDF were included in the “EFV/FTC/TDF” group; patients who were not prescribed EFV/FTC/TDF were in the “other cART” group. In the descriptive analyses, we characterized cART regimens by protease inhibitor, NRTI or NNRTI-based regimens. In addition, we created a variable for whether patients were on their first cART regimen or not.
Dependent variables: symptom burden and HRQoL
To determine symptom burden, participants completed the HIV Symptom Index, 30 included in the VACS survey. This previously validated 30 and widely adopted questionnaire assesses the symptom burden of 20 common symptoms. Patients are asked: “The following questions ask about symptoms you might have had during the past four weeks. Please fill in the circle of the one response that best describes how much you have been bothered by each symptom.” If the symptom was present, participants are prompted to indicate the degree of bother on a five-point Likert scale. For purposes of this analysis, a symptom was considered to be present if it was reported as “bothers me a little,” “it bothers me,” or “it bothers me a lot.” A symptom was considered to be absent if it was reported as “I don't have this symptom,” or “I have this symptom and it doesn't bother me.” Symptom data were considered to be missing only if data for all symptoms were missing. If at least one symptom was noted to be present, then other symptoms were considered to be absent if the data were missing.
HRQoL was determined using the short form-12 (SF-12). 31,32 This instrument has been extensively used for a range of chronic diseases to assess patient perspectives of different components of their health. We focused on the physical component summary scale (PCS) of the SF-12, scores of which range from 0 to 100, with higher scores representing higher functioning.
Covariates
Using VACS patient survey data, laboratory data, pharmacy data, and ICD-9 codes, we obtained data on demographics, serious mental illness (SMI), hepatitis C status, VACS Index scores, 33 and cART treatment. Basic demographics, including age, gender, and race/ethnicity, were derived from patient survey data; administrative data were used if survey data was missing. Depression scores were determined based on patient completion of the Beck Depression Inventory 34 as part of the VACS survey. Scores range from 0 to 63, with higher scoring indicating more severe depressive symptoms. SMI, including major depression, anxiety, schizophrenia, and bipolar disorder, was determined based on ICD-9 codes at baseline enrollment. Hepatitis C virus (HCV) status was defined as positive if a patient had a positive HCV antibody test, HCV RNA, or ICD-9 code (070.41, 070.44, 070.51, 070.54, or V02.62). The VACS Index 33,35 is a prognostic score for all-cause mortality for treated HIV-infected patients that incorporates data on age; HIV biomarkers (HIV-1 RNA viral load; CD4 count); and non-HIV biomarkers (hemoglobin, hepatitis C or hepatitis B infection; FIB-4 to assess liver function, and estimated glomerular filtration rate to assess renal function). Scores range from 0 to 164, with higher scores being associated with a greater risk of mortality. Specifically, a five point increase in the VACS Index score is associated with an absolute 1% increase in 5-year mortality risk (e.g., from 4% to 5%). We used the VACS Index score to adjust for comorbid disease severity. The most recent laboratory tests available prior to the patient survey date were used.
Overall medication adherence to cART was calculated using the Steiner algorithm 36 to estimate the proportion of medication doses consumed based on fill and refill pharmacy data over the prior 12 months. This algorithm has been previously validated 36,37 and adopted by the VACS team 38 Scores range from 0 to 1, with 0 reflecting complete nonadherence and 1 reflecting perfect adherence. Patients were considered to be recently started on cART if they were previously cART-naïve and cART was initiated within the year prior to the survey (recent cART). Number of consecutive days on cART therapy was also determined from pharmacy data.
Data analyses
Descriptive statistics to determine the characteristics of patients prescribed EFV/FTC/TDF, in comparison to those on other cART were calculated using χ2 for categorical variables, and t-tests, or nonparametric counterpart, for continuous variables. Logistic regression models were used to determine the odds ratios (OR) for bothersome symptoms, with cART treatment group as the major independent variable. In adjusted analyses, we included the VACS Index score, cART adherence, and cART-naïve status as covariates. We then used linear regression models to assess the association between EFV/FTC/TDF use and HRQoL, unadjusted and then adjusted for total number of bothersome symptoms, disease severity based on 5 point increments of the VACS Index score, SMI, and treatment characteristics (cART adherence and recent cART).
