
Abstract
Low 25-hydroxyvitamin D levels are common in the general and HIV-infected populations alike. Defined as levels less than 30 ng/mL, suboptimal vitamin D is known to afflict over 70% of representative samples from each group in resource-rich countries with even greater prevalence in resource-poor regions of the world. In both those with and without HIV, dark skin, low vitamin D intake, exiguous exposure to sunlight, and season act as risk factors for suboptimal vitamin D levels. In those infected with HIV, antiretroviral therapy, particularly non-nucleoside reverse transcriptase inhibitors (NNRTIs), increase risk for low vitamin D as well. Furthermore, metabolic aberrations, including obesity and hyperlipidemia, and miscellaneous risk factors, such as advanced AIDS and substance abuse, have been linked to suboptimal vitamin D in those with HIV. While the skeletal and cardiovascular systems of HIV patients may be adversely impacted as a result of low levels, recent data have also linked low vitamin D to decreased CD4 counts, higher viral loads, and to critical end points including progression to AIDS events and death. More research is needed to confirm these potential consequences of low vitamin D in those with HIV and to discern the benefits of routine screening for and treatment of low vitamin D in this population.
Introduction
S

Illustration of vitamin D metabolism in the human body. Adapted from Deeb et al. 54 UV B light, ultraviolet B light; PTH, parathyroid hormone; FGF-23, fibroblast growth factor-23.
Scope of the Problem
Low vitamin D is a common condition throughout the world and has become increasingly recognized in recent years. Data from NHANES-III in the United States indicate that 77% of adults have vitamin D insufficiency while as many as 6% have severe deficiency. 8 Likewise, other evidence of broadly sampled populations indicate vitamin D deficiency is also common with up to 40% of the population affected. 9 This problem is magnified in African Americans. Those with HIV are not exempt. In a mixed cohort of HIV-infected men and women in New York City, for instance, 68% of patients were found to have vitamin D insufficiency while 28% were found to have vitamin D deficiency. 10 A similar study performed in Boston found rates of severe deficiency to be 10.5% among the HIV-infected population. 11 African Americans were significantly more likely to have low vitamin D than Caucasians in both of these analyses. Regarding gender, it also appears suboptimal vitamin D is more common in HIV-infected women than men. One cohort of HIV-infected women, for example, revealed a 60% prevalence of vitamin D deficiency compared to a 20% prevalence found in a separate cohort of HIV-infected men. 12,13 Residing in southern latitudes may not ameliorate this trend, as rates of vitamin D deficiency as high as 65% were found in a mixed group of HIV patients in Texas. 14 However, despite these disparaging numbers in those with HIV, when HIV-infected patients are compared to the general population in a single cohort, it has been shown that the prevalence of low vitamin D (≤30 ng/mL) is no greater in the HIV-infected population (70% HIV-infected compared to 79% uninfected). 15
Risk Factors for Low Vitamin D Levels in HIV Patients
The ubiquitous nature of low vitamin D has acted as an impetus for further study of risk factors associated with the condition both in the general and HIV-infected populations. Given the effect of sunlight on conversion of dehydrocholesterol to vitamin D3 in the skin, 16 it is not surprising that season, 17 dark skin, 10,11 and lack of exposure to sunlight 18 are associated with low vitamin D in the general and HIV-infected populations alike, although latitude, paradoxically, has not been clearly linked to low vitamin D in those with HIV, 14,19 as previously discussed. Suboptimal intake of vitamin D is also associated with low levels. 14 However, given the complexity of HIV infection, copious risk factors have emerged for low vitamin D, specifically certain antiretroviral medications, metabolic aberrations, and various miscellaneous conditions.
