
Abstract
Crystal methamphetamine use is a major driver behind high-risk sexual behavior among men who have sex with men (MSM). Prior work suggests a cycle of continued crystal methamphetamine use and high-risk sex due to loss of the ability to enjoy other activities, which appears to be a side effect of this drug. Behavioral activation (BA) is a treatment for depression that involves learning to reengage in life's activities. We evaluated a novel intervention for crystal methamphetamine abuse and high-risk sex in MSM, incorporating 10 sessions of BA with integrated HIV risk reduction counseling (RR). Forty-four subjects were screened, of whom 21 met initial entry criteria. A total of 19 participants enrolled; 16 completed an open-phase study of the intervention. Behavioral assessments were conducted at baseline, 3 months postbaseline, and 6 months postbaseline. Linear mixed effects regression models were fit to assess change over time. Mean unprotected anal intercourse (UAI) episodes decreased significantly from baseline to acute postintervention (β=−4.86; 95% confidence interval [CI]=−7.48, −2.24; p=0.0015) and from baseline to 6 months postbaseline (β=−5.07; 95% CI=−7.85, −2.29; p=0.0017; test of fixed effects χ2=16.59; df=2,13; p=0.0002). On average, there was a significant decrease over time in the number of crystal methamphetamine episodes in the past 3 months (χ2=22.43; df=2,15; p<0.0001), and the number of days of crystal methamphetamine use in the past 30 days (χ2=9.21; df=2,15; p=0.010). Statistically significant reductions in depressive symptoms and poly-substance use were also maintained. Adding behavioral activation to risk reduction counseling for MSM with problematic crystal methamphetamine use may augment the potency of a risk reduction intervention for this population. Due to the small sample size and time intensive intervention, future testing in a randomized design is necessary to determine efficacy, with subsequent effectiveness testing.
Introduction
M
In the United States, crystal methamphetamine (crystal meth) use is endemic among urban MSM. 5 –12 The prevalence of crystal methamphetamine use among sexually active MSM has been shown to be 20 times that of the general population, with an estimated 10–20% of sexually active, nonmonogamous MSM reporting crystal methamphetamine use in the past 6 months. 13 –18 Baseline data from the EXPLORE study (a large-scale, multisite behavioral intervention that enrolled 4295 HIV-uninfected MSM between 1999–2002) revealed that 13% of participants reported using crystal methamphetamine in the previous 6 months. 19,20 This study also found that, from baseline through follow-up, 28% of the enrolled MSM reported at least one episode of crystal methamphetamine use. 21 Crystal methamphetamine, a highly addictive psychostimulant, remains extremely affordable, relatively simple to manufacture, and easy to obtain, 22 causing a broad and negative impact on public health nationwide 23,24 —in particular among U.S. MSM.
A number of studies have documented that crystal methamphetamine use (versus non-use) is associated with higher numbers of sexual partners, as well as increased HIV sexual risk taking among MSM. 16,21,22,25 –33 A study of 2172 MSM found that recreational drug use, particularly crystal methamphetamine, was highly prevalent among urban MSM (52%) and independently associated with risky sexual practices. 33 Baseline data from the EXPLORE cohort demonstrated that crystal methamphetamine use was significantly associated with unprotected sex. 20 Given research reporting that the primary medical correlate of crystal methamphetamine use is HIV infection 34 HIV-uninfected MSM who use crystal methamphetamine at levels garnering an abuse or dependence diagnosis are at exceptionally high risk for HIV acquisition, largely due to the frequently concomitant drug-associated sexual risk behaviors. 35
Our formative work 5 showed that an important consequence of continued crystal methamphetamine use is anhedonia—loss of interest in previously enjoyed activities that do not involve drug use—one of the chief symptoms of depression. Accordingly, crystal methamphetamine use appears to become a central means for enjoyment in MSM who routinely abuse crystal methamphetamine, hence causing a cycle of continued use as the only means for enjoyment. We hypothesized that an intervention addressing both sexual risk reduction and crystal methamphetamine abuse, that helps individuals relearn how to enjoy safe but pleasurable activities that do not involve drug use, will increase intervention efficacy for HIV risk reduction and reduce crystal methamphetamine use. Behavioral activation is an empirically supported treatment for depressed mood that helps patients gradually increase goal-directed potentially rewarding and pleasurable activities. 36 –38 For the current study, the underlying conceptual model is that behavioral activation will reengage participants in pleasurable non-drug use activities (e.g., interests or hobbies that were enjoyable before crystal methamphetamine use) that will serve as a naturally occurring reinforcer for more adaptive behavior, improve depressed mood when not on crystal methamphetamine by experiencing increases in pleasure and mastery, and decrease overall distress so that MSM who abuse crystal methamphetamine can better benefit from HIV risk reduction counseling. Accordingly, we developed the intervention, and present the results of a demonstration trial below.
