
Abstract
The once daily, single-tablet regimen (STR) combining rilpivirine (RPV), emtricitabine (FTC), and tenofovir disoproxil fumarate (TDF) provides a simplified treatment option for antiretroviral therapy (ART)-naïve patients with baseline HIV-1 RNA (BLVL) of ≤100,000 copies/mL. The aim of this analysis is to compare long-term efficacy, safety, and tolerability of RPV+FTC/TDF vs. efavirenz (EFV)+FTC/TDF as individual components in subjects with BLVL ≤100,000 copies/mL. Week 96 efficacy and safety data from subjects with BLVL ≤100,000 copies/mL, who received daily RPV 25 mg or EFV 600 mg with FTC/TDF in the phase 3, randomized, double-blind, double-dummy, active-controlled, registrational trials ECHO and THRIVE, were analyzed. Virologic response was evaluated by intent-to-treat, time to loss of virological response (ITT-TLOVR), and Snapshot algorithms. Through Week 96, RPV+FTC/TDF demonstrated non-inferior efficacy to EFV+FTC/TDF (84% vs. 81%, respectively; ITT-TLOVR) in 543 subjects with BLVL ≤100,000 copies/mL, and overall rates of virologic failure (VF) were 5.9% vs. 2.4%, respectively. Resistance development was lower in Year 2 than Year 1. Subjects in both arms with suboptimal adherence (≤95%) had lower virologic responses (63% vs. 62%, respectively). Treatment with RPV+FTC/TDF was associated with significantly fewer treatment-related adverse events (AEs), grade 2–4 AEs, neurological and psychiatric AEs (including dizziness and abnormal dreams/nightmares), and rash. Additionally, grade 2–4 treatment-emergent laboratory abnormalities and grade 1–3 lipid abnormalities were significantly less common with RPV+FTC/TDF than EFV+FTC/TDF. RPV+FTC/TDF demonstrated non-inferior efficacy to EFV+FTC/TDF in ART-naïve subjects with BLVL ≤100,000 copies/mL and was associated with a higher rate of VF but a more favorable safety and tolerability profile through Week 96.
Introduction
F
In light of the indication for RPV, both as the individual agent and as the STR, it is considered appropriate to assess the efficacy, safety, and tolerability of RPV+FTC/TDF (the components of the STR) in the subset of subjects with BLVL ≤100,000 copies/mL from the pooled ECHO and THRIVE trials. This publication extends through the final analysis point at Week 96 the pooled ECHO and THRIVE analysis of RPV versus EFV both with FTC/TDF in subjects with BLVL ≤100,000 copies/mL. 7
Materials and Methods
ECHO and THRIVE were two phase 3, double-blind, double-dummy, active-controlled, randomized, multicenter trials designed to assess the efficacy, safety, and tolerability of RPV 25 mg versus EFV 600 mg taken once daily with an nucleoside/nucleotide reverse transcriptase inhibitor [N(t)RTI] background regimen for 96 weeks. In the THRIVE study, investigators could choose from three background N(t)RTI regimens [FTC/TDF, zidovudine/lamivudine (AZT/3TC), or abacavir/lamivudine (ABC/3TC)], while in the ECHO study all individuals received FTC/TDF. Subjects enrolled in both studies were HIV-1 infected ART-naïve adults with any CD4 cell count, plasma HIV-1 RNA ≥5000 copies/mL, and demonstrated viral sensitivity to the background N(t)RTIs. Subjects were excluded if they had known NNRTI resistance associated mutations (RAMs), 8 active clinically significant disease, HIV-2 infection, renal impairment [estimated glomerular filtration rate (eGFR) <50 mL/min], or were pregnant or breastfeeding. Rilpivirine (or matching placebo) was recommended to be taken with food, whereas EFV (or matching placebo) was recommended to be taken on an empty stomach at bedtime. Further detail on the individual study designs, timing of assessments, and methods have been previously published. 9,10,11
For both the ECHO and THRIVE studies, the primary endpoint was Week 48 non-inferiority of RPV compared to EFV using the 95% confidence interval (CI) of the difference in virologic response between treatment arms and a pre-specified non-inferiority margin of 12%. Virologic response is defined as HIV-1 RNA <50 copies/mL according to the FDA's time to loss of virologic response (TLOVR) algorithm. Virologic response using the FDA's Snapshot algorithm was also assessed. Virologic failure was defined as HIV-1 RNA >50 copies/mL at Week 48, Week 96, early discontinuation, or last visit on study drug. Adverse events (AEs) were coded using MedDRA (version 11.0), and severity of AEs was evaluated according to the Division of AIDS grading scale. 12 Using all available data, the incidence of treatment-related AEs, AEs leading to discontinuation, and select EFV-related neurologic and psychiatric AEs were compared between the RPV+FTC/TDF and EFV+FTC/TDF groups within the BLVL ≤100,000 copies/mL subset. Adherence data were self-reported using an abbreviated version of the validated Medication Adherence Self-Report Inventory (MASRI) questionnaire in which subjects self-report their adherence over the past 30 days by means of a horizontal visual analogue scale ranging from 0% to 100%. Dual energy x-ray absorptiometry (DEXA) was performed in sub-studies to assess any changes in bone mineral density (BMD) and limb fat.