Results
Participant characteristics
Of 2,137 HIV-infected veterans who completed Follow-Up 4 survey data, our final analytic sample included 1,759 patients. Ten patients were missing all symptom data; 368 patients lacked pharmacy data and the ability to calculate cART adherence; 7 patients were missing the parameters needed to calculate a VACS Index score. These categories were not mutually exclusive (Fig. 1). These excluded patients (18%) of the entire sample were not demographically different than the analytic sample.
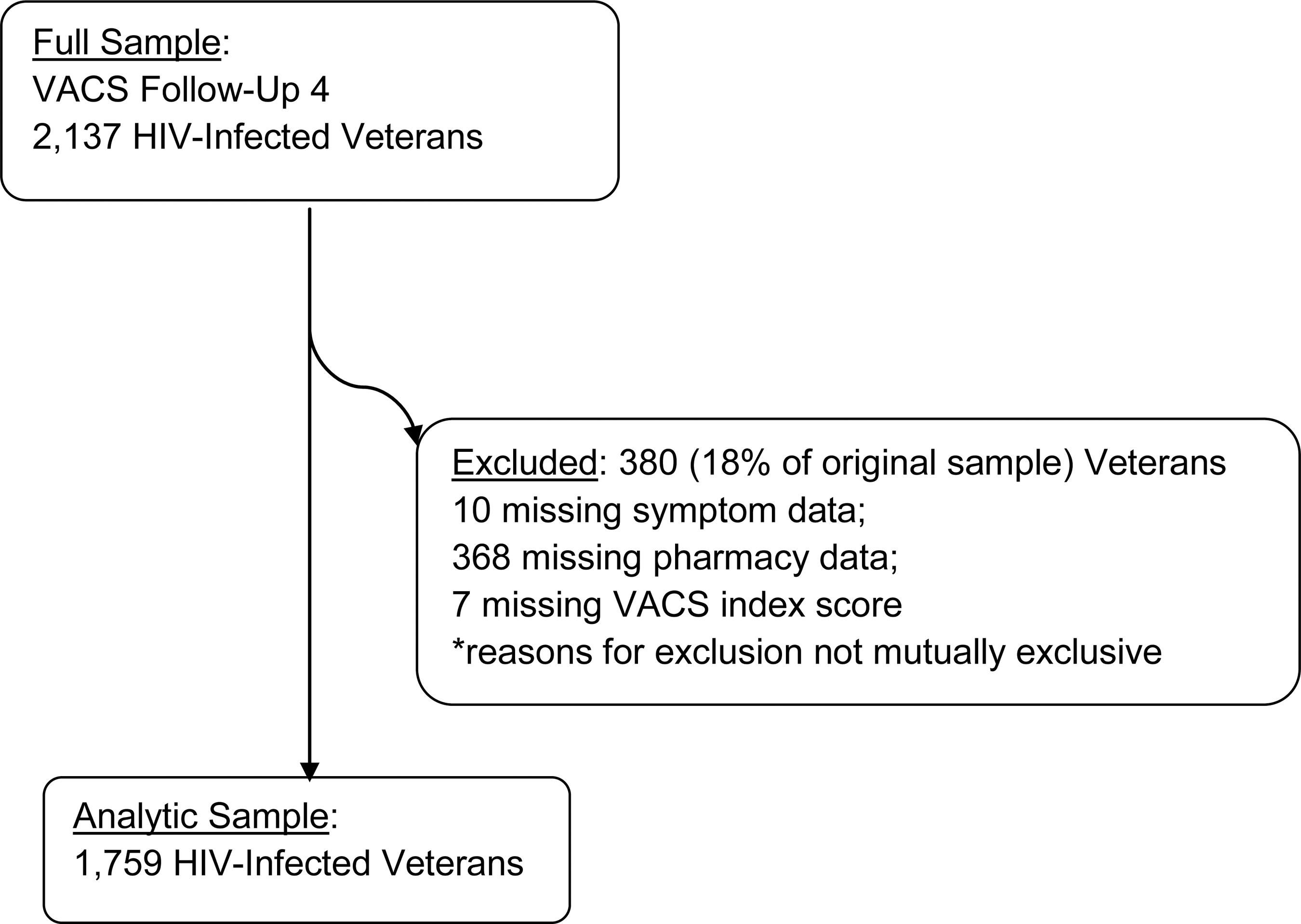
Analytic sample.