Antiretroviral associations
Exposure to antiretroviral therapy has emerged as a risk for low vitamin D. Specifically, although no stratification for class of antiretroviral drug was undertaken, duration of ART 3 years or more predicted vitamin D insufficiency in a study of HIV-infected women. 19 This relationship remained upon controlling for multiple alternative predictors. However, when specific classes of antiretrovirals are considered, the preponderance of evidence suggests non-nucleoside reverse transcriptase inhibitors (NNRTIs) are the predominant culprit, likely related to their penchant to induce hepatic microsomal enzymes through the pregnane X receptor similar to barbiturates. 20
As a group, NNRTIs have been shown to be more likely to contribute to risk for low vitamin D than other antiretrovirals (adjusted odds ratio [AOR] 6.62; 95% confidence interval [CI] 1.91–22.89, p=0.0017). 13 The NNRTI with the most consistent association with low vitamin D is efavirenz. After controlling for ethnicity, geographical site, body mass index, age, and HIV severity, one study found efavirenz to be an independent risk for vitamin D insufficiency (AOR 1.98; 95% CI 1.18–3.34). 15 Likewise, in a group of patients followed prospectively after starting antiretroviral therapy, vitamin D levels were found to decrease significantly more in the efavirenz group than the alternative antiretroviral group (average decrease in the efavirenz group of 12.7±3.7 nmol/l, p=0.001). 21 Furthermore, in evaluating the efficacy of boosted darunavir in the MONET trial, efavirenz was found more likely to be related to vitamin D deficiency at baseline than other antiretrovirals (Parameter estimate −6.00; 95% CI −1.05 to −10.95, p=0.0062), and it was discovered, in turn, that changing the antiretroviral base from efavirenz to boosted darunavir was associated with increases in vitamin D. 22 However, the relationship between nevirapine and vitamin D is less consistent with some evidence suggesting this medicine is related to low levels 23 and other evidence suggesting it is not. 24 Regardless, the propensity of nevirapine to lower vitamin D appears to be less than efavirenz. In a secondary analysis of the Swiss HIV cohort study, it was demonstrated that levels of vitamin D were more often sufficient in the nevirapine group than the efavirenz group (17.9% versus 5.4%, p=0.05). 25 The data on the effects of etravirine is in its infancy, although the relationship between this second-generation NNRTI and vitamin D may be similar to efavirenz. 26 Data on vitamin D and rilpivirine await systematic study.
Regarding the protease inhibitor (PI) class, these medicines as a group have been implicated in bone health; however, these effects appear independent of vitamin D. In fact, possibly related to their proclivity for inhibition of hepatic microenzymes, PIs may be protective with regard to developing inadequate vitamin D. In a study that evaluated women with HIV, for instance, exposure to PIs was shown to impart a reduced risk of vitamin D deficiency (AOR 0.67; 95% CI 0.48–0.95, p=0.025). 12 Likewise, another analysis found a 44% decreased risk of vitamin D insufficiency if exposed specifically to ritonavir (AOR 0.56; 95% CI 0.35–0.89). 15 Thus, PIs appear less likely to be associated with low vitamin D than other antiretrovirals and may be protective.
The NRTI class has been associated with alterations in skeletal health as well, particularly the nucleotide analogue tenofovir, 27,28 but, like the PIs, these effects appear independent of vitamin D. While tenofovir has been linked to secondary hyperparathyroidism specifically, this medicine has not been linked to low vitamin D. 24,27,28 One analysis specifically compared levels of vitamin D in patients before and after starting tenofovir and found no significant change in levels (p=0.665). 23 Zidovudine, however, unlike other medicines in this class, has been shown to be a risk for vitamin D deficiency. 22
In summary, considering the data available for all ART, the most robust association between these medicines and low vitamin D is with the NNRTI class, namely efavirenz. Duration of implicated medicines 3 years or more particularly increases risk. PIs appear unrelated to low vitamin D levels. Likewise, the NRTI class does not appear to be associated conclusively with low vitamin D, although zidovudine may be an exception. Further study is necessary to elucidate the relationship between etravirine and rilpivirine and vitamin D.
Metabolic associations
Although the pathophysiology is not fully elaborated, various metabolic correlates of vitamin D deficiency have begun to emerge. The data is preliminary, but potential areas of concern are high body mass index (BMI) and total body fat and hypercholesterolemia.
