
Abstract
Medication adherence is a major determinant of antiretroviral (ARV) treatment success and a significant challenge for HIV-positive patients, yet a well-defined adherence threshold to maintain virologic suppression on current ARV regimens remains unclear. The present study evaluated 1915 Kaiser Permanente Southern California HIV-positive patients on one of three regimen types: (1) emtricitabine–tenofovir–efavirenz (FTC-TDF-EFV); (2) emtricitabine–tenofovir (FTC-TDF) and raltegravir (RAL); and (3) FTC-TDF and a boosted protease inhibitor, either darunavir (DRV) or atazanavir (ATV), to compare virologic failure rates between patients with varying levels of adherence to the regimens. Medication possession ratios (MPRs) were calculated to determine adherence, and HIV RNA PCR levels drawn 12–18 months after the initial pharmacy claim for the measured drug were used to determine virologic failure, which was defined as two consecutive HIV RNA PCR measurements ≥200 copies/mL. Adherence was inversely related to virologic failure, with an 80–90% MPR threshold resulting in no more than 3.5% virologic failure rate. In comparison, ≥90% MPR yielded no more that 1.1% virologic failure rate. Although the gold-standard adherence threshold for older ARV regimens has been 95%, an 80–90% MPR appears sufficient to maintain virologic suppression in patients treated with these three ARV regimen types.
Introduction
C
The adherence threshold for ARVs needed to maintain virologic suppression has historically been set at 95%, but this figure was based on older, less potent unboosted protease inhibitor regimens. 3 –5 Few studies have attempted to define necessary adherence thresholds of newer ARV regimens, regimens that have now become first-line therapies recommended by major treatment guidelines, including those from the US Department of Health and Human Services and the International Antiviral Society–USA. 6,7 Evidence does suggest that the different classes of ARV agents require different levels of adherence to maintain suppression, but well-defined thresholds remain unclear. 8 –10 These newer regimens are far more potent and efficacious than the unboosted protease inhibitor regimens used to define the gold-standard 95% adherence threshold. Understanding the effects of these improved treatments on adherence thresholds is important to ARV regimen selection in HIV patients, particularly those with barriers to adherence.
The present study examined virologic failure rates across varying levels of adherence to three first-line ARV regimen types: (1) emtricitabine–tenofovir–efavirenz (FTC-TDF-EFV); (2) emtricitabine–tenofovir (FTC-TDF) and raltegravir (RAL); and (3) FTC-TDF and a boosted protease inhibitor, either darunavir (DRV) or atazanavir (ATV). The goal of the study is to define an adherence threshold necessary to maintain virologic suppression on these newer regimens that have become the mainstays of HIV treatment.
Methods
The study received Institutional Review Board approval. The study was conducted within Kaiser Permanente Southern California, a large integrated managed care organization. Data from electronic medical records of patients at least 18 years of age who were prescribed one of the three regimen types and filled the measured drug (either FTC-TDF-EFV, RAL, DRV, or ATV) at least once between August 31, 2007 and August 31, 2011, were retrieved. 11 Patients had to have at least one HIV viral load drawn during a 12- to 18-month follow-up period after the initial fill of the measured drug. Both treatment-naïve patients newly starting on ARV therapy and patients already virally controlled on one of the regimens of interest were included in the study. Patients could be included more than once if they switched from one regimen of interest to another regimen of interest during the study time period. Patients were excluded if: (1) they had a MPR of ≥90%, but never achieved virologic suppression on the regimen, indicating their viral strain was resistant to the regimen; and (2) they had no confirmatory HIV viral load level to determine virologic failure if their viral load measurement at the end of their follow-up period was ≥200 copies/mL.
Definitions of virologic failure have varied somewhat in the literature. 3,8,9,11 Due to testing limitations of the time, early adherence studies defined virologic failure as a viral load >400 copies/mL, and many more recent studies have retained this definition for comparison purposes. In an effort to distinguish between “viral blips,” measurable increases in viral load that revert to being undetectable while maintaining the same antiretroviral regimen, and true virologic failure, this study defined virologic failure as two consecutive HIV viral load levels ≥200 copies/mL. MPR was calculated for the measured drug in each regimen type, either FTC-TDF-EFV, RAL, DRV, or ATV, and this MPR served as a marker of adherence for the respective regimen. MPR was calculated by dividing the number of days of medication supplied to the patient during their study period by the patient's study period, which was the number of days from the patient's initial fill of the measured drug until their first HIV viral load laboratory date, 12–18 months after that initial fill.