Methods
Sampling, recruitment, and eligibility
Between June 2008 and November 2009, HIV-uninfected MSM were enrolled in Project IMPACT (Intervention with MSM to Prevent Acquisition of HIV through Crystal methamphetamine Treatment), a demonstration study addressing HIV sexual risk behavior and concomitant crystal methamphetamine use. Purposive sampling 39 was used to recruit the target population of men by posting study flyers from community-based health centers, substance use programs, bars/nightclubs and the Internet. Eligibility criteria were: (1) age 18 or older; (2) self-reported one or more episode of unprotected anal sex (insertive or receptive) with a nonmonogamous male sexual partner while concurrently using crystal methamphetamine (use of crystal methamphetamine a few hours prior to or during sex) in the past 3 months; (3) HIV-uninfected (verified serostatus at baseline via HIV antibody testing). Forty-four subjects screened, of whom 21 met initial entry criteria. Of these 21 participants, 2 tested positive for HIV and were triaged into care. A total of 19 participants enrolled; 16 returned and initiated treatment. These 16 HIV-uninfected MSM completed the Project IMPACT intervention (10 sessions, approximately 50 min each) and all three assessment visits. All study activities took place at The Fenway Institute, Fenway Health, in Boston, Massachusetts. The Fenway Institute Institutional Review Board approved the study and all procedures, and each participant completed an informed consent process.
Assessment visits
There were three major assessment points: baseline, acute postintervention (3 months postbaseline), and 3 month postintervention (6 months postbaseline). All postintervention assessment visits were completed by August 2010. The same study procedures and assessments were conducted at all three assessment visits. Each assessment visit lasted approximately 2 h and participants were compensated $50 per visit for their time and travel.
Behavioral activation therapy and risk reduction counseling (BA-RR) intervention
Baseline session: building rapport, orienting, rationale, and information gathering (1 session)
In this session, the aim was to build rapport and orient the participant to the research site, study, and interventionist. The interventionist provided an overview of, and the rationale for, both the risk reduction counseling and the BA aspects of the treatment, as well as gathered information about the participant's history and patterns of substance use (including proximal and distal triggers), substance use treatment, and mental health history.
Information-motivation-behavioral (IMB) skills change approach to sexual risk reduction (2 sessions)
The IMB model is constructed on an analysis and integration of theory and research in both health and social psychology literatures and has been applied to a wide array of wellness-promotion and health behaviors. 40,41 With respect to HIV prevention, IMB focuses parsimoniously on the set of informational, motivational, and behavioral skills that are conceptually and empirically associated with HIV prevention. In the present study, we utilize interventions consistent with the IMB model for the HIV risk reduction activities in which BA is integrated.
Early intervention modules focused directly on sexual risk reduction practices. The interventionist prompted the participant to discuss his sexual history, sexual risk limits, and elicited identification of barriers (e.g., motivation or skills) to maintaining sexual safety. This session also involved psychoeducation regarding the level of risk associated with specific sexual behaviors (information). The interventionist gathered and presented information in a way that promoted credibility and confidence in the treatment, which is associated with positive outcomes in psychological interventions. 42
The interventionist and participant also identified both triggers for, and motivations for, crystal use, and used motivational interviewing 43 to examine the impact of crystal methamphetamine episodes on the patient's life—including changes in mood and decreased feelings of enjoyment and mastery that are associated with crystal methamphetamine use and the relation between these constructs. Behavioral activation was introduced as a means to interrupt the cycle. As part of motivational interviewing, a discussion of pros and cons of changing (and not changing) was meant to assist the participant advance to a higher level of readiness to change.
Participants were prompted to identify goals for change and, with the interventionist's help, formulated an individualized behavioral skills plan. Change plans to increase behavioral skills included, for example: (1) initiating a discussion of HIV status for all partners; (2) increasing behavioral skills related to condom use; (3) working on reducing mixing crystal methamphetamine with sex; (4) identifying and modifying triggers for crystal methamphetamine use or sexual risk behavior; and (5) strategies for negotiating sexual safety even when crystal methamphetamine use occurs.
Behavioral activation integrated with risk reduction counseling (6 sessions)
As discussed above, the conceptual model postulated that, over time, crystal methamphetamine use combined with sex would significantly decreases an individual's ability to find pleasure from other previously enjoyed activities. This narrowing of an individual's behavioral repertoire, in turn, exacerbates crystal use. Thus, subsequent intervention content focused on integrating behavioral activation—that is, identifying patterns of behavioral avoidance, and relearning how to enjoy previously enjoyed activities without crystal methamphetamine use—with risk reduction counseling. Each session began with a behavioral assessment of the past week's crystal methamphetamine use and sexual risk taking behaviors, as well as an assessment of the participant's mood during that time. As needed, the interventionist reviewed the behavioral skills introduced in the first two sessions that focused on risk reduction.