In a large Swiss HIV cohort, being overweight (BMI≥25kg/m2) was associated with low vitamin D. 17 These results were later replicated in the study by Crutchley et al. 14 who again found a high BMI predicted vitamin D deficiency. In contrast, if body weight is below average (the equivalent of<70 kg in a man), perhaps reflecting global malnutrition, vitamin D levels may also be suboptimal. 23 Finally, after controlling for antiretroviral regimen, elevated triglycerides, and elevated low density lipoprotein levels, elevated total cholesterol was also found to be associated with vitamin D deficiency (AOR 2.07; 95% CI 1.16–3.70, p=0.013). 19
Thus, factors associated with the metabolic syndrome including BMI and hypercholesterolemia are potential risks for low vitamin D. In contrast, extremely low body weight may also be a risk as a result of poor nutrition.
Miscellaneous associations
Less studied potential risk factors for inadequate vitamin D in the HIV-infected population are detectable viral loads, 10 presence of AIDS, 12,29 injection drug use, 17 sedentary lifestyle, 15 tobacco use, 13 and lactose intolerance. 11 Although the progression of hepatitis C fibrosis in the HIV patient may be related to low vitamin D, the presence of comorbid hepatitis C has not been associated with low vitamin D. 17,30
In summary, NNRTI use and the metabolic syndrome may be associated with low vitamin D levels as are factors such as advanced AIDS and substance abuse. In addition, risks for low vitamin D in the general population, such as dark skin, poor vitamin D intake, and exiguous sunlight exposure, also contribute to risk in the HIV-infected population. More data are needed for the novel NNRTIs and the metabolic risk factors as mediators of vitamin D levels in those with HIV. While screening for low vitamin can be considered for HIV patients, additional research is needed before widespread recommendations can be made. Table 1 enumerates the risk factors for low vitamin D.
HIV, human immunodeficiency virus; vit D, vitamin D; ART, antiretroviral therapy; NNRTI, non-nucleoside reverse transcriptase inhibitor; IDU, intravenous drug use; BMI, body mass index; EFV, efavirenz; ESR, erythrocyte sedimentation rate; RR, risk ratio; PI, protease inhibitor; WIHS, Women's Interagency HIV Study; VL, viral load; ZDV, zidovudine; DRV/RTV, darunavir/ritonavir; RTV, ritonavir; NVP, nevirapine; AOR, adjusted odds ratio; 95% CI, 95% confidence interval; NS, not significant.
Potential Consequences of Low Vitamin D Levels in HIV Patients
Low vitamin D is common in the HIV-infected population given the multitude of risk factors for suboptimal levels that these patients share. Data are beginning to suggest that suboptimal levels may contribute to various clinical maladies that have heretofore been unknown to be related to vitamin D. While more information is likely to emerge in the next several years about vitamin D on other aspects of health, the best studied potential consequences of suboptimal vitamin D in the HIV-infected population are as follows.
Endocrinologic consequences
Given its intricate association with bone metabolism, it is no surprise that low vitamin D is associated with osteoporosis in the general population. 31 Less intuitively, low vitamin D has been linked to the presence diabetes mellitus in those without HIV. Suboptimal vitamin D also appears related to decreased bone mineral density (BMD) and diabetes mellitus in those with HIV.
In a cohort of HIV-infected males, some of whom were prescribed ART and some of whom were not, the prevalence of osteopenia was found to be 50% while the prevalence of osteoporosis was noted to be 12%, both significantly greater than the national average. Although vitamin D levels were not a specific predictor in the multivariate model, more than 80% of the sample was found to be vitamin D deficient. 32 In a study focusing on HIV-infected premenopausal women, BMD was found to decrease more rapidly in those infected with HIV compared to those unaffected, and vitamin D deficiency was linked to loss of bone density at the femoral neck in particular (p=0.011), even after adjusting for body weight and alcohol use. 34
While various aspects of the metabolic syndrome, such as obesity, may contribute to risk for low vitamin D in those with HIV, as in the general population, the presence of hyperglycemia and diabetes may be a potential consequence of low vitamin D. In a cross-sectional study performed in HIV-infected patients in Italy, for instance, after controlling for body weight, vitamin D deficiency was found to be an independent predictor of the presence of diabetes mellitus (AOR 1.85; 95% CI 1.03–3.32, p=0.038). 35
As a result, those with HIV may experience accelerated BMD decline when vitamin D levels are suboptimal. Given additional clinical entities in HIV patients that potentially synergize with low vitamin D to create low BMD, osteoporosis and osteopenia have become more common in the HIV-infected population than the general population 36 and have become two of the most important clinical consequences in the aging HIV-infected population, leading to increased risk of fractures. 37 Furthermore, while obesity increases risk for low vitamin D, low vitamin D may also contribute to risk of diabetes mellitus in both those with and without HIV.