Records for patients on all regimens were pooled and divided into three levels of MPR: (1) <80%, (2) 80–90%, (3) ≥90%. The primary objective of this study was to determine the adherence threshold that resulted in <5% virologic failure rate. Secondary objectives were to determine the adherence threshold that resulted in <20% virologic failure rate and to analyze the difference in virologic failure rate between the 80–90% MPR and ≥90% MPR groups. Chi-squared analyses were used to compare patient characteristics. Logistic regression and probit analyses were performed to examine the differences in virologic failure between patients with varying levels of MPR.
Results
Patient characteristics
Of 1972 patient records retrieved, 1915 patient records were eligible after exclusion criteria were applied. Eight records were excluded for patients who were ≥90% adherent but never reached viral suppression, and 49 records were excluded for patients without a confirmatory viral load level to determine virologic failure. Patient characteristics are shown in Table 1. Males predominated in all three MPR groups with an average age of 43 years. It is well-known that total medication and pill burden, as well as having certain types of concomitant medications prescribed in addition to ARVs can influence ARV adherence. 12 The study patients had, on average, eight to nine total medications prescribed to them during their study period in addition to their ARVs. Although patients in all of the MPR groups had low numbers of concomitant psychiatric or pain medications, the least adherent group of <80% MPR appeared to have slightly more of these types of medications prescribed during their study period.
Outcomes
Virologic failure rate was inversely related to MPR as shown in Fig. 1. The majority of patients fell into the higher MPR ranges, tightening the 95% confidence intervals with increasing MPR. However, both the logistic regression and probit analyses predicted virologic failure rates that fell within the 95% confidence intervals of the observed rates.
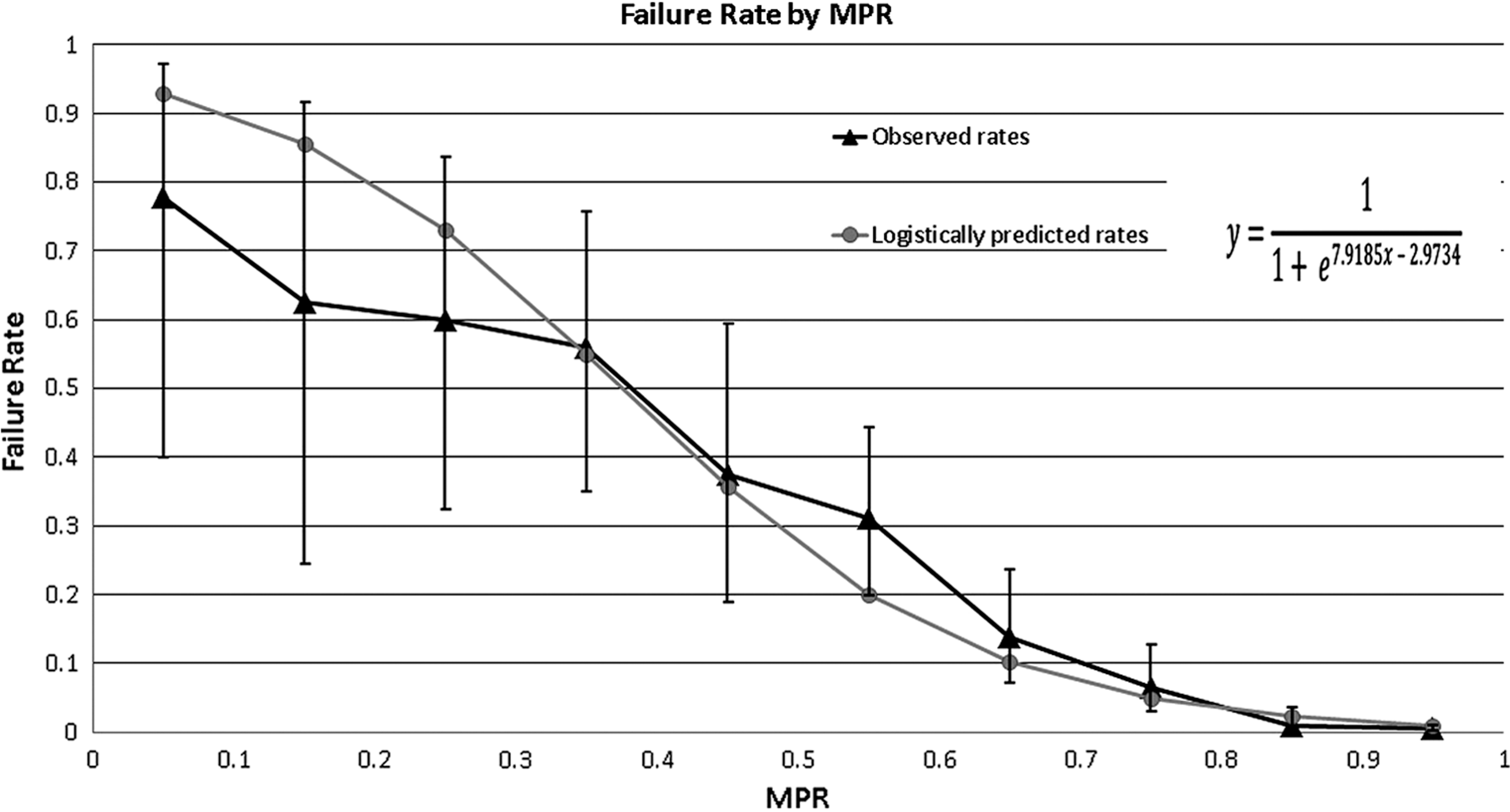
Failure rate by MPR.
Table 2 depicts the findings for the primary outcome. The MPR threshold that resulted in <5% virologic failure rate in this group of patients was 80–90%; more specifically, these data show that this level of MPR will result in no more than 3.5% virologic failure rate for patients prescribed the three ARV regimen types examined in this study. The most adherent patients with MPRs of ≥90% will have no more than 1.1% virologic failure rate on these regimen types. The study did not reach sufficient power to assess the secondary outcome to determine a statistically significant difference in virologic failure rates between the 80–90% and ≥90% MPR groups.