In comparison to patients on other cART, patients on EFV/FTC/TDF were less likely to be infected with HCV (36% vs. 47%, p<0.001), less likely to have psychiatric illnesses other than depression and anxiety (16% vs. 22%, p=0.003), and had lower VACS Index scores (mean 28 vs. 33, p<0.001) reflecting lower burden of the composite of HIV disease and medical comorbidities (Table 1). Patients were similar based on other characteristics, including age (mean age 53–54 years old), race/ethnicity (majority non-white), gender (98% male), Beck Depression Inventory scores (minimal depression), anxiety (5%), and cART adherence (0.8). A similar proportion of patients on EFV/FTC/TDF and other cART were on their first regimen (14% vs. 15%, p=0.65). Among those on other cART, 77% of patients were on protease-inhibitor based regimens, with ritonavir-boosted atazanavir and FTC/TDF being the most commonly prescribed individual regimen (12%) (data not shown).
Statistically significant at the p<0.05 level.
Composite of major depression, PTSD, schizophrenia, bipolar disorder and other psychosis.
EFV/FTC/TDF, efavirenz, emtricitabine, and tenofovir; cART, combination antiretroviral therapy; SD, standard deviation; VACS, Veterans Aging Cohort Study. IQR, interquartile range.
Patient-reported symptoms
Patients reported a high symptom burden. Patients on EFV/FTC/TDF had a mean of six symptoms, whereas patients on other cART had seven symptoms (p=0.01) (Table 1). Similarly, > 80% of patients in either treatment group had at least one bothersome symptom. All symptoms were less commonly reported by the patients on EFV/FTC/TDF than by those on other cART (p=0.004–0.58); the