Results
Of the 1368 subjects in the ECHO and THRIVE studies, 80% received RPV or EFV with FTC/TDF. Five hundred and forty-three subjects with BLVL ≤100,000 copies/mL were included in this analysis: 288 subjects treated with RPV+FTC/TDF and 255 subjects treated with EFV+FTC/TDF. Baseline demographics and disease characteristics were similar between the RPV+FTC/TDF and EFV+FTC/TDF groups (Table 1). About three quarters of the 543 subjects were males, 60% RPV+FTC/TDF and 59% EFV+FTC/TDF were Whites, 27% and 24% Blacks, 10% and 15% Asian, 22% and 27% were Hispanic/Latino ethnicity, respectively. The two arms had a similar median age, median duration of HIV infection, median CD4 count, and median baseline viral load of 4.5 log10 copies/mL.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; RPV, rilpivirine.
At Week 96, RPV+FTC/TDF demonstrated non-inferior efficacy to EFV+FTC/TDF with 84% and 81% of subjects achieving HIV-1 RNA <50 copies/mL utilizing the primary endpoint ITT-TLOVR analysis. (Table 2, Fig. 1). The difference in response rates between RPV+FTC/TDF and EFV+FTC/TDF was +2.9% with a 95% confidence interval of −3.6%, +9.3% (Table 2). The results by Snapshot analysis were similar at 83% and 80%. Mean increases from baseline to Week 96 in CD4 count were also similar (+221 and +211 cells/mm3, respectively). Overall VF rates, as defined in the ITT-TLOVR analysis, were low but higher with RPV+FTC/TDF [5.9% (17/288)] compared to EFV+FTC/TDF [2.4% (6/255)] through Week 96 (Table 2).