Consistent throughout all modules is the use of a motivational interviewing style of intervention to identify discrepancies between goals and behavior, and to increase motivation for change. Elements of problem solving training 44 were included as part of the behavioral activation sessions, and involves teaching participants how to break down a complex task into manageable steps with the goal of reducing behavioral avoidance. Additional problem solving techniques include training in how to define a problem, generate and evaluate alternative solutions, and implement a potential change. This approach is commonly used for the treatment of depression 45 and has specific application to substance abuse. 46 For participants in this study, problem solving may have been particularly helpful in breaking the maladaptive and self-perpetuating cycle of crystal methamphetamine use in response to wanting to improve one's mood (e.g., participant withdrawal from crystal methamphetamine, feels depressed/unable to experience pleasure, participant uses more crystal to feel better, problem worsens, participant may engage in continued HIV risk behaviors). 46
Using the techniques of BA, the interventionist and participant identified nondrug use activities that were likely to increase a sense of pleasure or mastery, and discussed barriers to engagement in these activities. Activities may be those that the participant previously enjoyed or new activities that are identified with the use of a positive events checklist. Participants were encouraged to retry positive events that they previously enjoyed without using substances, and problem-solved with the interventionist ways to re-engage in such activities. The idea is for participants to broaden their repertoire of behavior and, over time, to begin to reexperience positive feelings as consequences of their nondrug use activities. Many participants required training in how to identify and label their emotional experiences.
Participants were introduced to an Activity Log, a mood and activity monitoring sheet, to track all behavior and, especially, to note the context and consequences of reengaging in pleasurable, nondrug use activities. Subsequent sessions are substantially focused on a review and analysis of the linkages between the participant's mood and behavior as tracked by the Activity Log. The interventionist monitored and highlighted the degree of engagement in pleasurable activities and helped the participant problem-solve this integration, as well as reviewed potential additional activities and barriers to ongoing behavioral activation. These techniques are based on activity scheduling, which is both a standard part of cognitive therapy for depression and the primary intervention technique in behavioral activation when applied to depression. 47 As much as possible, participants were encouraged to find regularly occurring activities including (but not limited to) social events, volunteering, and involvement in additional supportive activities.
Review and plan for relapse prevention (1 session)
A final session involved a review of previous sessions and skills acquired, and a focus on plans for relapse prevention regarding both crystal methamphetamine use, unprotected anal sex, and continued engagement in enjoyable life activities other than drug use. Required content included differentiating a lapse from a relapse, anticipating difficult or stressful situations that may be triggers for lapses, and encouraging ways to utilize skills learned to maintain gains. The focus of this session, generally, is to transition participants to be their own interventionist or to engage with ongoing support or psychotherapy to address lingering problems related to substance use, mood, or sexual risk.
Biologic testing for HIV
The FDA-approved OraQuick® ADVANCE ® HIV-1/2 Antibody Test (finger stick; OraSure Technologies, Bethlehem, PA) was used for HIV testing in the present study (sensitivity: 99.6% [98.5–99.9]; specificity: 100% [99.7–100]). Like conventional HIV enzyme immunoassays (EIAs), rapid HIV tests are screening tests that require confirmation if reactive (positive). All confirmatory test procedures were followed with participants whose test results were indeterminate. Onsite confirmatory testing by blood draw followed the HIV testing guidelines of Fenway Health.
Measures
Demographic characteristics
Demographic characteristics included age, race/ethnicity, education, employment, income, sexual orientation, and relationship status. Participants were queried about their lifetime history of sexually transmitted infections (STIs).
HIV sexual risk behavior
Participants were asked about the number of episodes of unprotected anal intercourse (UAI) in the past 3 months (continuous), including UAI in the context of using crystal methamphetamine, and with HIV serostatus unknown sexual partners. Participants were also asked to indicate their self-perceived risk for HIV infection on a 10-point scale, ranging from 0 (not at all at risk) to 10 (extremely at risk).
Substance use
A quantity-frequency index for crystal methamphetamine and other substances was used, to be sensitive to pre-/postintervention change. The NIDA-CTN Addiction Severity Index Lite (ASI-Lite) was administered, 48 a shortened version of the Addiction Severity Index (ASI). 49 Participants were asked to self-report the number of days they used crystal methamphetamine in the past 30 days. Additional questions assessed crystal methamphetamine use in the past 3 months, including the number of discrete crystal methamphetamine episodes.
The frequency of other substances used in the past 3 months in the context of sex (using a few hours prior to or during sex) was also queried, including poppers, non-prescribed erectile dysfunction drugs, marijuana, GHB, crack, cocaine, downers, painkillers, ecstasy, and alcohol. A summary score was created of the number of substances used during sex in the past 3 months by dichotomizing each substance used during sex in the past 3 months (yes/no) and summing across the binary variables, with possible values ranging from 0 to 10.
Depressive symptoms
Montgomery-Asberg Depression Rating Scale (MADRS) is a semistructured, clinician-rated interview designed to be used in patients to measure the degree of severity of depressive symptoms, and particularly as a sensitive measure of change in symptom severity. 50 The MADRS has a fixed scaling of seven points (from 0 to 6) and measures the severity of symptoms, including mood and sadness, tension, sleep, appetite, energy, concentration, suicidal ideation, and restlessness. The following mean scores correlated with global severity measures: 44 very severe; 31 severe; 25 moderate; 15 mild; 7 recovered. The Cronbach coefficient α for the MADRS in this current study was 0.82 (baseline), 0.86 (acute postintervention), and 0.91 (3 months postintervention).