Cardiovascular consequences
Although the pathophysiologic mechanism is not clear, suboptimal vitamin D levels have been found to be a risk for cardiovascular disease in the general population, and this relationship has persisted despite controlling for traditional risk factors. 38 Those with HIV have an increased prevalence of cardiovascular disease compared to those uninfected 39 ; research also suggests that the presence of low vitamin D may further modulate risk.
In a predominantly male population of HIV patients, those with vitamin D insufficiency were more likely to have coronary artery calcium, a surrogate measure of coronary artery disease (relative risk [RR] 1.02, p=0.04), as well as disrupted function in peripheral arteries as measured by brachial artery flow-mediated dilation. 40 After controlling for cardiovascular risk factors such as age, sex, hypertension, cholesterol level, and smoking, Choi and colleagues 41 found vitamin D insufficiency to be associated with increased carotid intima-media thickness. In addition, in a similar cross-sectional study of HIV patients, those with elevated carotid intima-media thickness were also more likely to have vitamin D insufficiency (OR 10.62; 95% CI 1.37–82.34, p<0.01), again suggesting a link between vitamin D and cardiovascular dysfunction. 42 Finally, in an observational study of African Americans with HIV, after controlling for Framingham risk, age, gender, hyperlipidemia, and use of antiretrovirals, vitamin D deficiency predicted asymptomatic coronary stenosis of 50% or more by computed tomographic (CT) coronary angiography (AOR 2.28; 95% CI 1.23–4.21). 43
Therefore, while there are no data linking vitamin D to symptomatic cardiovascular disease in HIV patients, studies that employ surrogate measures of cardiovascular disease suggest that low vitamin D could be a risk for symptomatic cardiovascular disease. Further study with definitive end points such as myocardial infarction is needed to ascertain the relationship between vitamin D and cardiovascular disease in HIV patients.
Immunologic, virologic, and related clinical consequences
Polymorphisms in the vitamin D receptor contribute to risk of HIV acquisition upon exposure as well as to subsequent progression after the disease is contracted. 44,45 Furthermore, the active form of vitamin D, 1,25-dihydroxyvitamin D, mediates autophagy in mononuclear cells, a manner through which the HIV virus may be eradicated in these effectors of the immune system. 46 As a result, it follows that suboptimal vitamin D levels could be related to immunologic and virologic consequences in HIV patients.
Regarding HIV status and vitamin sufficiency in general, initial work was executed in resource-limited countries and demonstrated that administration of multivitamins that did not contain vitamin D decreased the rates of AIDS-associated deaths, led to higher CD4 counts, and decreased viral loads. 47 From this work, it is unclear if this effect were related to improvement in nutritional status or if a specific vitamin imparted a unique effect to the immune system. This work, however, along with basic science research on vitamin D, 44 –46 has become the impetus for systematic study of the role of this vitamin on HIV progression.
