
Abstract
Limited data are available regarding adults age ≥50 at initial HIV diagnosis. Improved understanding of this group is critical in designing interventions to facilitate earlier diagnosis and linkage to HIV care. We characterize individuals newly diagnosed with HIV, particularly those ≥50 years old, and examine the relationship between age and late diagnosis defined as concurrent HIV and AIDS diagnoses. This is a retrospective study of individuals newly diagnosed with HIV from 2006–2011 at an academic medical center in New York City. Multivariable logistic regression was performed to evaluate the effect of age, gender, race/ethnicity, risk factor, and prior medical visits on late diagnosis. Adults age ≥50 comprised 21.3% of all newly diagnosed individuals. Among these older adults, 70.0% were diagnosed as inpatients and 68.9% concurrent with AIDS, compared to 41.7% and 38.9% of younger adults, respectively. On adjusted analyses, age ≥50 (OR 3.13, 95% CI 1.63, 5.98) and injection drug use (OR 4.4, 95% CI 1.31, 14.75) were positively associated with late diagnosis, whereas female gender was negatively associated with late diagnosis (OR 0.52, 95% CI 0.28, 0.98). Our data suggest that HIV testing efforts targeting older adults are essential to address the unmet needs of this population, including implementation of HIV screening guidelines in primary care settings.
Introduction
H
One critical consideration is whether older adults diagnosed with HIV are being identified later in the course of their disease than their younger counterparts, and whether this has adverse consequences in terms of treatment response, disease outcomes, and mortality. Studies have already demonstrated that late diagnosis of HIV leads to initiation of antiretroviral therapy (ART) at a more advanced stage of disease, resulting in longer time to, and often incomplete, CD4 cell count restoration. 15 These trends are exacerbated in older individuals in whom immunologic response to ART is impaired, and older age has been shown to negatively impact CD4 cell count increases. 15,16 A likely reason for this phenomenon is that HIV infection enhances the negative effect of advanced age on T-cells, and thereby counteracts the benefits of ART in this group. 17,18 As such, older adults may be particularly vulnerable to the detrimental sequelae of late HIV diagnosis, and data from the Centers for Disease Control and Prevention (CDC) reveal that the proportion of individuals who progress to AIDS within 12 months of their initial HIV diagnosis is considerably higher among adults age 50 and older. 11
An association between increased age and late diagnosis has been demonstrated in some studies 19 –24 but not others, 25 –27 suggesting that there is much to be learned about newly diagnosed HIV-infected older adults. Further, the racial and ethnic disparity in HIV diagnoses in the United States is even more extreme among adults age 50 and older than in younger adults. 28 We therefore aim to examine the role of age in timely diagnosis and characterize the demographic and clinical characteristics of individuals who were newly diagnosed with HIV between 2006 and 2011 at a New York City academic medical center that provides care to substantial numbers of HIV-infected, largely African American and Latino adults, many of whom are diagnosed with HIV at older ages.
Methods
Study population and setting
Data were collected from a large academic medical center in Northern Manhattan. The medical center includes two hospital campuses with inpatient, ambulatory, and emergency services, a network of more than ten primary care clinics, and multiple specialty clinics. It is located in a community that is approximately 74% Latino, 29 has a median income of $38,320 with 25.8% of the population below the poverty line, 30 and has an estimated HIV prevalence of 1.7%. 31
Most HIV testing at the medical center is provider-driven, but dedicated HIV counselors are available for rapid testing at several of the larger ambulatory care clinics. Counselor-based rapid testing was available in the Emergency Department during weekday business hours for the interval of this study. A centralized HIV Counseling and Testing Service (CTS) receives all positive results of HIV tests conducted in the hospital laboratory and provides assistance with post-test counseling, epidemiologic reports, and referrals to care for newly diagnosed individuals tested at any site within the institution, both hospital and outpatient settings. Institutional Review Board approval for the study was obtained.