The results showed that 70–80% MPR is the adherence threshold necessary to achieve <20% virologic failure with a failure rate of 6.6% (95% CI, 2.9–12.6%). Below this level of MPR, virologic failure rate rises much more steeply with decreasing adherence.
Discussion
As expected, higher levels of virologic failure were associated with lower levels of MPR, with failure rates rising steeply below the 70–80% MPR range. However, the 70–89% MPR meets the threshold for the secondary outcome of <20% virologic failure rate. Compared with the gold-standard Paterson study which necessitated 95% adherence to achieve 22% virologic failure, these results support the increased potency and efficacy of these newer ARV regimens. 3
ARV adherence studies subsequent to the Paterson study accepted virologic failure rates of <20% to define adherence thresholds. 10 This study aimed for a more stringent virologic failure limit of <5% that should be more attainable with today's available ARV agents, as well as more informative for clinicians in selecting regimens for patients with a history of non-adherence. For the pooled analysis of patients on FTC-TDF-EFV, FTC-TDF and RAL, and FTC-TDF plus either boosted DRV or ATV, a MPR of 80–90% met this primary objective, resulting in no more than 3.5% virologic failure rate.
A MPR of ≥90% to these regimen types resulted in no more than 1.1% virologic failure rate. In order to achieve sufficient power to compare the virologic failure rates between the 80–90% MPR and ≥90% MPR groups, approximately 5700 patients per group would be needed, a sample size not achievable with the current HIV-positive Kaiser Permanente Southern California patient population. Although this study cannot determine a statistically significant difference in virologic failure rates between these two MPR groups, from a clinical practice standpoint, the difference between 3.5% failure rate and 1.1% failure rate is negligible, particularly in light of literature acceptance of failure rates up to 20%.
The threshold of 80% adherence is an important figure. Adherence studies for other chronic disease states consistently define 80% adherence as the cut-off between adherent and non-adherent patients. As HIV has become a chronic disease and as ARV agents have dramatically improved since the FDA-approval of zidovudine in 1987, it is plausible that today's ARV adherence requirement to maintain virologic suppression in HIV-positive patients is less than the 95% gold-standard observed by Paterson et al. in 2000.
