
Abstract
Since 2012, lifelong antiretroviral therapy for all HIV-positive pregnant women (“Option B+”) is recommended by WHO for the prevention of mother-to-child transmission of HIV (PMTCT). Many sub-Saharan African countries have since introduced this regimen, but to date, longer-term outcome evaluations are scarce. We conducted an observational study in Fort Portal Municipality, Uganda, to describe uptake and adherence of Option B+ during pregnancy. HIV-positive women approaching antenatal care (ANC) services in two hospitals were enrolled and followed-up at monthly routine ANC visits until delivery. At each visit, next to sociodemographic and clinical data, we assessed drug adherence through pill counts. In total, 124 HIV-positive pregnant women were enrolled in our study; from these, 80.8% had not been aware of their positive serostatus before. Forty-five PMTCT clients (36.3%) never returned to ANC after their first visit. Protective factors (p < 0.05) for immediate loss to care included previous HIV status knowledge, status disclosure before or at first ANC visit, and tertiary education. Among those clients starting Option B+, the median adherence during pregnancy was 95.7% pill intake. Rather low adherence (<80%) was observed in 21.1% of clients, while more than half achieved an adherence level of ≥95%, with 40.8% of all clients being 100% adherent. The cohort's median adherence remained stable throughout the course of pregnancy. Healthcare providers should place high emphasis on individual PMTCT counseling at first ANC encounter, and pay special attention to those women previously unaware of their HIV status. However, after initial uptake, high adherence seems to be feasible for Option B+.
Introduction
O
In 2012, the WHO published the latest programmatic update of PMTCT guidelines. 6 While prior guidelines 7 recommended two temporary antiretroviral prophylaxis options (Option A and Option B) limited to the transmission period during pregnancy and breastfeeding, the newly introduced regimen of Option B+ requires the initiation of all pregnant HIV-positive women on lifelong full antiretroviral therapy (ART), irrespective of their clinical condition, CD4 cell count, and gestational week. A major benefit of this new option is the simplified enrollment procedure, which enables even basic health centers to offer PMTCT services to their clients and therefore extends access to effective care to peripheral settings.
Option B+ offers highly effective and continued protection from vertical transmission, also with respect to a woman's future pregnancies, 8,9 avoiding the formation of resistant HIV strains due to starting and stopping antiretroviral drug intake between pregnancies. In addition, it provides a strong prevention benefit when it comes to sexual transmission in sero-discordant couples by suppressing the viral load in infected women. 10 –12
However, prior studies have identified low adherence as a barrier to effective prevention of HIV transmission. 5,13 –16 Option B+ is a lifelong therapy, continuously requiring a high level of adherence to the daily intake of antiretroviral medication. Mal-adherence to ART does not only affect the efficacy of the regimen in reducing transmission rates, but also harbors the risk of provoking the formation of drug resistant viral strains. 17,18 However, very few studies have so far investigated the acceptance and feasibility of Option B+ in terms of adherence rates in a real life, resource-limited setting.
Uganda introduced Option B+ to the national PMTCT guidelines in 2012. 19 Being a country with high fertility with an average of 5.9 births per woman 20 and an estimated number of 100,000 pregnant women currently living with HIV, 1 an effective PMTCT strategy in this setting is of crucial importance. Our aim was to evaluate the acceptance of Option B+ in a Western district in Uganda in terms of intervention uptake and adherence levels in pregnant HIV-positive women, and to assess potential influencing factors.
Methods
Study setting
This observational, longitudinal study was conducted within the frame of a larger PMTCT study in Fort Portal, the capital of the Kabarole district in Western Uganda. Antenatal care (ANC) coverage in Uganda is almost universal, with about 93% of women attending at least one ANC visit; the proportion of deliveries attended by skilled health personnel lies at 57%. 20 Maternal mortality is present at a high level, with approximately 440 maternal deaths per 100,000 live births. 20 Adult HIV prevalence was estimated at 7.2% in 2013. 1
The study setting comprised the two major hospitals in Fort Portal: Fort Portal Regional Referral Hospital (FPRRH) and The Holy Family Virika Hospital (VH). FPRRH is a public hospital, which is attended by about 260 first-time ANC clients per month, with five midwives taking care of these clients. First-time visits are carried out on every weekday. VH is a private Catholic nonprofit hospital, with four midwives and one clinical officer serving about 60 first-time ANC clients per month. First-time ANC visits are carried out once a week. Both clinics offer free standard ANC and HIV- related care to their clients.