Engagement in positive events
The Behavioral Activation Scale (BADS) was used, 51 a 25-item measure that specifically assesses the behaviors believed to be responsible for change (i.e., behaviors that should lead to increased contact with response contingent positive reinforcement) according to the behavioral activation treatment model. 52 –57 The scale measures four factors (Activation, Avoidance/Rumination, Work/School Impairment, and Social Impairment) with good factor structure, internal consistency, test–retest reliability, and construct and predictive validity. 51
Changes in information, motivation, and behavioral skills
Increases in HIV information, motivation, and behavioral skills were assessed. Each of these variables mirrors content of the intervention manual. These assessments are based on valid scales, 58 –60 but were adapted for use in the current study.
Information
There are 18 information items answered on a “True,” “False,” or “Don't Know” scale. A participant's score on the information scale consists of the total number of correct responses out of 18 (“Don't Know” will be coded as incorrect).
Motivation
Motivation to practice safer behavior was assessed as three separate dimensions: attitudes (10 items), norms (13 items), and behavioral intentions (4 items) to engage in HIV-preventive actions (total scale=27 items).
Behavioral skills
Behavioral skills for HIV prevention was assessed with 10 items that asked how “hard” or “easy” it was for patients to implement a variety of skills, including discussing sex and condom use with both primary and non-primary sexual partners, and acquiring and using condoms. Response options range from 1=“Very Hard to Do” to 5=“Very Easy to Do.”
Data analysis
SAS (version 9.2; SAS Institute Inc., Cary, NC) was used for all data analyses, with statistical significance determined at the α 0.05 level. Working with the data in multivariate form (1 participant per row; 16 rows total; person-level dataset), descriptive statistics were obtained for all variables (frequencies, means, standard deviations, ranges), and the presence of outliers was evaluated. Tests for normality were obtained for all continuous measures (e.g., scale scores) to ensure that all statistical assumptions were met for linear regression procedures (e.g., linearity, normality).
Because a longitudinal, repeated measures design was utilized to collect identical measures on the same individuals over three measurement occasions (baseline [time 0], acute postintervention [time 1], and 3 month postintervention [time 2]), all measures were positively correlated over each measurement occasion—violating the fundamental assumption of independence required for many standard regression techniques. 61,62 To increase efficiency and precision of estimates, and to adjust standard errors, restricted maximum likelihood (REML) estimation, a modified form of maximum likelihood (ML) estimation, was used to fit linear regression models. This procedure corrects for the asymptotic properties of ML which produce biased estimates in smaller sample sizes (i.e., ML typically underestimates). 61
The data were converted to univariate form (1 observation per row for every measurement occasion; 48 rows total; person-period dataset). 62 The MIXED procedure in SAS (PROC MIXED) was used to obtain REML estimates (METHOD=REML), and to account for correlated measurements (REPEATED=ID). An unstructured covariance was assumed (TYPE=UN), meaning that no explicit structure was assumed for the covariance among the repeated measures, other than that the homogeneity of covariance across individuals. This method of analysis of longitudinal data is robust, since the potential risks of bias due to misspecification of the models for the mean and covariance are minimal. These procedures were especially appropriate given the current study's balanced design, i.e., all individuals had the same number of repeated measurements obtained at a common set of occasions.
A series of linear regression models were fit to assess change over time for two sets of outcomes (see below). All modeled outcomes were continuous. Time was the primary predictor of interest in each fitted model (main effects). Baseline (time 0) was the specified referent in each fitted model.
Primary outcomes: HIV sexual risk in the past 3 months
Seven regression models were fit as follows: (1) Model 1: UAI episodes; (2) Model 2: UAI episodes with an HIV unknown status male partner; (3) Model 3: UAI episodes while using crystal methamphetamine; (4) Model 4: UAI episodes with an HIV unknown status male partner while using crystal methamphetamine; (5) Model 5: self-perceived HIV risk; (6) Model 6: self-perceived HIV risk while using crystal methamphetamine; (7) Model 7: IMB behavioral skills.
Secondary outcomes: Psychosocial factors
Seven additional regression models were estimated as follows: (1) Model 1: number of crystal methamphetamine episodes in the past 3 months; (2) Model 2: Number of days of crystal methamphetamine use in the past 30 days; (3) Model 3: Number of days experiencing drug-related problems in the past 30 days; (4) Model 4: Depressive symptom score (MADRS); (5) Model 5: Avoidance subscale of BADS; (6) Model 6: Work/School impairment subscale of BADS; (7) Model 7: Social impairment subscale of BADS; (8) Model 8: Number of substances used during sex in the past 3 months.