Also reinforcing the issue of adherence threshold in HIV management is the potential for upcoming regulation from the Centers for Medicare and Medicaid Services (CMS). Although not in place yet, CMS is proposing a potential 5 Star Measure that would require an institution to achieve 90% adherence to ARVs amongst its patients. This figure differs from the traditional ARV adherence gold-standard of 95%, and also differs from the chronic disease gold-standard of 80%. There are many ways to calculate adherence, none of which are directly comparable to each other, and it is not yet clear what method CMS will use. However, the results of this study support the idea that newer ARV agents require lower adherence thresholds to maintain virologic suppression, and that adherence requirements for HIV management may not need to stand alone at 90% or 95%, but could be more in line with the requirements for other chronic disease states at 80%.
Study limitations should be considered. Multiple methods exist in the literature for calculating adherence, and no gold-standard has been established as the method that best represents how often a patient is taking his/her medication properly. 13,14 All methods rely on markers of adherence, such as pill counts or pharmacy refill records, which do not necessarily represent patients' actual adherence level. Prospective adherence studies do not solve the problem and, in fact, may be less representative of a patient's true adherence as there is an incentive to patients to be adherent to remain eligible for otherwise prohibitively expensive or inaccessible treatment.
MPR is an adherence measure that, in the case of this study, was based upon pharmacy refill records. In addition to the inaccuracy introduced by relying on these records, MPR will also overestimate patients' adherence if patients refill their medications early, as the calculation does not adjust for the overlap in the number of days of medication supplied to the patient, and in effect, those days will be double-counted in the numerator of the MPR calculation. Furthermore, many factors impact patient medication adherence, including gender, co-morbities such as depression and other psychiatric illness, pain, intravenous drug use, follow up in health care systems, socioeconomic status, and many more. 15,16 This study did not evaluate the above listed impacts on adherence. This study also required that patients have at least one pharmacy claim for the measured drug and also that they have at least one HIV viral load level drawn 12–18 months after the date of that initial fill. This introduced some amount of selection bias into the study as patients had to have this baseline level of adherence to be eligible; completely non-adherent patients were not captured.
In addition, this study included both treatment-naïve patients newly starting on ARV therapy, as well as patients already virally controlled on an ARV regimen. It is known that the level of adherence necessary to maintain virologic suppression after a long period of suppression is less than that needed at treatment initiation, particularly when patients have a high initial viral load. 17 This study did not have the power to analyze these two groups separately, and therefore, these results may underestimate the rate of virologic failure in treatment-naïve patients.
The study also excluded patients with both >90% MPR and virologic failure. Since this study did not look at genotypes, excluding these patients can underestimate failure rate. However, including these patients could also confound the results, since patients started on a regimen to which they are resistant would not achieve virologic suppression at any level of adherence. However, this only encompassed eight patients (0.4% of the study population), which would not significantly affect the results. Sample size also limited the ability to evaluate the impact of MPR of each of the specific drug types (non-nucleoside reverse transcriptase inhibitor, integrase inhibitor, or boosted protease inhibitor) on virologic failure rate. Thus, the three regimens had to be pooled, and overall failure rates were assessed.
This study did not examine the effects of lower adherence levels to these ARV regimen types on the development of resistance patterns, which is of crucial importance for a disease that requires life-long medication management and that involves a highly-mutable virus that adapts to evade entire classes of ARV agents. This is an important area of future research for these newer ARVs. Another on-going challenge for all adherence studies across the gamut of disease management is to establish an accurate, cost-effective, and feasible measure of medication adherence that would allow for the true understanding of medication efficacy and for the comparison of outcomes across studies.
Conclusions
This study demonstrated that 80%–90% MPR to FTC-TDF-EFV, FTC-TDF and RAL, and FTC-TDF plus either boosted DRV or ATV will result in no more than 3.5% virologic failure rate. In a clinical-practice sense, this does not pose a significant difference in failure rate compared with ≥90% MPR that will result in no more than 1.1% virologic failure rate. With other studies in the HIV literature using virologic failure rates of up to 20% to define adherence threshold requirements, clinicians can be confident that patients who are 80–90% adherent to these three regimen types will achieve virologic suppression. However, HIV management also encompasses other considerations such as viral reservoirs, the effects of other inflammatory markers, and some evidence that suggests suboptimal adherence is associated with increased mortality. 18,19 Because of these reasons, in addition to the inherent complexity of medication adherence, the goalpost for ARV adherence should remain 100%.
Footnotes
Acknowledgments
This article is the result of work supported with resources and use of facilities at Kaiser Permanente Los Angeles Medical Center.
Author Disclosure Statement
No competing financial interests exist.