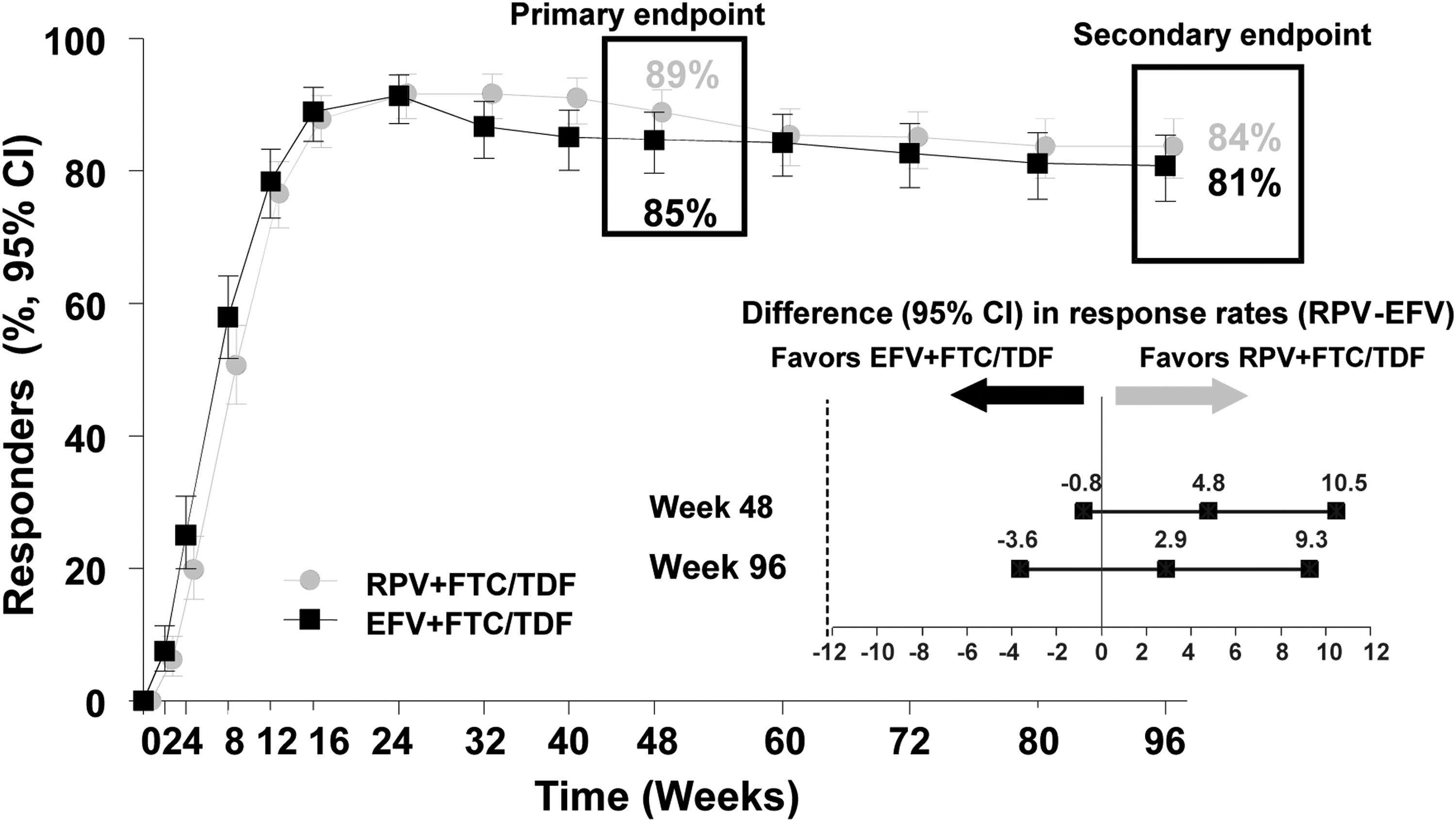
Virologic response (HIV-1 RNA <50 copies/mL) over time through week 96 (ITT-TLOVR analysis). CI, confidence interval; EFV, efavirenz; RPV, rilpivirine.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; RPV, rilpivirine; CI, confidence interval; TLOVR, time to loss of virologic response.
Plasma HIV-1 RNA was determined using a Roche Amplicor v1.5 viral load assay.
Virologic failure for TLOVR was defined as (1) confirmed two consecutive virologic response viral load (VL) <50 copies/mL before Week 96 and confirmed two consecutive rebound of HIV-1 RNA ≥50 copies/mL at or before Week 96, or (2) no confirmed response (VL <50 copies/mL) before Week 96.
Snapshot analysis based upon the last HIV-1 RNA value in the Week 96 visit window (90–103 weeks) was performed.
Virologic failure for Snapshot was defined as (1) last on-treatment HIV-1 RNA ≥50 copies/mL in the Week 96 analysis window, or (2) no on-treatment HIV-1 RNA data in the Week 96 analysis window because subjects discontinued study drug prior to or in the Week 96 window either due to lack of efficacy or due to reasons other than adverse event, death, and lack of efficacy and have the last on-treatment HIV-1 RNA>50 copies/mL.