Data collection
To establish a prospective cohort, study participants were recruited within ANC wards at their first antenatal visit and included into the study if they satisfied the following eligibility criteria: informed written consent, age above 18 years, confirmed pregnancy, and positive HIV status without prior ART enrollment. HIV status was established in a routine testing procedure using rapid HIV antibody test devices (e.g., Statpack, Determine, Unigold), which is offered as a standard procedure to all pregnant women at the first ANC visit, along with pre- and post-counseling. As soon as a woman was diagnosed with HIV infection, she was enrolled in Option B+ for PMTCT following the national guidelines. 19 All enrolled women were handed out Option B+ drugs at the first ANC visit.
Study participants were interviewed by ANC staff within their routine sessions using structured questionnaires. Collection of data did not interfere with routine ANC services following the national guidelines on HIV counseling, testing, and PMTCT care. Interviews were held in the local language and the study questionnaires were filled in English. The obtained data included information about the socio-demographic and economic status of the participants, as well as information on previous medical and obstetric history.
In order to compare patients' social status, a scale ranging from 0 to 8 was created, taking into account the availability of electricity, tap water, radio, television, radio, fridge, car, or a shelf in the household. To compare subjective health complaints in HIV-positive pregnant women, several symptoms (fever, headache, cough, shivering, weakness, abdominal pain, vomiting, loss of appetite, vaginal discharge, uterine contractions, other complaints) were quantified with a score from 0–3, according to whether the complaints were absent, mild, moderate, or severe; this score was subsequently added to form a complaint scale ranging from 0 to 33.
In addition, women were clinically and obstetrically examined by the ANC midwives, and a peripheral venous blood sample (2.7 mL) was collected for assessment of hemoglobin levels, CD4-count, and malaria testing. Hematological and serological examination, as well as processing and storing of blood samples, was done at VH. Anemia was defined as Hb <12.0 g/dL according to WHO recommendations. 21
Clients were followed up at each subsequent ANC visit, which were due every 4 weeks for routine pre-delivery check-ups and drug dispensing. Follow-up questionnaires were used to collect information on aspects such as timely return for the scheduled visit, clinical status, number of pills brought back, and disclosure of HIV status. For those women who delivered at either VH or FPRRH, an additional questionnaire was filled within 72 h of delivery. Clients who did not return after their first visit were defined as lost to follow-up (LTFU). Two non-returning clients whose gestational age at first visit had been >36 weeks were not classified as LTFU, as they had possibly delivered the baby before they could return. The data of these clients were used in determining baseline data, but was not included when assessing adherence.
Pill count adherence (PCA) was calculated by taking the difference between pills dispensed at the last visit and pills brought back, and dividing this by the number of days between two ANC visits, for example,
Statistical methods
Data obtained from questionnaires and laboratory forms were crosschecked and entered into an electronic database using Microsoft Excel. For statistical analysis, data were transferred to IBM SPSS. Descriptive analysis was carried out on patientś baseline information, and the two hospital groups were checked for differences. We assessed median adherence levels for each individual client and for the overall cohort. Median adherence was also assessed for each separate ANC visit to evaluate changes throughout the course of pregnancy. In bivariate analysis, socio-demographic factors such as age, education, occupation, social status, and distance to hospital, as well as clinical features such as CD4-count, week of gestation or parity, were analyzed to investigate their influence on LTFU after the first ANC visit and on adherence levels. Pearson's chi squared test or Fisher's exact test were used to analyze categorical data, while the Mann-Whitney U-test was used for analysis of metric factors. Odds Ratios (OR) of potential influencing factors were calculated using a Confidence Interval (CI) of 95%. A p value of <0.05 was considered as statistically significant.
Ethical considerations
Data were used anonymously and were treated as strictly confidential throughout conduction of the study. Women could withdraw their participation from the study at all times without explanation and without any adverse consequences for their continued healthcare. The study was ethically approved by the Committee of Higher Degrees, Research and Ethics, College of Health Sciences, Makerere University, Kampala, and by the Ugandan National Council for Science and Technology.
Results
Baseline characteristics of the study cohort
During the recruitment period, a total of 124 women were enrolled into the study. From these, 60 clients attended ANC at VH, and 64 women were recruited and followed-up at FPRRH.