Higher vitamin D intake was initially found to be associated with higher CD4 counts in a study on combined vitamin A and D supplementation. Only vitamin D intake correlated with CD4 counts in multivariate analysis, however, in contrast to vitamin A. 48 Furthermore, in another analysis, after controlling for multiple potential confounders by multivariate logistic regression, vitamin D sufficiency was also linked to achievement of higher CD4 counts and immune reconstitution after starting ART (p<0.01). 42
Vitamin D has also been shown to have a relationship to clinical outcomes. A study conducted in Tanzania showed increased rates of oral candidiasis (hazard ratio [HR] 2.74; 95% CI 1.29–5.83) and upper respiratory infection (HR 1.27; 95% CI 1.04–1.54) in those with lower vitamin D (≤32 ng/mL). 49 Another analysis found no association of vitamin D with CD4 count; however, progression to World Health Organization (WHO) stage III or beyond was related to insufficient vitamin D (RR 1.25; 95% CI 1.05–1.50, p=0.01). Furthermore, those with the highest levels of vitamin D (defined as the highest quintile in the study) were less likely to die at follow up after controlling for age, CD4 count, and initial WHO class (RR 0.58; 95% CI 0.40–0.84, p=0.01). 50 Likewise, in a secondary analysis of the Eurosida study that followed patients prospectively for 5 years, individuals were less likely to die who had vitamin D levels between 12–30 ng/mL compared to those with levels less than 12 ng/mL (RR 0.68; 95% CI 0.47–0.99, p=0.045). In addition, those with levels less than 12 ng/mL were more likely to develop clinical AIDS while there was a trend for those with levels this low to progress to non-AIDS events (defined as cardiovascular events, non-AIDS cancers, liver disease, pancreatitis, and end-stage renal disease). 51 The bivariate time-to-event analysis is in Fig. 2.
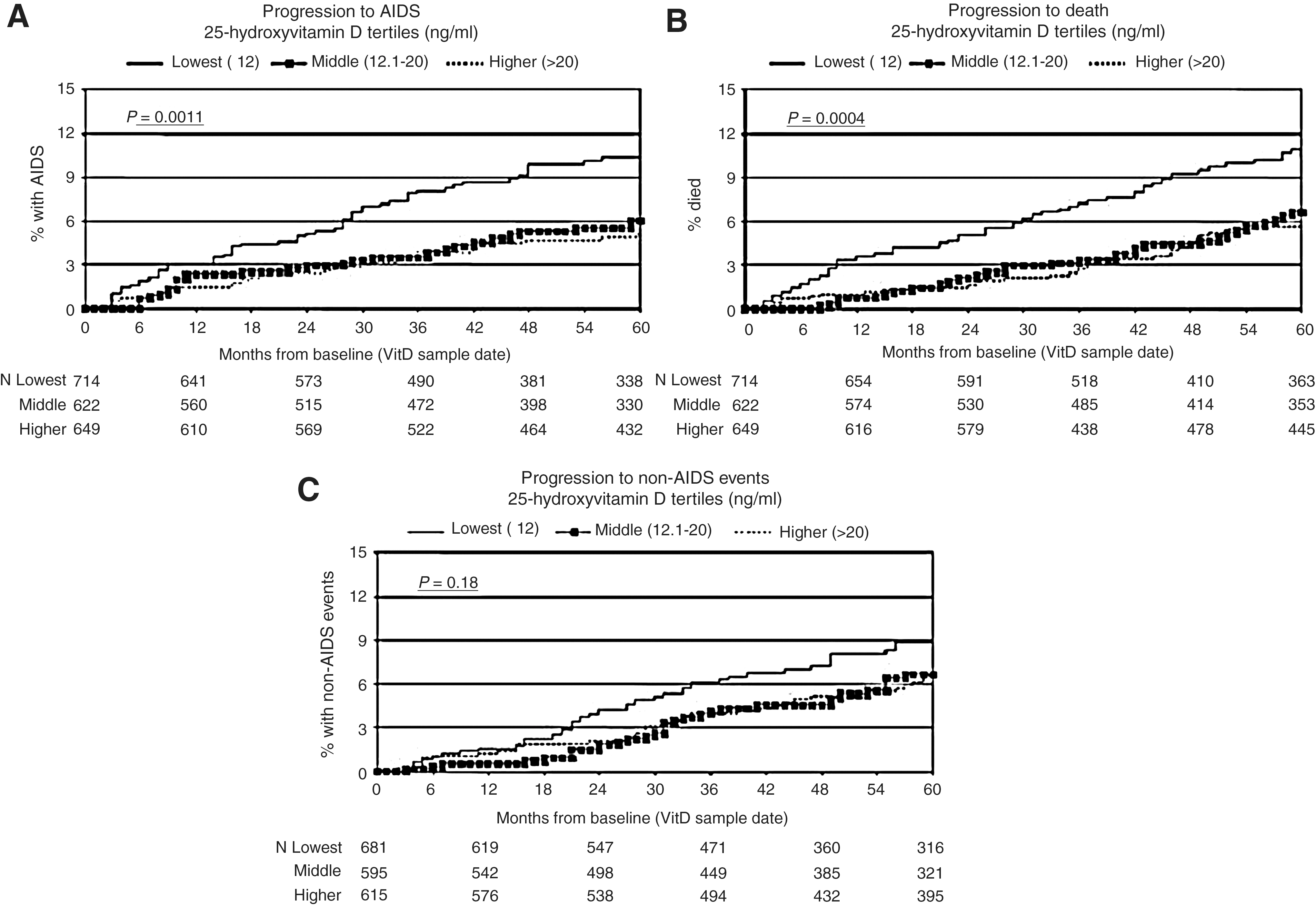
Kaplan-Meier curves comparing those with vitamin D levels less than 12 ng/mL to those with levels between 12–20 ng/mL and greater than 30 ng/mL, respectively, based on (
Thus, possibly related to effects on mononuclear cells and inadequate interaction with the vitamin D receptor with lower levels of vitamin D, low vitamin D may be associated with decreased CD4 counts and higher viral loads. Furthermore, inadequate vitamin D levels may modulate outcomes including progression to AIDS and death. Clinical progression appears to be most evident in those with levels less than 12 ng/mL. Future controlled research is unequivocally needed to confirm these associations, particularly the suggestion of increased mortality. While widespread screening of HIV patients for low vitamin D cannot be recommended based on this evidence alone, clinicians should consider vitamin D as a potential variable modulating outcomes in HIV and screen on a case-by-case basis. Table 2 enumerates the potential consequences of low vitamin D.