Results
Sample characteristics
Table 1 presents characteristics of the study sample (n=16). Participants ranged in age from 24 to 52, with a mean age of 40.0 (standard deviation [SD]=9.56). Overall, 37.50% were racial/ethnic minorities (18.75% black/African American, 6.25% Latino/Hispanic, 6.25% Asian/Native Hawaiian/Other Pacific Islander, and 12.50% American Indian/Alaskan Native). The majority of the sample (62.50%) reported having had an STI in their lifetime; 43.75% reported having had one STI, and 18.75% reported two or more STIs. Self-reported STIs were as follows: 37.50% gonorrhea, 12.50% syphilis, 12.50% chlamydia, 6.25% herpes, and 25.00% some other STI.
SD, standard deviation; STDs, sexually transmitted diseases; IDU, injection drug use.
Participants reported having been in drug treatment a mean of 3.63 (SD=7.56) times in their lifetimes. Participants reported using crystal methamphetamine in the past 3 months as follows: 87.50% smoked, 25.00% snorted, 25.00% injected, 18.75% rectally inserted. Nearly one third (31.25%) reported having traded sex in exchange for crystal methamphetamine in the past 3 months.
Primary outcomes: HIV sexual risk behavior in the past 3 months
Baseline
Participants reported a mean number of 5.93 (SD=4.50) UAI episodes in the past 3 months at baseline, 3.36 (SD=3.86) of which were with an HIV unknown status male sex partner. A mean of 4.43 (SD=4.16) UAI episodes were reported while using crystal methamphetamine in the past 3 months, 2.13 (SD=2.39) of which were with an HIV unknown status male partner. Participants perceived themselves to be at moderately high risk for HIV infection, with a mean score of 6.28 of 10 (SD=2.78), and self-perceived their risk to increase in the context of crystal methamphetamine use (mean=7.69; SD=2.85).
Postintervention
Table 2 presents the means (SDs) for the primary outcomes of HIV sexual risk at the baseline, acute postintervention, and 3-month postintervention assessments. Compared to baseline, all primary outcome variables decreased at the acute postintervention, and at the 3-month postintervention assessments—indicating reductions in HIV sexual risk behaviors following the completion of the BA-RR intervention.
UAI, unprotected anal intercourse.
Repeated measures analysis
Table 3 presents fitted linear models regressing HIV sexual risk behavior scores on time. Statistically significant reductions in sexual risk behaviors were observed across all primary outcome variables comparing baseline and postintervention assessments, and were maintained over time comparing baseline and 3 months postintervention.
Note on Model 4: There was not enough variability between postintervention and 3 month follow-up assessments to model; therefore the fitted model for number of UAI episodes using crystal meth with an HIV unknown serostatus partner only includes baseline and acute postintervention assessments.
CI, confidence interval; UAI, unprotected and intercourse.