only exception was change in body composition (32% vs. 31%, p=0.62). The most common symptoms among both patients on EFV/FTC/TDF and other cART were fatigue (49% vs. 52%, p=0.31), muscle aches/pains (47% vs. 49%, p=0.58), and difficulty sleeping (46% vs. 48%, p=0.43) (Fig. 2). The least common symptoms included: nausea/vomiting (10% vs. 16%, p=0.004) and hair loss/changes (12% vs. 16%, p=0.09).
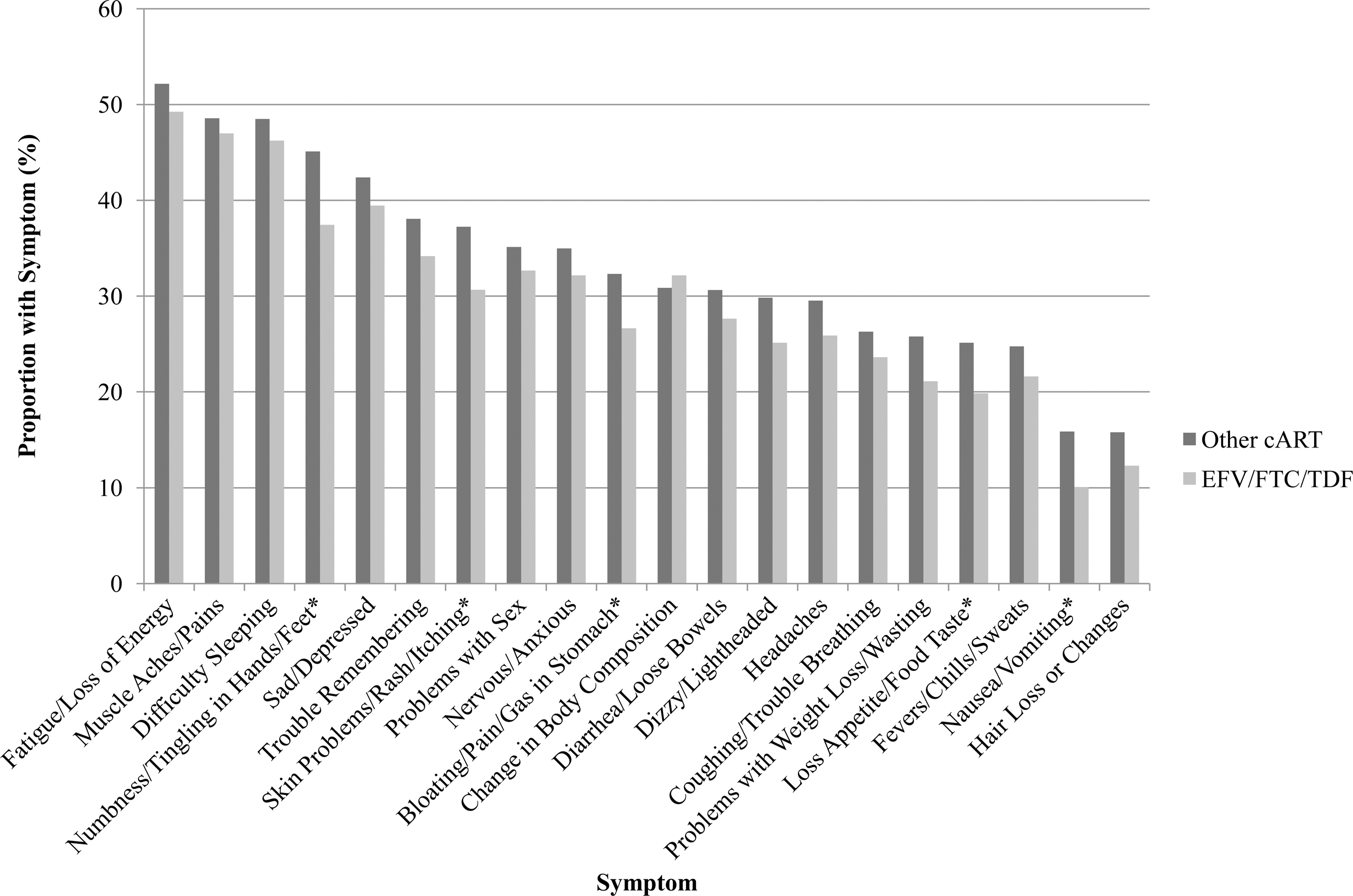
Patient-reported symptoms on efavirenz, emtricitabine, and tenofovir (EFV/FTC/TDF) versus other combination antiretroviral therapy (cART), n=1,759. Asterix (*) indicates statistical significance at p<0.05 level.
Association between symptoms and EFV/FTC/TDF
In comparison to other cART, in both unadjusted and adjusted models, EFV/FTC/TDF was generally inversely associated with symptoms (Tables 2 and 3; Figs. 2 and 3). In unadjusted models, patients on EFV/FTC/TDF were significantly less likely to report numbness/tingling in hands/feet (OR=0.73, 95% CI 0.58, 0.92), nausea/vomiting (OR=0.59, 95% CI 0.41, 0.85), skin problems/rash/itching (OR=0.74, 95% CI 0.59, 0.95), loss of appetite/food taste (OR=0.74, 95% CI 0.56, 0.97), and bloating/pain/gas in stomach (OR=0.76, 95% CI 0.59, 0.98) (Table 2). After adjusting for the VACS Index score, cART adherence and recent cART, patients on EFV/FTC/TDF continued to be significantly less likely to report numbness/tingling in hands/feet (OR=0.76, 95% CI 0.60, 0.96, p=0.02), nausea/vomiting (OR=0.61, 95% CI 0.43, 0.88, p=0.01) skin problems/rash/itching (OR=0.78, 95% CI 0.61, 0.99, p=0.04) and bloating/pain/gas in stomach (OR=0.77, 95% CI 0.60, 0.99, p=0.04) (Table 3; Fig. 3).