HIV, human immunodeficiency virus; vit D, vitamin D; CAC, coronary artery calcium; FMD, flow-mediated dilation; ART, antiretroviral therapy; cIMT, carotid intima-media thickness; MVI, multivitamin; WHO, World Health Organization; AIDS, acquired immunodeficiency syndrome; WIHS, Women's Interagency HIV Study; BV, bacterial vaginosis; AOR, adjusted odds ratio; RR, relative risk; HR, hazard ratio; AIRR, adjusted incidence rate ratio; 95% CI, 95% confidence interval.
In conclusion, low vitamin D is prevalent in the general and HIV-infected populations alike. The NNRTI class appears to be a major risk for suboptimal vitamin D levels in those with HIV. Metabolic aberrations, including hypercholesterolemia and obesity, may further mitigate risk. As in the general population, osteoporosis, osteopenia, and subsequent fractures may be related to vitamin D deficiency in those with HIV. Furthermore, surrogate markers of cardiovascular disease presence, such as presence of coronary artery calcium, have been related to low vitamin D. In addition, intriguing research has begun to suggest associations between inadequate vitamin D and lower CD4 counts, higher viral loads, and progression to AIDS events, even death, particularly as vitamin D levels become severely deficient.
More study is needed, particularly employing clinical endpoints, in elucidating the relationship between vitamin D and cardiovascular risk in the HIV-infected population. Furthermore, replication of previous work suggesting the association of vitamin D, mortality, and AIDS events is warranted. The optimal level of vitamin D to achieve in the HIV patient and the best method of replacement also deserve further study. Given that the research on the effects of vitamin D on outcomes in HIV is preliminary, additional research is needed before recommendations on widespread screening and treatment that would differ from the general population can be made for those infected with HIV. However, as with all patients, in order to prevent deficiency in those with HIV, clinicians should recommend an average daily intake of vitamin D of 600 IU for those less than 70 years and 800 IU for those greater than 70 years, as recommended by the Institute of Medicine. 52
Footnotes
Acknowledgments
The authors would like to thank Elizabeth Smigielski, M.S.L.S., assistant director of the Kornhauser Health Sciences Library in Louisville, KY, for assistance.
Author Disclosure Statement
No competing financial interests exist.