Socio-demographic and clinical baseline data of the cohort are presented in Table 1. Women had a median age of 25 years, and a median gestational age of 21 weeks when approaching ANC for the first time. On average, women had previously delivered once, and 30 women (24.2%) were primigravidae. A CD4-cell count was carried out for 67 women (54.0%) at the first ANC visit. The median CD4-cell count was 486 cells/μL, ranging from 83 to 1851 cells/μL, and 19 (28.4%) women had a CD4-cell count of less than 350 cells/μL without being on treatment.
Prior to their first ANC visit, 97/120 (80.8%) clients had not been aware of being HIV positive. Of the 23 women who had been previously aware of their positive serostatus, the majority (19/23) had already disclosed their status by the time of their first ANC encounter. Prior status knowledge was more common among clients of higher age (p = 0.001) and among clients with a higher number of previous pregnancies (p = 0.005). However, patients aware of their status did not show any tendency to present to ANC earlier in pregnancy (p = 0.317).
Among those clients followed-up until delivery, a total of 75/78 (96.2%) reported to have disclosed their status at some point in the course of pregnancy. Of these clients, 55/79 (69.6%) disclosed to their partner, and 50/79 (63.3%) disclosed to family members. Among married clients, 36/48 (75.0%) disclosed their status to their husband. Disclosure of status was not associated with age, education, or marital status.
Clients who returned after the first ANC visit were also asked whether after their HIV status had been revealed, their partners would as a consequence decide to also get tested for HIV or accompany their wives to the ANC for couple counseling. 35/75 (46.7%) clients reported that their partners had been tested for HIV (following the clients' diagnosis), and 23/76 (30.3%) accompanied their pregnant partner to ANC at least once in the course of pregnancy.
Patients at the two hospitals did not differ regarding social status and education; patients at VH, however, tended to be older. Also, they were less likely to perform an income-generating activity and accepted a longer travel distance as well as higher travel cost to the clinic (Table 2). A significant difference was observed regarding prior knowledge of HIV status. At VH, a higher proportion of clients already knew their status before being tested at their first ANC visit. Before attending ANC, 21/56 (37.5%) clients at VH were aware of being HIV positive, compared to 2/64 (3.13%) clients knowing their status before at FPRRH (p < 0.001). Moreover, the proportion of women disclosing their status and having their partners tested for HIV was found higher at VH than at FPRRH. While at VH, a total of 45/52 (86.5%) women disclosed their status; only 35/63 (55.6%) women did so at FPRRH (p < 0.001). At VH, 23/40 (57.5%) of partners were tested for HIV, which was only the case for 12/35 (34.3%) clients at FPRRH (p = 0.044).
Mann-Whitney U Test; bPearson Chi 2 Test or Fisher's Exact Test where applicable.
Uptake of the intervention and LTFU
Of the 124 recruited clients, 45 (36.3%) did not return for ANC and PMTCT care after their first visit, while 79 were retained in care. Patients who had known their status before the first ANC encounter, as well as clients who had disclosed their status before or at first-time ANC attendance were significantly less likely to be lost to follow up after the first ANC visit (p = 0.049 and 0.019, respectively). The same was true for clients with education above secondary school (p = 0.031). Apart from that, other factors such as age, marital status, travel cost or distance, social status, gestational week at first visit, gravidity, or parity did not influence LTFU on a significant level (Table 3).
Pearson Chi 2 Test or Fisher's Exact Test where applicable.
According to clinical examination and laboratory test results, there was also no significant difference between the two groups considering axillary temperature, hemoglobin level, present anemia, CD4 cell count, positive malaria RDT result, or score of complaints at the first visit. In the group of clients that was followed-up, the median score of complaints remained stable on a low level and did not correlate with adherence.
Adherence
Out of the 79 followed-up clients, adherence measurement data was available for 76 clients (Fig. 1). The median pill count adherence was found to be 95.7% (range: 24.2–100%). Rather low adherence <80% was observed in 16 clients (21.1%), while moderate adherence of 80–94.9% was achieved by 21 clients (27.6%). An adequate adherence level of ≥95% was achieved by 39 clients (51.3%). From these, 31 clients (40.8% out of all) achieved full (i.e.,100%) drug adherence.