Data sources and variables
CTS program data was used to construct a sample that includes all individuals age 18 or over who were newly diagnosed with HIV at any site in our institution between January 1, 2006 and December 31, 2011. Since all positive Western blot results are reported to CTS, program files and the electronic medical record were reviewed to distinguish newly versus previously diagnosed individuals. Individuals whose records were too limited to determine if they were newly diagnosed and those newly diagnosed but without a CD4 cell count within 90 days of diagnosis were excluded.
Participants were classified as having a “late diagnosis” if they had concurrent HIV and AIDS diagnoses, defined as a CD4 cell count less than 200 cells/μL on first available result within 90 days of HIV test or an AIDS-defining illness within 90 days of HIV test. Additional outcomes included CD4 cell count less than 350 cells/μL on first available result within 90 days of HIV test, as well as HIV diagnosis in the hospital (inpatient or Emergency Department compared to outpatient).
The primary risk factor of interest was age, categorized as 50 years and older, as this has been determined to be a meaningful age cut-off for defining older adults with HIV infection based on immunologic response to ART and risk of death. 32 Other variables collected include race/ethnicity, gender, risk factor for HIV infection, location of HIV testing (inpatient, outpatient, or Emergency Department), prior visits to the medical center (inpatient admissions, Emergency Department visits, or outpatient clinic visits in 1 and 5 years prior to diagnosis), and co-morbidities including a current or past history of substance abuse and psychiatric illness.
Statistical analysis
Characteristics of the study population were summarized and described. Variables of those 18–49 years old were compared to those age 50 and older using χ2 and Fisher's exact tests where appropriate for categorical variables, and Student t test and Mann Whitney U test for continuous variables. Two separate logistic regression models were performed to evaluate late diagnosis and hospital diagnosis of HIV, as described above. Variables with clinical and epidemiological significance were included in the models. All statistical analyses were performed with SAS, version 9.3 (SAS Institute Inc., Cary, NC).
Results
There were 461 positive HIV test results in the CTS database from January 1, 2006 through December 21, 2011. We verified that 337 individuals were actually newly diagnosed with HIV during the study period. Of these, 50 individuals lacked CD4 cell counts within 90 days of diagnosis and were thus excluded, resulting in a sample size of 287. Twenty one percent (61 individuals) were age 50 or older, 70.4% (202) were male, 46.3% (113) were Latino, and 36.9% (106) were African American; neither gender nor race/ethnicity differed significantly between the two age groups (Table 1). There were differences in self-reported HIV risk factors in the older compared to younger age groups (p value<0.001): men who have sex with men (MSM) accounted for 38.1% of the younger group and only 18.0% of the older group, heterosexual sex was reported in 35.0% of the 18–49 year olds and 47.5% of those age 50 and older, and injection drug use (IDU) was the risk factor identified for 4.4% of the younger group and 16.4% of the older group.
p Value for comparison between the age groups; bvisit defined as inpatient admission or Emergency Department/outpatient visit at our medical center.
Significant differences were noted in the setting where diagnosis was made, initial CD4 cell count and viral load, and the presence of an AIDS-defining illness at diagnosis (Table 1). Overall, almost half (47.7%) of the study population was diagnosed as an inpatient with an additional 8.5% diagnosed in the Emergency Department. Individuals 50 years of age and older were more likely to be diagnosed as inpatients (70.0% vs. 41.7%). The median CD4 cell count at diagnosis was low overall at 259 cells/μL (IQR 54–467), but differed significantly (p=0.003) between younger adults (307 cells/μL, IQR 62–492), and older adults (97 cells/μL, IQR 22–291). Among the whole study population, 42.3% had CD4 cell count less than 200 cells/μL at diagnosis (36.4% of the younger group and 63.9% of the older group, p<0.001), 61.5% had CD4 cell count less than 350 cells/μL at diagnosis (55.6% of the younger group and 83.6% of the older group, p<0.001), and 30.7% had an AIDS-defining illness at diagnosis (25.7% of the younger group and 49.2% of the older group, p<0.001). There were no statistically significant differences for prior visits to the medical center, substance abuse, and psychiatric illness between the age groups.