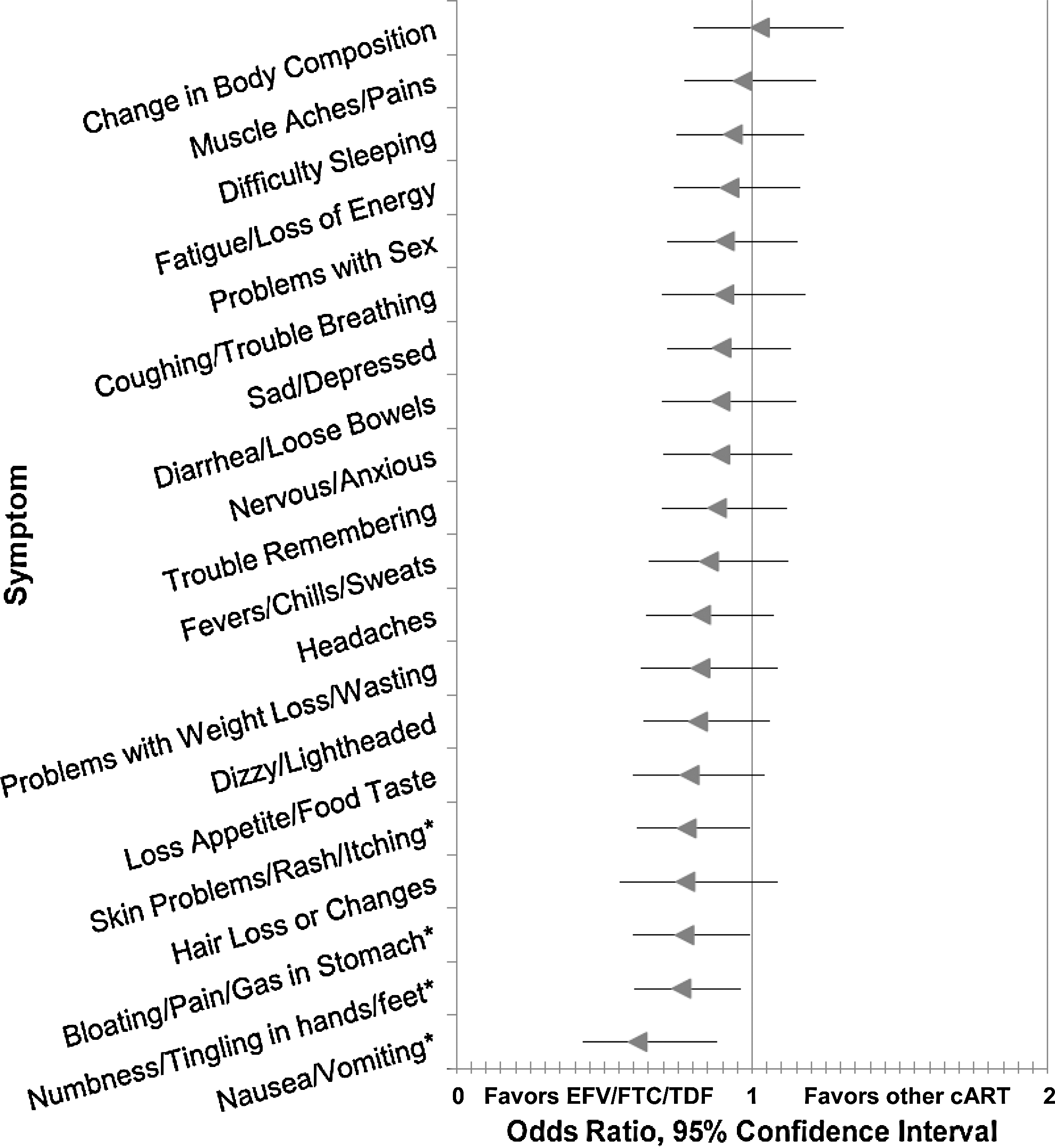
Adjusted association between efavirenz, emtricitabine and tenofovir (EFV/FTC/TDF) use and bothersome symptoms, using logistic regression (n=1,759) adjusted for Veterans Aging Cohort Study (VACS) index; combination antiretroviral therapy (cART) adherence; and cART-naïve treatment status. Asterix (*) indicates statistical significance at p<0.05 level.
EFV/FTC/TDF, efavirenz, emtricitabine, and tenofovir; cART, combination antiretroviral therapy; bold indicates statistical significance at p<0.05 level.
Adjusted for Veterans Aging Cohort Study (VACS) index score, combination antiretroviral therapy (cART) adherence, and cART-naïve status; bold text indicates statistical significance at p<0.05 level.
EFV/FTC/TDF, efavirenz, emtricitabine, and tenofovir.