Through Week 96, a similar proportions of subjects on RPV+FTC/TDF (85%) and EFV+FTC/TDF (81%) had adherence levels>95% using the ITT analysis set. Optimal study drug adherence (>95%; patient-reported using the visual analog scale) was associated with a Week 96 virologic response of 87% in both treatment groups and similar rates of VFs [3.7% (9/245) for RPV+FTC/TDF and 2.9% (6/207) for EFV+FTC/TDF]. In those subjects with suboptimal adherence (≤95%), lower virologic responses of 63% and 62% were seen in the RPV+FTC/TDF and EFV+FTC/TDF treatment arms, respectively, with VF occurring in 6/32 (19%) and 0/29 (0%) subjects. At Week 96, efficacy was comparable in subjects with baseline CD4 values of <200 or ≥200 cells/mm3 (ranging between 80% to 84%) (Table 3). VF rates (HIV-1 RNA ≥50 copies/mL) by baseline CD4 <200 cells/mm3 were 7.7% in subjects on RPV+FTC/TDF and 6.7% in subjects on EFV+FTC/TDF, and were 5.4% and 1.4% by baseline CD4 ≥200 cells/mm3, respectively.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; RPV, rilpivirine; TLOVR, time to loss of virologic response.
Plasma HIV-1 RNA was determined using a Roche Amplicor V1.5 viral load assay.
Virologic failure for TLOVR was defined as (1) confirmed two consecutive virologic response of viral load (VL) <50 copies/mL before Week 96 and confirmed two consecutive rebound of VL ≥50 copies/mL at or before Week 96, or (2) no confirmed response (VL <50 copies/mL) before Week 96.
The resistance analysis population consisted of 8.0% (23 of 288) of RPV+FTC/TDF subjects and 4.7% (12 of 255) of EFV+FTC/TDF subjects. Most subjects were analyzed for emergent HIV resistance during the first 48 weeks with an additional five subjects (2%) in both treatment groups during Week 48 through 96 (Table 4). Genotypic data was available for isolates from 22 subjects in the RPV+FTC/TDF group and 10 subjects in the EFV+FTC/TDF group. The proportions of isolates with any treatment-emergent NNRTI RAM 8 were low for both treatment groups (3.5% and 1.2%, respectively), with E138K (1.4%) and K103N (1.2%) reported as the most frequently occurring NNRTI RAMs for RPV+FTC/TDF and EFV+FTC/TDF, respectively. Nine subjects taking RPV+FTC/TDF (3.1%) developed N(t)RTI RAMs in their HIV, as defined by the International AIDS Society (IAS), 13 and none did on EFV+FTC/TDF. The most frequently reported N(t)RTI RAM with RPV+FTC/TDF was M184I (2.8%) followed by M184V (0.7%). The K65R mutation, associated with TDF resistance, was not detected in either treatment group.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; NNRTI, non-nucleoside reverse transcriptase inhibitor; N(t)RTI, nucleoside/nucleotide reverse transcriptase inhibitor; RAM, resistance-associated mutation; RPV, rilpivirine.
Virologic failure in the resistance analysis was defined as (1) achieved two consecutive VL <50 copies/mL and then two consecutive VL ≥50 copies/mL or last visit VL ≥50 copies/mL, or (2) never achieved two consecutive VL <50 c/mL and increase in viral load ≥0.5 log10 copies/mL above the nadir). For individuals with confirmed virological failure, viral genotypic and phenotypic determinations were performed using VircoTYPE and Antivirogram assays (Janssen Diagnostics BVBA, Beerse, Belgium).
Post-dose genotypic data was obtained from the first available genotype after failure.
At least one emergent NNRTI RAM7 or N(t)RTI RAM.12
The K65R mutation was not detected in either treatment group.
One subject with a mixture of M184V/I was counted as having M184V and M184I.
Overall, RPV+FTC/TDF demonstrated a more favorable safety profile (Tables 5 and 6) and was better tolerated than EFV+FTC/TDF with numerical lower rates of discontinuations due to AEs 2.8% compared to 4.3%. The proportions of subjects experiencing any treatment-related AEs or treatment-related grade 2–4 AEs were lower in the RPV+FTC/TDF group compared to the EFV+FTC/TDF group (47% vs. 62% and 17% vs. 30%, respectively; both p<0.001). A smaller proportion of subjects on RPV+FTC/TDF compared to EVF+FTC/TDF experienced at least one treatment-related neurological and psychiatric AE of interest (19% vs. 38%; p<0.001 and 16% vs. 25%; p=0.018, respectively). These included a smaller proportion of subjects in the RPV+FTC/TDF group, compared to the EFV+FTC/TDF group, who experienced dizziness (10% vs. 28%, respectively; p<0.001), abnormal dreams/nightmares (7.6% vs. 14%, respectively; p=0.025), and rash (2.1% vs. 10.6%, respectively; all p<0.001). The majority of neurological and psychiatric AEs were grade 1 or 2 in severity.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; RPV, rilpivirine.
p Values are based on the Fisher exact test.