As shown graphically in Fig. 1A, mean UAI episodes decreased significantly from baseline to acute post-intervention (β=−4.86; 95% CI=−7.48, −2.24; p=0.0015) and from baseline to 3 months postintervention (β=−5.07; 95% CI=−7.85, −2.29; p=0.0017) (Model 1: test of fixed effects χ2=16.59; df=2,13; p=0.0002). Similarly, mean UAI episodes with HIV unknown status male partner(s) evidenced statistically significant decreases from baseline to postintervention (β=−3.23; 95% CI=−5.45, −0.98; p=0.0083) and from baseline to 3 months postintervention (β=−2.79; 95% CI=−4.89, −0.68; p=0.0133; Model 2: test of fixed effects χ2=10.10; df=2,13; p=0.0064).
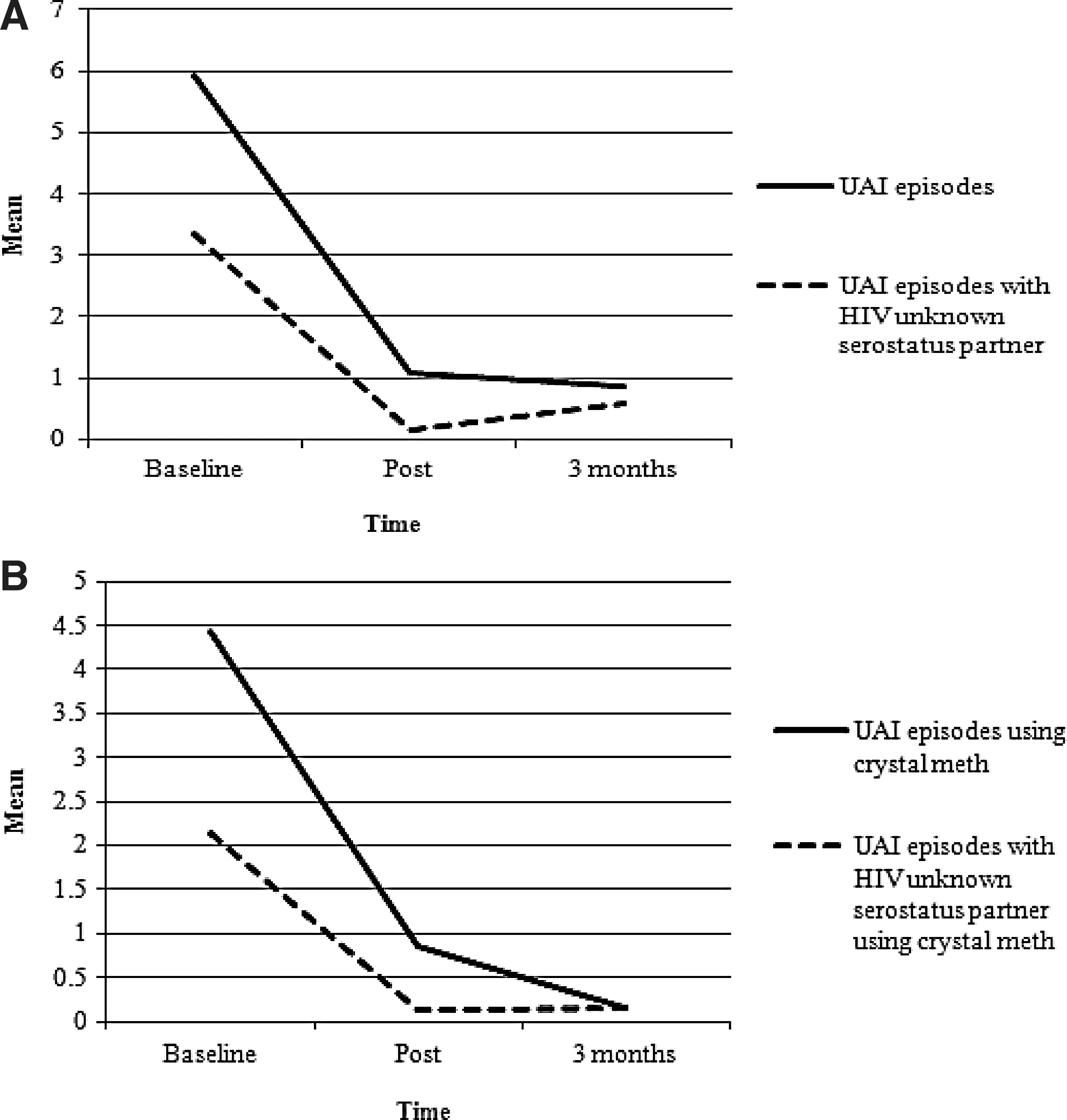
Graphical display of HIV sexual risk behavior (number of unprotected anal intercourse episodes in the past 3 months) at baseline, acute postintervention, and 3 months postintervention.
A similar pattern of risk reduction (Fig. 1B) was seen in UAI episodes while using crystal methamphetamine at acute postintervention (β=−3.57; 95% CI=−6.24, −0.90; p=0.0126) and 3 months post-intervention (β=−4.29; 95% CI=−6.74, −1.83; p=0.0023; Model 3: test of fixed effects χ2=17.45; df=2,13; p=0.0002), as well as UAI episodes with HIV unknown serostatus male partner(s) while using crystal methamphetamine from baseline to post-intervention (β=−2.00; 95% CI=−3.32, −0.68; p=0.0059) (Model 4: test of fixed effects χ2=10.50; df=1,14; p=0.0012).
Reductions in self-perceived HIV risk accompanied observed changes in sexual risk behaviors at acute postintervention (β=−2.19; 95% CI=−3.94, −0.43; p=0.0179) and 3 months postintervention (β=−2.25; 95% CI=−4.25, −0.25; p=0.0298; Model 5: test of fixed effects χ2=7.08; df=2,15; p=0.029). This pattern of change was also found for self-perceived HIV risk while using crystal methamphetamine (Model 6: test of fixed effects χ2=32.92; df=2,15; p<0.0001). Improvement in IMB behavioral skills were seen in the expected direction (higher scores indicating increases in IMB behavioral skills), but did not reach statistical significance (Model 7: test of fixed effects: χ2=3.43; df=2,15; p=0.18).
Secondary outcomes: Psychosocial factors
Baseline
Participants reported a mean number of 3.33 (SD=2.35) episodes of crystal methamphetamine use in the past 3 months. In the past 30 days, participants reported a mean number of 3.75 days (SD=6.91) of crystal methamphetamine use and 17.19 (SD=12.05) days on which they experienced drug-related problems related to their use of substances. Mean depression scores were in the clinically moderate range (mean 23.63; SD=8.49) at baseline. In addition to crystal methamphetamine use, participants reported using a mean number of 4.94 (SD=1.24) other substances during sex in the prior 3 months. Substances included 81.25% poppers, 62.50% non-prescribed erectile dysfunction drugs, 56.25% marijuana, 43.75% GHB, 43.75% crack, 31.25% cocaine, 18.75% downers, 12.50% painkillers, 6.25% ecstasy, and 37.50% alcohol.
Postintervention
Table 4 presents the mean (SD) for psychosocial factors (secondary outcomes) at baseline, acute postintervention, and 3 months postintervention. Compared to baseline, all psychosocial factors decreased at the acute post-intervention and 3 months postintervention assessments after completing the BA-RR intervention.