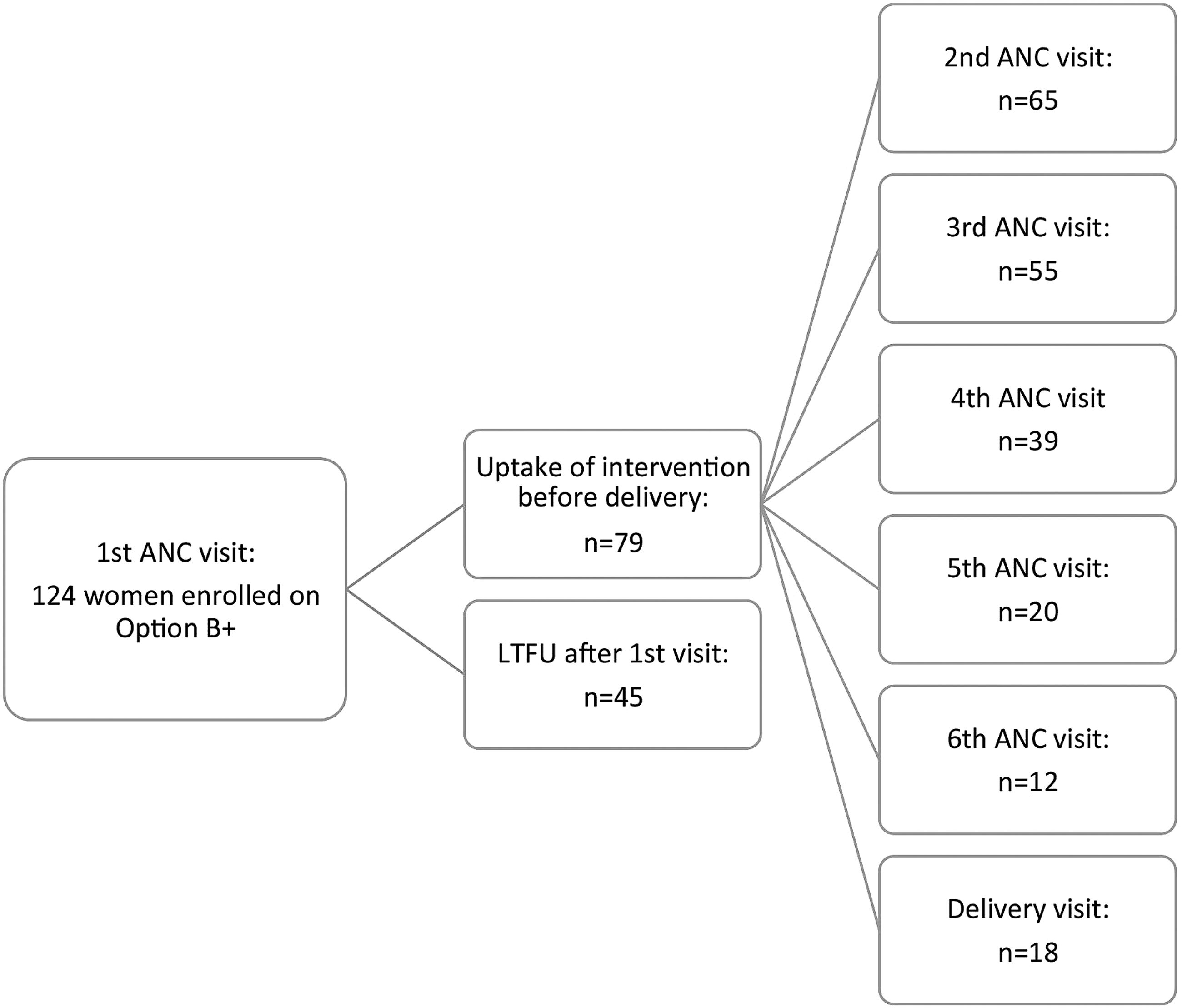
Option B+ enrolled women attending ANC visits.
Those clients who had taken up the intervention had a median of four pre-delivery ANC visits, with 58/79 clients (73.4%) attending three or more visits. The median amount of time between two visits was 29 days. In the course of pregnancy, adherence levels as well as the number of days between visits were found to remain stable with no tendency to decline during the course of the pregnancy (Table 4). Women who had taken up the intervention had a median ARV exposure of 129 days (range: 2–243 days) prior to delivery.
Most socio-demographic factors such as age, occupation, gravidity, or marital status were of no significant influence on adherence levels (Table 3). However, clients with education above secondary level were significantly less likely to achieve 95% adherence (p = 0.047), even though they were at the same time less likely to be LTFU cases (Table 3).
Discussion
To date, little research has been conducted to assess if Option B+ is feasible to implement in real-life settings in sub-Saharan Africa. In our study examining uptake and adherence of Option B+ in Fort Portal, Uganda, we found that a third of the PMTCT clients in our study setting was lost to care immediately after their first ANC visit. However, for those women who took up the intervention, high pre-delivery adherence was achieved.