Includes preferred terms: depressed mood, depression, dysphoria, major depression, mood altered, negative thoughts, suicidal ideation, suicide attempts.
EFV, efavirenz; FTC/TDF, emtricitabine/tenofovir disoproxil fumarate; RPV, rilpivirine; LDL, low density lipoprotein.
Only those subjects with post-baseline measurements are included.
p Values are based upon a Fisher exact test.
There is no grade 4 for total cholesterol and LDL in the DAIDS grading scale.
For LDL cholesterol, only 248 subjects on EFV+FTC/TDF had post-baseline measurements.
Overall, through Week 96 a smaller proportion of subjects experienced grade 3–4 treatment-emergent laboratory abnormalities in the RPV+FTC/TDF group compared to the EFV+FTC/TDF group (11% vs. 21%, p=0.002) (Table 6). Grade 2–4 alanine aminotransferase (ALT) and aspartate aminotransferase (AST) abnormalities occurred less often in the RPV+FTC/TDF group compared to the EFV+FTC/TDF group, and was significant for ALT (6.6% vs. 12.9%, p=0.018). While grade 2–4 hyperbilirubinemia occurred in 4.2% of RPV+FTC/TDF subjects, it did not occur in the EFV+FTC/TDF group, p=0.001. Subjects receiving RPV+FTC/TDF experienced significant less grade 2–3 elevations in total cholesterol (TC; 7% vs. 22%, p<0.001, respectively) and low density lipoprotein cholesterol (LDL-C; 9% vs. 19%, p=0.001, respectively) compared with subjects receiving EFV+FTC/TDF over 96 weeks (Table 6). Fewer RPV+FTC/TDF subjects reported grade 1 total cholesterol (23.0% vs. 35.3%) compared to EFV/FTC/TDF, similar observation were seen with LDL-C (19.9% vs. 32.7%). Median values of TC, LDL-C, and triglycerides (TG), all decreased with RPV+FTC/TDF, while these parameters increased with EFV+FTC/TDF (all p<0.001) (Fig. 2). High density lipoprotein cholesterol (HDL-C) increased more with EFV+FTC/TDF compared to RPV+FTC/TDF (median values of 8.9 vs. 1.9 mg/dL, p<0.001). There was no difference between treatment groups in median TC: HDL-C ratio with a ratio of 3.5 at Week 96 in both treatment arms. Fewer subjects on RPV+FTC/TDF compared to EFV+FTC/TDF required lipid-lowering medications during the 96-week course of these studies (2.1% vs. 6.3%, p=0.016).