Crystal meth episode=“How many different episodes of crystal use did you have in the past 3 months?”
MADRS, Montgomery Asberg Depression Rating Scale; SD, standard deviation; BADS, Behavioral Activation for Depression Scale.
Repeated measures analysis
Table 5 provides results from fitted linear regression models regressing psychosocial factor scores on time. Statistically significant reductions in psychosocial factors were observed comparing baseline and postintervention assessments, and were maintained over time comparing baseline and 3 months postintervention. On average, there was a significant decrease over time in the number of crystal methamphetamine episodes in the past 3 months (Model 1: test of fixed effects χ2=22.43; df=2,15; p<0.0001); number of days of crystal methamphetamine use in the past 30 days (Model 2: test of fixed effects χ2=9.21; df=2,15; p=0.010); and number of days experiencing drug-related problems in the past 30 days (Model 3: test of fixed effects χ2=10.58; df=2,15; p=0.005).
Crystal meth episode=“How many different episodes of crystal use did you have in the past 3 months?”
Model 1, Model 2, Model 3, Model 4, Model 5, Model 6: n=48 observations.
CI, confidence interval; MADRS, Montgomery Asberg Depression Rating Scale; BADS, Behavioral Activation for Depression Scale.
In addition, compared to baseline, significant reductions in depression scores were seen at acute postintervention (β=−5.45; 95% CI=−10.67, −0.22; p=0.042) and 3 months post-intervention (β=−7.44; 95% CI=−13.04, −1.84; p=0.013; Model 4: test of fixed effects χ2=8.22; df=2,15; p=0.016). Improvements in behavioral activation subscales were seen in the expected direction, but did not reach statistical significance for avoidance (Model 5), work/school impairment (Model 6), or social impairment (Model 7). There was a significant decrease over time in the number of substances used during sex in the past 3 months (Model 8: test of fixed effects χ2=25.60; df=2,15; p<0.0001).
Discussion
This study provides good evidence of participant acceptance, ability to recruit, feasibility of treatment delivery, adaptation of the treatment manual, and significant improvement in primary and secondary outcomes. The focus of this intervention development study was to demonstrate the ability to conduct the intervention and examine whether it has the potential to impact study outcomes in a clinically relevant way. Although the primary focus was not on obtaining statistically significant results, in fact all of the primary and many of the secondary outcome measures showed improvements in the hypothesized direction. Moreover, statistically significant differences did emerge with respect to the main study outcomes: reductions in risky sexual behavior and crystal methamphetamine use (primary), and psychosocial factors (secondary), including depression and polysubstance use, over study follow-up.
There is a lack of intervention research that focuses on treating problematic crystal methamphetamine use among MSM at high risk for HIV infection. The mainstay of crystal methamphetamine treatment is behavioral modification, using interventions such as cognitive behavioral therapy (CBT) 63 –66 and contingency management (CM). 67 –71 To date, few studies have been successful at demonstrating the utility of CBT for the treatment of crystal methamphetamine abuse. 35,70,72,73 Moreover, CM has been shown to decrease stimulant use and increase both clinic attendance and medication adherence, 68,74 and individuals receiving contingency management have been shown to have a greater percentage of negative toxicology screens while on treatment compared with standard of care and CBT. 35,66,73,75 However, data from stimulant-abusing West Coast MSM who enter behavioral treatment (e.g., CM or CBT) for substance abuse suggests that, although reductions in both substance use and HIV-related sexual risk behaviors are seen almost immediately upon treatment entry, these effects diminish over time. 35,76,77 Additionally, CM may not be feasible in many settings. The current study adds to the literature in that data are not available for nonhospital or outpatient settings on the East Coast, and the use of behavioral activation as a treatment modality with this population is novel, and as a skills-based program in the current study shows promise for good maintenance of treatment effect.
At present, there are no medications approved for the treatment of crystal methamphetamine abuse or dependence. 78 Despite evidence that pharmacotherapies for crystal methamphetamine may be developed by altering the pharmacokinetics and pharmacodynamics of methamphetamine or its effects on the brain's appetitive systems, 79 there have been fewer than 10 published placebo-controlled double-blinded efficacy trials of potential methamphetamine pharmacotherapies (e.g., methylphenidate, modafinil, bupropion, etc., and studies are underway examining naltrexone showing preliminary evidence of good activity). 70,71,73,80 –84 Given that not all patients will want to take medications, and that adding behavioral interventions to medications could be valuable in promoting engagement and retention to treatments and improving outcomes, 79,82 investing in and refining new behavioral treatment approaches to methamphetamine abuse/dependence represents an important step towards intervention development for both crystal methamphetamine use and HIV sexual risk among MSM.