Half of the clients who started the regimen took ≥95% of the required drugs before delivery, with the majority of these even taking 100% of pills. The high median adherence level of 95% remained stable throughout the course of pregnancy, irrespective of socio-demographic and economic factors. The majority of women returned to their ANC visits as scheduled, which furthermore indicates these women's motivation to adhere to the regimen.
Results of previous studies on adherence to PMTCT vary, and mainly refer to other PMTCT regimens than Option B+. Kirsten et al. 22 found a rather low median pill count adherence of 77% when assessing adherence to Option A in a rural Tanzanian setting. In Option A, women were required to start ARVs only at a gestational age of 14 weeks, meaning that women diagnosed at a lower gestational age were asked to come back later for PMTCT services. Also, the medication consisted of different pills for the pre-delivery, intrapartum, and postpartum period. Since this rather elaborate procedure required a higher level of commitment and effort both from the clients and staff, it is conceivable that this might have impeded adherence to some extent, and higher adherence in our study possibly indicates the benefits of the simplified Option B+ procedure.
Other recent studies on Option B or B+ presented even higher adherence rates compared to our study. Okonji et al. 23 found that 84% of their participants in Kenya had pre-delivery adherence rates >95% under Option B (ART until cessation of breastfeeding), possibly indicating that women adhere better to a regimen when knowing that they will only have to do so for a limited amount of time.
On the other hand, Mepham et al. 24 did not find a difference in adherence outcomes when comparing South African patients receiving Option B to patients receiving a short course of zidovudine monotherapy. The mean pill count adherence in this study was also found at a rather high level of 94.2%. Ayuo et al. 25 reported 89% of their clients in Kenya to be adherent to ART until delivery. Women in this study were likely to disengage from treatment later in the course of pregnancy, while in our study, adherence levels remained stable throughout pregnancy. However, adherence in the latter studies was determined by the use of adherence measurement questions, which only differentiate between “adherence” and “non-adherence” and do not provide information on exact levels of adherence compared to pill count.
The same applies to the study of Ebuy et al., 26 who identified 87.1% of their clients in Ethiopia to be adherent to Option B+. Although pill count as a tool for adherence measurement also depends on clients honestly declaring any leftover pills, prior research on its validity compared to other tools found rather positive evidence, 27 –29 and it is quite possible that adherence measurements relying on self-report alone and using only two categories lead to over-reporting compared to PCA.
Despite high overall adherence levels, it is an alarming finding that one-third of the cohort was lost to care immediately after the first visit. These women represent missed opportunities for preventing vertical transmission. The high immediate LTFU rate in our setting is consistent with previous research 14,15,30 –36 and outlines the importance of comprehensive counseling for new PMTCT clients at their first visit to prepare them adequately for Option B+ uptake.
Lacking prior HIV status awareness was identified as a factor increasing the risk for LTFU. Our results imply that status knowledge and HIV testing coverage represent a huge challenge, as has also been reported in other studies. The Uganda AIDS Indicator Survey 2011 furthermore reported that only 64.4% of women aged 15–49 years had ever been tested for HIV. 37 Despite the fact that this problem has been a known issue for several years, we still found a concerning rate of HIV-positive first-time ANC attendees being unaware of their positive status. Learning about an HIV-positive serostatus is likely to evoke emotional distress in the client. As a result, the capacity to process the information given about PMTCT procedures at the same visit, and to subsequently comply with them, might be severely compromised.
At the same time, almost a quarter of our study participants presented to ANC at progressed disease stage with a CD4-cell count <350 cells/μL, which would have qualified them for ART even without being pregnant, and which is associated with higher viral load and an increased vertical transmission rate. 38 This finding clearly implies the necessity to encourage and enable young women in their reproductive age to repeatedly test for HIV, in order to take action at the earliest possible time.
Among those clients who are aware of their seropositive status, disclosure to partner and family members remains a challenging issue. In agreement with preexisting research, our study has identified status disclosure as a positive predictive factor for intervention uptake. In other studies, disclosure has also been recognized to promote higher adherence levels. 22,24,26,39,40 However, we found that a quarter of married clients would decide to not disclose their status to their partner. Also, male involvement in HIV testing has frequently been identified as contributing to PMTCT uptake and adherence, but is mostly found at a low level. 33,40 –43 Our study shows rather low numbers of partners tested for HIV, with less than a third of partners willing to accompany their pregnant wife to ANC at least once for couple counseling.