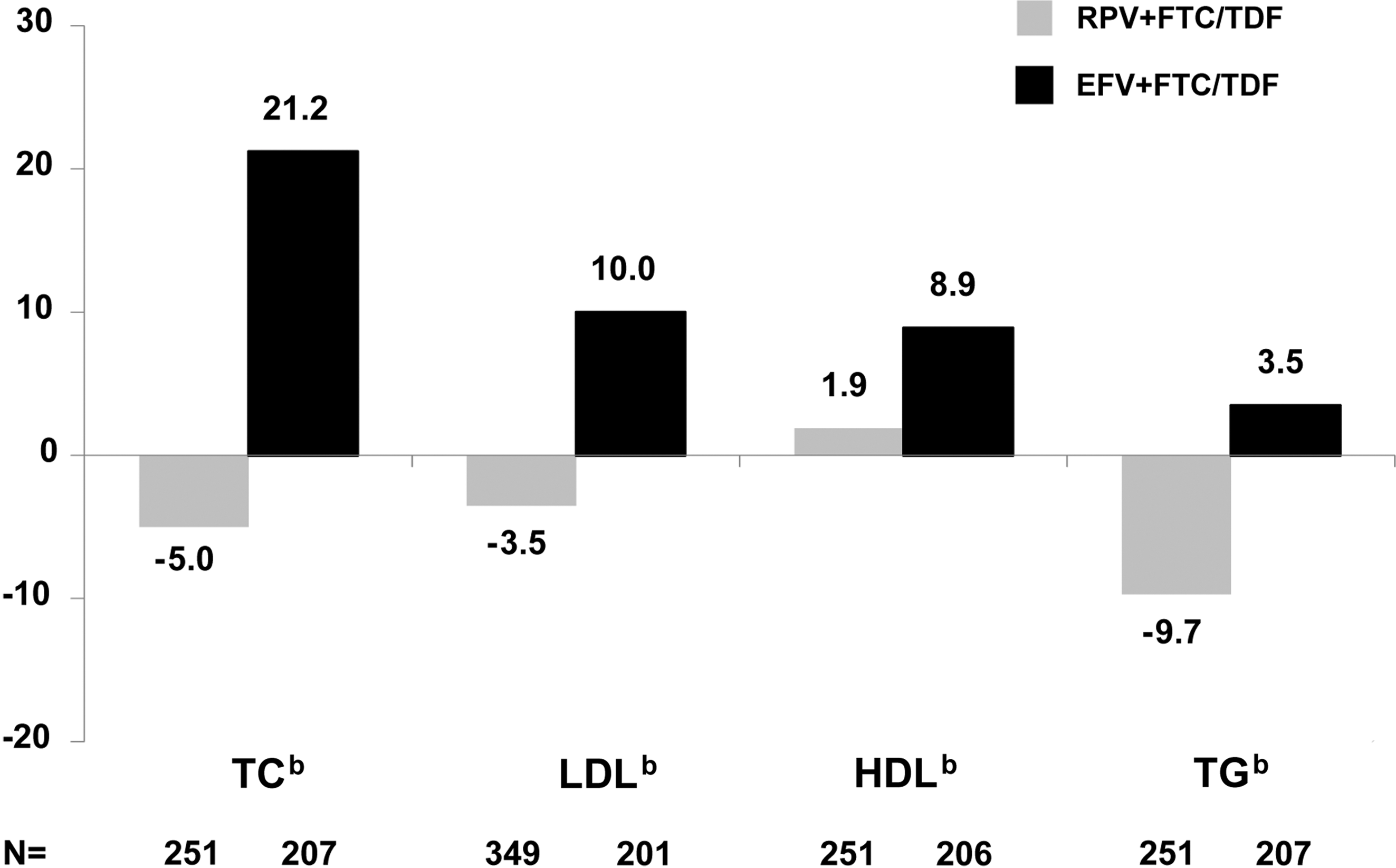
Mean fasting lipid changes from baseline to 96 weeks.a EFV, efavirenz; HDL, high density lipoprotein; LDL, low density lipoprotein; RPV, rilpivirine; TC, total cholesterol; TG, triglycerides. aExcludes subjects who received lipid lowering medications: RPV 6/288 subjects (2.1%) and EFV 16/255 subjects (6.3%). b p<0.001 for all comparisons (RPV vs. EFV) using the Wilcoxon rank-sum test.
Median serum creatinine changes from baseline to Week 96 were small for both treatment groups (RPV+FTC/TDF 0.10 mg/dL and EFV+FTC/TDF 0.03 mg/dL), but higher for the RPV group (p<0.001). Most serum creatinine changes were grade 1 elevations (RPV+FTC/TDF 6.3% and EFV+FTC/TDF 1.2%) and grade 2–4 elevations occurred in ≤1% of subjects in both treatment groups. The median eGFR at Week 96 remained in the normal range. There were no significant differences between treatment groups in changes from baseline to Week 96 in bone mineral density and limb fat. The median changes in bone mineral density were −0.015 grams/cm2 for RPV+FTC/TDF arm and −0.014 grams/cm2 for EFV+FTC/TDF arm. The median change from baseline to Week 96 in limb fat were +501 grams for RPV+FTC/TDF arm and +578 grams for EFV+FTC/TDF arm.