A substantially greater proportion of older adults had advanced disease at the time of diagnosis: 68.9% in the older age group were diagnosed concurrent with AIDS, in contrast to 38.9% in the 18–49 age group. On bivariable analysis, age 50 and older (OR 3.47, 95% CI 1.89, 6.34) and risk factor of IDU (OR 3.78, 95% CI 1.34, 10.71) were associated with late diagnosis (Table 2). Age 50 and older (OR 3.13, 95% CI 1.63, 5.98) and IDU (OR 4.4, 95% CI 1.31, 14.75) remained significantly associated with late diagnosis in the multivariable analysis adjusted also for gender, race/ethnicity, year diagnosed, and prior visits to the medical center. In addition on the multivariable analysis, the odds of late diagnosis were 48% lower for women compared to men (OR 0.52, 95% CI 0.28, 0.98). Older age was also associated with CD4 cell count less than 350 cells/μL, adjusted for the same variables (OR 3.62, 95% CI 1.67, 7.89, data not shown).
Adjusted for year of diagnosis; bvisit defined as inpatient admission or Emergency Department/outpatient visit at our medical center.
CI, confidence interval; OR, odds ratio.
Similarly, older age, gender, and IDU were significantly associated with being diagnosed in the hospital on both bivariable and multivariable analyses (Table 3). In addition, on multivariable analysis, individuals reporting heterosexual sex as a risk factor for HIV acquisition were twice as likely to be diagnosed in the hospital (OR 2.20, 95% CI 1.11, 4.39) adjusted for age, gender, race/ethnicity, prior visits to the medical center, and year of diagnosis. Visits to the medical center in the year prior to HIV diagnosis was associated with a 51% reduction in odds of being diagnosed in the hospital (OR 0.49, 95% CI 0.27, 0.88).
Adjusted for year of diagnosis; bvisit defined as inpatient admission or Emergency Department/outpatient visit at our medical center.
CI, confidence interval; OR, odds ratio.
A fairly wide range of AIDS-defining illnesses was seen among those study participants found to have one, or more than one, of these conditions within 90 days of diagnosis (Fig. 1). Pneumonia caused by Pneumocystis jiroveci was the most common and accounted for 34% of AIDS-defining illnesses. This was followed by candidiasis of the esophagus, trachea, or lungs, seen in 21%, and toxoplasmosis identified in 9%. Fourteen other different conditions were found in study participants with an AIDS-defining illness at diagnosis. The spectrum of illness was similar in the older group compared to the younger group, with the exception of a higher representation of HIV-associated dementia in those 50 years of age or older.