Crystal methamphetamine use has been linked with depression in the wake of cessation of use, with a loss of pleasure and interest in other activities accompanying periods of abstinence. 5,34,85 Notably, several studies suggest that pleasurable activities reported prior to the initiation of crystal methamphetamine use become much less enjoyable in the absence of sustained use, 5,86,87 which is consistent with our formative qualitative work. 5 Reports indicate that the crystal “high” becomes normalized for the user, and abstinence (previously the normal state) comes to be perceived by the user as a subnormal condition. 88 Within the first several days of ceasing crystal methamphetamine use, individuals report anhedonia, irritability, and poor concentration—symptoms consistent with depression. 86 There is also evidence that depressive symptoms may persist for many months following cessation of use, likely due to disruptions in the dopamine pathways in the brain. 87 The anhedonia reported by crystal methamphetamine users during periods of abstinence parallels the loss of interest in sex and other activities without crystal methamphetamine reported by many MSM users. 5,27 The fear of no longer being sexual has been identified as a major barrier to giving up crystal methamphetamine among MSM. 89 These data have informed our study conceptualization (empirically supported treatment for depression to facilitate crystal methamphetamine abstinence) in that individuals will be drawn to continued crystal methamphetamine use to alleviate depressed mood.
Effective treatments for crystal methamphetamine abuse and HIV risk reduction are needed in outpatient clinics and tertiary care centers that serve MSM. The reduction or cessation of substance use is the principal concern of hospital and other inpatient drug treatment programs. 90 However, many individuals receiving drug abuse treatment experience co-occurring problems that remain unaddressed in these settings, such as HIV sexual risk behaviors, that may complicate not only their recovery process but also have broad public health significance with respect to rates of infectious disease. 17 Moreover, at specialized settings or clinics serving MSM, a lack of effective treatment for crystal methamphetamine abuse and difficulties implementing traditional HIV prevention modalities among methamphetamine-using MSM remain significant barriers to addressing these concomitant health concerns of this population. Effective treatment for problematic crystal methamphetamine use, such as the intervention described here, delivered to HIV seronegative MSM in a specialized setting may represent an important component of a comprehensive HIV/STI control strategy for MSM. 35 The future of HIV-related behavioral interventions appear to include comprehensive programs that provide treatment for mental health problems along with the use of techniques proven to change health behaviors. 91
Although the study provides promising initial findings suggesting the feasibility, acceptability and the potential for an integrated behavioral program to impact sexual risk, substance use, and depression outcomes these findings are most appropriately interpreted in the context of the limitations of the study design. The current study used a small sample size, and did not use a randomized control condition. The small sample size also precludes testing of the hypothesized theoretical model underlying the significant changes that we observed. This would seem especially important given the lack of significant findings related to the behavioral activation subscales. However, this study represents an initial step towards developing and testing a potentially efficacious intervention for a high-risk group. An additional limitation is that the study enrolled only HIV-uninfected MSM. The justification for including only HIV-uninfected MSM was twofold. First, the research literature documents that crystal methamphetamine use increases sexual risk taking in this population. Second, through the clinical experience of the study team, which guided the development of the current intervention, it was determined that an intervention for HIV-infected crystal methamphetamine using MSM would need to incorporate additional components regarding self-care, initiating and maintaining active involvement in medical care, medication adherence, etc. The current intervention did not include such components. Additional research and intervention development is needed to address crystal methamphetamine use among HIV-infected MSM generally, and to test in a randomized fashion this current intervention, specifically.
There are few interventions that target sexual risk taking in the population of MSM who abuse crystal methamphetamine, and no interventions to our knowledge that have been developed and tested integrating risk reduction counseling with BA. Existing empirical data, as well as our ongoing qualitative and clinical work, suggest that continued crystal methamphetamine use may be exacerbated or maintained, in part, as a result of a symptom of anhedonia—loss of interest in previously pleasurable activities. An intervention that integrates state-of-the-art approaches to sexual risk reduction (i.e., based on the IMB model), with evidence-based treatments such as behavioral activation, may be an effective approach to reducing this complex, mutually interactive, and treatment-refractory set of problems.
Futhermore, BA is a principle-based treatment that is intended to be delivered by therapists with a wide range of educational backgrounds—allowing for delivery of this intervention across multiple settings. There is no reason a case manager or other bachelors-level interventionist could not implement this treatment. It is possible that peer counselors could be interventionists on a BA protocol although we do not know of any trials that have used lay therapists in this way. BA-RR appears to be an acceptable and feasible intervention for MSM with problematic crystal methamphetamine use who are at high risk for HIV-infection. This preliminary evidence suggests that BA-RR may well have the potential to effect significant reductions in both sexual risk for HIV and crystal methamphetamine use for those MSM who continue to struggle with both problems, and is worthy of efficacy testing in a future randomized controlled trial, with cost effectiveness examined.
Footnotes
Acknowledgments
This project was supported by grant number R03DA023393 (PI: Mimiaga) from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health. These findings were partially presented at the Society of Behavioral Medicine 2010 Annual Meeting, Seattle, Washington, and at the 2010 International AIDS Society Meeting, Vienna, Austria.
Author Disclosure Statement
No competing financial interests exist.