Discussion
In subjects with BL VL ≤100,000 copies/mL, RPV+FTC/TDF demonstrated non-inferior efficacy to EFV+FTC/TDF that was sustained over 96 weeks (84% vs. 81%, respectively; ITT TLOVR). These results are consistent with the analysis at Week 48 where virologic response rates were 89% versus 85% (Fig. 1). Higher levels of adherence were associated with a better virologic response in both treatment groups. Virologic responses were similar regardless of baseline CD4 count (≥200 or <200 cells/mm3) in subjects on RPV+FTC/TDF, though there was a small number of subjects with baseline CD4 count <200 cells/mm3.
The double-dummy design of the ECHO and THRIVE studies required subjects to take three pills given 2–3 times a day with differing meal requirements, which may have hampered study drug adherence. With the current availability of the STR formulation of the study drugs, the findings from the optimal adherence group (>95%) may be of particular interest, given the easier adherence requirements with a STR. Through Week 96, RPV+FTC/TDF subjects with optimal drug adherence demonstrated sustained, high virologic response (87%) with low VF rates (<4%).
Virologic outcomes may be impacted by the use of an STR, due to reduced pill count and decreased risk of selective adherence compared to individual antiretroviral components. 14 –17 The ongoing randomized, multicenter, international, open-label, phase 3b, 96-week, STaR study of 786 ART-naïve subjects evaluated the efficacy, safety, and tolerability of the two STRs [RPV/FTC/TDF (Complera®) and EFV/FTC/TDF (Atripla®) (EUDRACT ID 2010-024007-27, Clinical trials.gov: NCT01309243)]. 18 At Week 48 in the BLVL ≤100,000 copies/mL, the RPV/FTC/TDF STR compared to EFV/FTC/TDF STR showed non-inferiority and a significantly higher virologic response rate [89% vs 82%, 95% CI: +7.2% (+1.1%, +13.4%)] based on the Snapshot analysis. Through Week 48, the VF rates were low and similar; 5% for RPV/FTC/TDF and RPV+FTC/TDF and 3% for EFV/FTC/TDF and EFV+FTC/TDF in the STaR and ECHO/THRIVE studies, respectively. It should be noted that differences in study designs (i.e., open-label vs. double-dummy, double-blind), baseline characteristics (i.e., CD4), or other factors (i.e., study drug adherence, pharmacokinetics, adherence to RPV food requirement) may be contributing to the differences in outcomes observed in these studies of the individual components and STR for RPV, FTC, and TDF.
At Week 96 VF rates were low overall, but higher in the RPV+FTC/TDF group (5.9 %) compared to the EFV+FTC/TDF group (2.4%). More subjects with VF in the RPV+FTC/TDF group than in the EFV+FTC/TDF group had emergent NNRTI and/or N(t)RTI resistance substitutions in their HIV (3.5% vs.1.2%). The signature mutations for RPV (E138K) and FTC (M184I/V) were the most frequently occurring RAMs in the RPV+FTC/TDF group with no K65R emerging on treatment. For EFV+FTC/TDF the most frequent RAM was K103N with no M184I/V or K65R detected. These overall rates of resistance were comparable to those of other recent clinical trials in treatment naïve patients. 19,20
Overall, RPV+FTC/TDF demonstrated a more favorable safety and tolerability profile than EFV+FTC/TDF based on a lower rate of discontinuation due to AEs, as well as lower rates of moderate to severe treatment-related AEs, EFV-related neurologic and psychiatric AEs, and laboratory abnormalities. RPV+FTC/TDF provides a treatment option for patients that prefer to minimize the potential development of EFV-related AEs, such as dizziness, abnormal dreams/nightmares, and rash. The RPV+FTC/TDF laboratory abnormality profile is differentiated from EFV+FTC/TDF in that it has less impact on lipid parameters and alanine aminotransferase with greater changes in serum creatinine and bilirubin. RPV+FTC/TDF improved TC, LDL-C, and TG values and EFV+FTC/TDF improved HDL-C values. These lipid changes occurred early in therapy and were sustained through Week 96. The rate of grade 2–4 alanine aminotransferase with RPV+FTV/TDF was half that observed with EFV+FTC/TDF (6.6% vs. 12.9%). RPV inhibits a renal tubular secretion transporter of creatinine, and results in small serum creatinine elevations by Week 4 that plateau thereafter, consistent with the inhibition of tubular secretion of creatinine (S.K. Chuck, personal communication). This is supported by a previous publication on THRIVE data showing RPV treatment does not result in a decrease in cystatin C clearance, a surrogate marker of glomerular filtration rate. 10 No subjects in either treatment group discontinued the study due to renal AEs. The rate of grade 2–4 hyperbilirubinemia was higher with RPV+FTC/TDF (4.2% vs. 0% with EFV+FTC/TDF), but there were no reports of scleral icterus or jaundice.