Association between HRQoL and EFV/FTC/TDF
In the unadjusted linear regression model, the use of EFV/FTC/TDF was associated with improvements in HRQoL (β coefficient 2.48; 95% CI 1.26, 3.70). Patients on EFV/FTC/TDF were 19% more likely to have a higher quality of life score on average than patients on other cART even after adjusting for symptom burden, disease severity (as measured by the VACS index), treatment characteristics (cART adherence and recent cART) and serious mental illness (β coefficient 1.19; 95% CI 0.15, 2.23). This relationship was explained in part by symptom burden (β coefficient −0.94; 95% CI −1.03, −0.86), which remained significantly associated with quality of life scores after adjustment for disease severity as assessed by the VACS Index score (β coefficient −0.51; 95% CI −0.62, −0.41), and serious mental illness (β coefficient −1.37, 95% CI −2.48, −0.27) (Table 4).
EFV/FTC/TDF, efavirenz, emtricitabine, and tenofovir; HRQoL, health-related quality of life; PCS, physical component summary scale; VACS, Veterans Aging Cohort Study; cART, combination antiretroviral therapy.
Discussion
The focus of this study was to assess the symptom experiences among an older, HIV-infected population with comorbid disease when treated with EFV/FTC/TDF. We also aimed to determine and explain the association between EFV/FTC/TDF and HRQoL. Patients in the current cART era still suffer from a high burden of symptoms. In this older HIV-infected cohort with comorbid disease, the use of EFV/ FTC/TDF was associated with fewer symptoms than other antiretroviral agents. Specifically, we found that five symptoms were significantly less common among patients on EFV/FTC/TDF. This association persisted for all but one symptom after adjusting for differences in disease severity. The relationship between HRQoL and EFV/FTC/TDF appears to be at least partially mediated through bothersome symptoms, a relationship that persisted after adjusting for disease severity, treatment characteristics, and serious mental illness.
The high symptom burden reported by our patients is not surprising. 1,7,10,39 –41 This pattern, however, may reflect a shifting balance in symptom etiology as associated treatment toxicities decrease and comorbidities increase. 42 –45 For example, diarrhea/loose bowels was reported half as commonly in our current population as in a similar group from an earlier treatment era, 10 perhaps reflecting a shift away from use of older antiretroviral agents, such as nelfinavir, 1,46,47 higher to lower dose ritonavir, and possibly better symptomatic management of side effects.
The use of EFV/FTC/TDF, compared with other antiretroviral agents, was generally protective across all symptoms. This association was statistically significant for numbness/tingling in hands/feet; nausea/vomiting; skin problems/rash itching, loss of appetite/food taste and bloating/pain/gas in stomach; a relationship that persisted for four of these five symptoms after adjusting for disease severity with the VACS Index score and treatment characteristics, including cART adherence and recent cART. These findings are consistent with the Department of Health and Human Services (DHHS) treatment guidelines, which rely on data from randomized controlled trials; only limited side effects are reported for the components of EFV/FTC/TDF, 20 including neuropsychiatric side effects with EFV. 48 A lower proportion of participants had serious mental illness in the EFV/FTC/TDF than in other cART group (16% vs. 22%), possibly explained by providers' avoidance of efavirenz among patients likely to experience the well-known side effect of neuropsychiatric complications. Other listed potential side effects in the DHHS guidelines would not necessarily be symptomatic (dyslipidemia with EFV, renal impairment, or decrease in bone mineral density with FTC/TDF). 20 In contrast, stavudine and didanosine, 20 associated with peripheral neuropathy, were each currently prescribed for 4% of our sample, perhaps contributing to this difference in this symptom by treatment group. Similarly, the nucleoside reverse transcriptase inhibitors, particularly didanosine and zidovudine, as well as protease-inhibitor-based regimens, 20 are known to be associated with gastrointestinal complaints.
Skin problems/rash/itching was significantly less common among patients on EFV/FTC/TDF in the unadjusted and adjusted analyses. This may be explained by the fact that rash is an early complication of efavirenz use and patients are usually discontinued from the drug if it is persistent. In addition, protease inhibitors, including atazanavir, are also associated with rash. Notably, atazanavir was a component of the most commonly prescribed regimen among patients not on EFV/FTC/TDF. Moreover, the known association between liver disease, and HCV in particular, with skin manifestations may be contributing to our results, given the higher proportion of patients with HCV (47% vs. 36%) and higher VACS Index scores (33 vs. 28) in the other cART group, compared with those on EFV/FTC/TDF. Given the extensive use 23 of and support 20 for EFV/FTC/TDF, it is reassuring that we did not find unexpected symptoms associated with its use in a population engaged in routine clinical care.