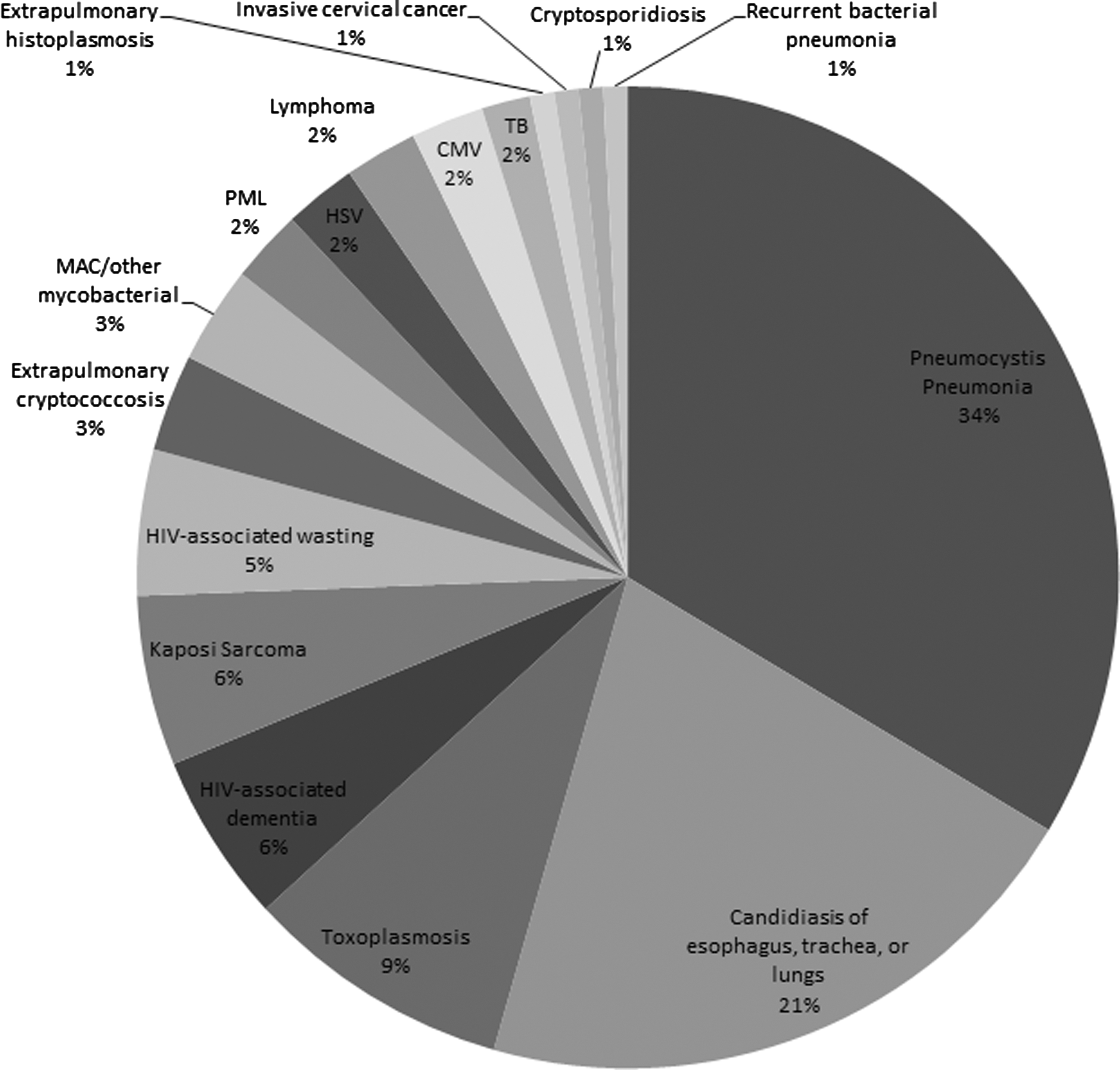
Spectrum of AIDS-defining illnesses at initial HIV diagnosis among participants. CMV, cytomegalovirus; HSV, herpes simplex virus; MAC, mycobacterium avium complex; PML, progressive multifocal leukoencephalopathy; TB, tuberculosis.
Discussion
We found that approximately one-fifth of new HIV diagnoses at our institution were among adults age 50 and older, and that this age group was more likely than younger adults to have a concurrent AIDS diagnosis. Overall, nearly half of the study population was diagnosed as an inpatient and concurrent with AIDS, but among the older adults these proportions were much higher, with 70.0% diagnosed inpatient and 68.9% concurrent with AIDS. Median CD4 cell count at diagnosis among those age 50 and older was one-third that of the younger adults.