A limitation of subset analyses is that the smaller sample size may limit generalization of the results. However, pooling the subjects from these two trials allowed the present analysis to include 543 subjects, which gave sufficient power to provide statistical analysis. The ECHO and THRIVE trials were stratified by BLVL with a pre-planned sub-analysis. The THRIVE trial was also stratified by N(t)RTI therapy with a pre-planned sub-analyses for this stratification. The current ad-hoc analysis combined the FTC/TDF subjects with VL <100,000 copies/mL from the two studies. In conclusion, ART-naïve subjects with BLVL ≤100,000 copies/mL who received the components of the STR (RPV+FTC/TDF) achieved a sustained virologic response through 96 weeks with an improved safety and tolerability profile and numerically higher rate of virologic failure compared to EFV plus FTC/TDF. The availability of RPV+FTC/TDF as a STR further enhances the choice of initial ART in patients with BLVL ≤100,000 copies/mL.
Footnotes
Acknowledgments
We thank the patients and their families for their participation and support during the ECHO and THRIVE studies. We acknowledge William Garner and Mike Tran (from Gilead Sciences Inc.) for statistical analysis and graphics contributions.
Funding: The ECHO and THRIVE studies were sponsored by Tibotec Pharmaceuticals (now Janssen R&D, LLC). This publication was supported by Gilead Sciences, Inc. Editorial services for this publication were provided by Sage Scientific Writing, LLC (Durham, NC), whose managing members are former employees of Gilead Sciences, Inc.
Author Disclosure Statement
The Janssen authors, (Drs. Lawurence Rimsky, Marita Stevens, and Simon Vanveggel) are full time employees of Janssen R&D, LLC or Janssen Infectious Diseases BVBA (Titusville, United States and Beerse, Belgium), and the Gilead Sciences authors (Drs. Matthew Bosse, David Thorpe, Kirsten White, Lijie Zhong, Jennifer DeMorin, and Susan Chuck) are full time employees of Gilead Sciences, Inc. or Europe Limited (Foster City, United States and Stockley Park, United Kingdom). Dr. Georg Behrens has received financial support (grants, speaker/advisor honoraria, travel) from AbbVie, Boehringer-Ingelheim, Bristol Myers Squibb, Gilead Sciences, GlaxoSmithKline, Merck, ViiV Healthcare, Teratechnology and Janssen Therapeutics. Dr. Bart Rijnders has received financial support (grants, speaker/advisor honoraria, travel) from Boehringer-Ingelheim, Bristol Myers Squibb, Gilead Sciences, GlaxoSmithKline, Janssen Therapeutics, and MSD. Dr. Mark Nelson has received honoraria for lectures and advisory boards and has received research support from Gilead Sciences and Janssen Therapeutics. Dr. Chloe Orkin has received financial support (grants, speaker/advisor honoraria, travel) from Abbott, Boehringer-Ingelheim, Bristol Myers Squibb, Gilead Sciences, GlaxoSmithKline, Janssen Therapeutics, Merck, and ViiV Healthcare. Dr. Anthony Mills has received honoraria for speaker lectures, advisory boards and research support from Gilead Sciences. Dr. Richard Elion has received financial support (research, speakers, consulting) from AbbVie, Boehringer-Ingelheim, Gilead Sciences, Janssen Therapeutics, Merck, and ViiV. Dr. Calvin Cohen has received honoraria for advisory boards from Bristol-Myers Squibb, Gilead Sciences, Janssen Therapeutics, Merck, Tobira, and ViiV. Dr. Cohen has received research support from Bristol-Myers Squibb, Gilead Sciences, Janssen Therapeutics, and Merck.