Keeping in mind that one of the WHO's objectives for recommending Option B+ is to additionally help with lowering the transmission to sero-discordant partners, 6 and that there might also be a strong need for future safe conception counseling among those couples, 44,45 both couple counseling and testing and serostatus disclosure should be strongly encouraged by ANC staff, especially at the first visit. If a woman has no confidants in her family environment, it could be a successful strategy to establish a “treatment buddy” system within the healthcare setting or community groups, as it has helped to facilitate successful general ART implementation and adherence in other settings. 46,47 Implementation research would be helpful to evaluate such strategies in the context of Option B+.
Clients with tertiary education were found to be more likely to be retained in care, demonstrating that highly educated clients are usually more knowledgeable about the PMTCT options. According to the Uganda AIDS Indicator Survey 2011, only 71.8% of women were aware of the fact that mother-to-child transmission can actually be prevented. 37 Women with less than secondary education were even less likely to know about the opportunity of PMTCT. Therefore, ANC facilities should place special emphasis on counseling clients with poor education.
The results of our study also underline the importance of the specific ANC setting and of the quality of post-test counseling. VH, being a private Catholic facility, is offering post-test counseling in a separate room, while at FPRRH, post-test counseling is carried out in a non-private, frequented area of the ANC ward. Participants already knowing their HIV status were more likely to seek ANC at VH, probably due to more privacy and confidentiality in the facility. Later on, clients who were counseled in this setting were also more likely to disclose their status and have their partner tested for HIV.
This emphasizes the fact that PMTCT clients' health seeking behavior also depends on structural quality and the confidentiality of the ANC clinic. It has been long known that fear of stigma due to a lack of privacy in counseling can limit acceptance and uptake of PMTCT care. 48,49 Hence, when implementing Option B+ at local health centers, it should be ensured that the conditions provided will meet women's needs regarding confidentiality.
A limitation of our study was the fact that our study cohort of 124 patients was rather small and did not allow for multivariate analysis due to low case numbers per event in relevant variable subgroups. We acknowledge that multivariate analysis would have strengthened the utility of our results, however, gaining a larger cohort was unfortunately beyond the scope of this study. However, considering that continuously increasing numbers of HIV-infected women are nowadays enrolled in general ART programs, by implication cohorts of ART-naïve HIV-positive pregnant women remain rather small, and related research will have to concentrate on multicenter studies including high patient volume facilities. Yet, due to the paucity of studies accompanying Option B+ uptake to date, we view our findings nonetheless as highly relevant for improving implementation, while for the future, additional large-scale studies assessing Option B+ will be urgently required.
As another limitation, PCA undoubtedly represents a less objective and reliable option than assessing plasma drug levels. However, it should be noted that the latter is often not feasible, especially in the frame of an observational study. Furthermore, our present findings focused on the pre-delivery period, while Option B+ is a lifelong treatment. A recent study of Clouse et al. 14 found that women who were adherent during pregnancy frequently disengaged from treatment in the postpartum period. Evidently, ongoing research focusing on the postpartum period is needed in order to assess the actual, achieved transmission reduction through Option B+.
In conclusion, we found encouraging evidence regarding high pre-delivery adherence in women enrolled in Option B+, supporting the feasibility of this regimen in rural, low-resource settings like Western Uganda. Among women retained in care, adherence levels remained stable throughout pregnancy. However, low levels of HIV status awareness among pregnant women, as well as too many missed opportunities for PMTCT due to immediate loss to care after the first ANC visit require attention of healthcare providers.
In order to facilitate intervention uptake and to retain this client group in care, high emphasis should be placed on individual PMTCT counseling in a confidential environment at the first ANC encounter as well as on specific support for those women previously unaware of their HIV status.
Footnotes
Acknowledgments
We would like to thank all participating women, midwives, laboratory staff, and administration of both The Holy Family VH and Fort Portal Regional Referral Hospital. The study was funded and supported by the German Federal Ministry for Economic Cooperation and Development via the ESTHER programme (Ensemble pour une Solidarité Thérapeutique Hospitalière En Réseau). The sponsor had no role in study design, in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication. This work forms part of the doctoral theses of AS, ER, SD, and VB.
Authors' contributions: JR, NMT, GH, PB, and FPM designed the study. AS, ER, SD, VB, ST, and PB were responsible for patient recruitment, clinical and laboratory examinations. AS and ST did the statistical analysis and wrote the article with major contributions of the other authors. All authors read and approved the final article.
Author Disclosure Statement
All authors declare that they have no conflict of financial interests.