This study demonstrates that older age, even after adjusting for other demographic characteristics, was associated with late diagnosis, consistent with what has been reported in several other studies. 19 –24 Data from the North American-AIDS Cohort Collaboration on Research and Design, a large cross-cohort collaboration including approximately 45,000 HIV-infected individuals from 13 North American cohorts, show that late presentation occurred with increased frequency among older adults. From 1997 to 2007, median CD4 cell count among those age 50 and older was significantly lower than in younger adults (266 vs. 336 cells/μL in 2007). 21 A study using the HIV/AIDS Reporting System of the Los Angeles Department of Public Health also found older age across all racial/ethnic groups to be associated with late HIV diagnosis in men. 23 In addition, two studies from the Southeastern United States, both with predominantly non-white study populations, showed older age to be associated with late diagnosis. 20,22 It is encouraging that some studies 24,25,27 have not found an association between older age and late diagnosis, which may be the result of regional differences in HIV testing behaviors, access to care, or screening practices of providers, but our findings remain in line with nationwide data.
We also found that women were less likely to be diagnosed late compared to men in adjusted analyses. This is consistent with much of what has been previously described 22,24,25 and may relate both to more regular use of the health care system by women in general and to pregnancy-related HIV screening. While we did not have a large sample of individuals with IDU as the risk factor reported for HIV infection, this was found to be independently associated with late diagnosis, also consistent with published data. Studies in Los Angeles and Houston found IDU and heterosexual sex to be associated with late diagnosis compared to MSM. 23,24 We did not find heterosexual sex to be an independent correlate of late diagnosis, but it is possible that this was the actual mode of transmission for many of those with unknown or missing risk factor, which could have changed the results of this analysis. We did, however, find heterosexual sex (in addition to the other factors associated with late diagnosis: older age, male gender, and IDU) to be associated with diagnosis in the hospital.
There are numerous reasons why older adults are more likely to be diagnosed with HIV at a late stage of disease. Inaccurate self-perception of risk among older adults has been shown in some studies. 33,34 For example, Akers et al. found that in a cohort of women above the age of 50, three-quarters self-reported being at low risk of HIV infection, yet almost half were determined to be at moderate to high risk. 33 Failure of medical providers to elicit a history of sexual risk behaviors from older adults 35,36 or to suggest HIV screening37 likely also contributes to this problem. Adekeye et al. found that a routine medical exam was the most common reason for an HIV test among adults age 50 and older, but also that only 25% of this population reported ever having been tested, which may represent missed opportunities on the part of primary care providers.37 In addition, even when older adults present with illness, medical providers often do not recognize the clinical signs of HIV and AIDS in this population. 2
Our study has several limitations. First, new HIV diagnosis was determined from the medical record and testing service records based on self-report. Additionally, there was insufficient information to determine stage of disease for all newly diagnosed individuals, resulting in a preferential exclusion of those diagnosed in the outpatient setting. However, the demographic characteristics of the excluded individuals were similar to those of the participants, and we had sufficient sample size for the analyses, therefore it is unlikely that the inclusion of these individuals would have substantially changed the results. Finally, there was missing or unknown information on HIV risk factors for some participants, although this is common in many HIV studies and in HIV surveillance data.
In conclusion, our study supports the finding that a very high proportion of individuals aged 50 and older are diagnosed with HIV at an advanced stage of disease, significantly later than younger individuals. Awareness of the vulnerable nature of older adults may aid in implementation of HIV screening recommendations in primary care settings—routine HIV screening in health-care settings for those aged 13–64. Community-based testing and education, as well as routinized screening in healthcare settings, should be evaluated to address the unmet needs of this population.
Footnotes
Acknowledgments
The authors thank Angelina Piles-Sherin, Paula Merricks-Lewis, and the whole CTS team, Ramon Negron for help with data extraction, as well as the clinical care providers.
Bristol-Myers Squibb Virology Fellows Research Training Program provided funding for this study, but did not have a role in study design, data collection, analysis, or interpretation of data.
All authors had access to the data and a role in writing the article.
Author Disclosure Statement
Tanya Ellman received a fellows research training grant from Bristol-Myers Squibb, but does not feel it reflects a conflict of interest given the role stated above. All other authors declare they do not have conflicts of interest.