It was similarly encouraging to find that EFV/FTC/TDF use is associated with HRQoL (adjusted β coefficient 1.19; 95% CI 0.15, 2.23), which may be because of the medication or associated with the characteristics of patients more likely to be prescribed this regimen. In addition, for each avoided bothersome symptom, there was an associated increase by almost one point in HRQoL (β estimate −0.94, 95% CI −1.03, −0.86), consistent with the recognized impact of symptoms on HRQoL. 4 –9 Of note, a three to five point increase in this score represents a clinically important difference, 49 highlighting the importance of symptom management to improve HRQoL. In our analyses, disease severity based on five point increases in the VACS Index 33,45 was also associated with HRQoL (β estimate −0.51, 95% CI −0.62, −0.41) as was serious mental illness (β estimate −1.37, 95% CI −2.48, −0.27). 50
Our study did not reveal any surprises with regard to patient-reported symptoms on EFV/FTC/TDF in comparison with other antiretroviral agents. Studies such as these, however, are increasingly important. They allow for evaluation of medications post-FDA approval 51 in a population that more accurately reflects a routine clinical population, in comparison with those who participate in randomized controlled trials. Certainly as the HIV-infected population continues to age, with a rising number of comorbidities, and treatment guidelines evolve that encourage earlier and earlier initiation of therapy, assessing symptom tolerability is critical as patients may require decades of antiretroviral therapy. As more once-daily treatment options 52 and novel agents become available, patient-reported symptoms should be included as a central assessment of tolerability.
Our study has several notable strengths. First, our sample, representing an older population (mean age >50 years old) with comorbid disease in clinical care, provides data to inform the care of the aging HIV-infected population. As a multi-site study from eight different sites, which are part of the system that serves the greatest number of HIV-infected patients in the United States, 29 these findings are likely generalizable to HIV-infected veterans. For symptom assessment, we relied on a validated 30 and extensively adapted tool. Moreover, we collected data through patient self-report, which represents the gold standard, 10,53 as provider report has been previously demonstrated to underreport symptoms and miss clinically relevant ones. 10
In contrast, there are limitations to our study. Our population consisted almost entirely of males in care, limiting the generalizability to the other patients, including women. This group, however, has been shown to be similar to others based on clinically relevant variables. 54,55 Moreover, a comparison of symptom reporting among veterans and non-veterans in the HIV Cost and Service Utilization Study demonstrated similar patterns. 56 We did not compare patients on EFV/FTC/TDF to those on a particular cART regimen, and therefore may have missed differences among different subgroups. New antiretroviral agents that are well tolerated, such as raltegravir, were not being used in the other cART group during the time frame of this study. There may be asymptomatic side effects and toxicities, such as renal disease and bone mineral density loss, known to be associated with tenofovir, which this study was not designed to capture. 24 –26,57 Finally, as we conducted a cross-sectional analysis, we are unable to determine whether the medications were causing the different symptom profiles or if there were underlying differences in the symptom experiences of the patients at baseline, which may have impacted prescribing decisions. However, that the associations between cART regimen and symptoms remained largely unchanged even after adjusting for disease severity and treatment characteristics, suggests that the relationship is, in fact, related to differences in cART regimens and not underlying characteristics of the clinical population.
Based on patient-reported symptoms, our findings support the use of EFV/FTC/TDF as the first-line regimen for treatment-naïve patients, consistent with the current guidelines as well as its tolerability for treatment-experienced patients when compared with other regimens. We encourage the use of similar analyses as novel antiretroviral agents and formulations become available, to better inform patient-centered treatment decisions. Future work should include longitudinal analyses to more clearly define these associations between symptom experiences and cART regimens in older populations presenting for routine clinical care.
Footnotes
Acknowledgments
This work was generously supported by the Robert Wood Johnson Foundation Clinical Scholars Program, the Department of Veteran Affairs, and the Veterans Aging Cohort Study funded by the National Institute on Alcohol Abuse and Alcoholism (U10 AA 13566).
Author Disclosure Statement
No competing financial interests exist.
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
This work was presented in earlier versions at the Robert Wood Johnson Clinical Scholars National Meeting, November 3rd, 2010, Atlanta, Georgia, and at the Society for General Internal Medicine National Annual Meeting. May 6th, 2011, Phoenix, Arizona.