
Abstract

To the Editor,
T
Recent outbreaks of sexually transmitted infections in European countries suggest increased at-risk sexual behavior among MSM. 3 The Swiss Federal Commission for HIV/AIDS statement 4 and ART effectiveness in preventing HIV transmission in serodiscordant couples (reviewed in Loutfy et al. 5 ) have led to great debate about possible sexual risk compensation among people living with HIV (PLWH) with sustained viral load (VL) suppression, especially MSM.
The ANRS-VESPA and VESPA2 national cross-sectional surveys were performed among representative samples of adult PLWH attending French hospitals in 2003 and 2011, respectively. We assessed changes in sexual behavior among MSM using data from the two survey waves by considering the patterns of condomless intercourse in this population according to VL. The ANRS-VESPA and ANRS-VESPA2 surveys took place in French hospitals 8 years apart, with representative samples of 2932 and 3022 patients included, respectively. Eligible patients were >18 years old, living in France for more than 6 months, HIV diagnosed for more than 6 months, and currently attending participating outpatient services. In both surveys, independent trained interviewers administered face-to-face interviews, collecting data about patients' socio-demographic characteristics, their lives with HIV, and their sexual behaviors. Medical staff provided clinical data. Weighted and calibrated data represented the entire PLWH population followed up in French hospitals in 2003 and in 2011. 6,7
This study sample included 1117 MSM (ANRS-VESPA) self-defined as homosexuals or bisexuals reporting minimum one male sexual partner during the previous year enrolled, and 1337 MSM (ANRS-VESPA2) self-defined as bisexuals, gays, homosexuals, or who reported at least one male sexual partner during the previous 12 months.
Participants were asked whether they had any event of condomless oral sex and condomless anal intercourse with a serodiscordant steady partner (SSP) in the previous 12 months. A partner with HIV-negative/unknown status was considered a serodiscordant partner. For the most recent encounter with a casual partner (CP), condomless sex was defined as no condom use during oral/anal sex. Chi-squared tests and median tests were performed for categorical and continuous variables, respectively. All tests were carried out on weighted and calibrated data. Stata/SE 12.1 for Windows (StataCorp LP, College Station, TX) software was used for analyses.
HIV-positive MSM represented 35.6% (n = 1117) and 39.1% (n = 1337) of the 2003 and 2011 survey participants, respectively. There was no significant difference between ANRS VESPA and ANRS VESPA2, about nationality (94.7% and 93.6% French, p = 0.40, respectively), educational level (57.1% and 56.5% secondary or lower level, p = 0.78, respectively), and being in active employment (61.1% and 59.4%, p = 0.46, respectively). Compared with 2003, in 2011 MSM were significantly older (median [interquartile range, IQR] 49 [42–55] versus 41 [36–47] years, p < 10−3, respectively); more likely to live in stable housing (N (%) 1232 (92.8) versus 977 (88.9), p = 0.004, respectively); living with HIV longer (median [IQR] 14 [6–20] versus 9 [5–14] years, p < 10−3, respectively); and more likely to have CD4 cell counts >500 cells/mm3 (N (%) 825 (62.2) versus 517 (49.9), p < 10−3, respectively) or an undetectable VL (<400 copies/mL, N (%) 1178 (90.5) versus 729 (66.2), p < 10−3, respectively). In 2011, MSM were significantly less likely to be sexually active in the previous 12 months than in 2003 (N (%) 1040 (79.2) versus 950 (87.2), p < 10−3, respectively) and to report satisfaction with their sexual life (N (%) 204 (19.5) very satisfied versus 359 (39.1), p < 10−3, respectively). No significant difference was observed regarding having a main partner (N (%) 619 (56.9) in ANRS-VESPA and 761 (58.6) in ANRS-VESPA2, p = 0.42) or the number of CPs in the previous 12 months (median [IQR] 2 [0–10] in both surveys, p = 0.24).
A majority of MSM had an SSP, 403 (64.5%) in ANRS-VESPA and 501 (66.7%) in ANRS-VESPA2, and among them there was no significant difference in the rate of condomless intercourse with such partners in the previous 12 months: 78.9% (ANRS-VESPA) versus 86.1% (ANRS-VESPA2) p = 0.06 for oral sex and 22.9% versus 25.1% p = 0.64 for anal sex, respectively (Fig. 1, upper panel). However, among MSM having a detectable VL (>400 copies/mL), 386 and 125 in ANRS-VESPA and VESPA2, a decrease was observed in condomless oral (22.7% versus 8.5%, p < 10−3, respectively) and condomless anal sex (6.7% versus 1.3%, p = 10−3, respectively) with such partners in the ANRS-VESPA2 survey. In ANRS-VESPA and ANRS-VESPA2, 680 and 770 MSM reported CPs in the previous 12 months, respectively.
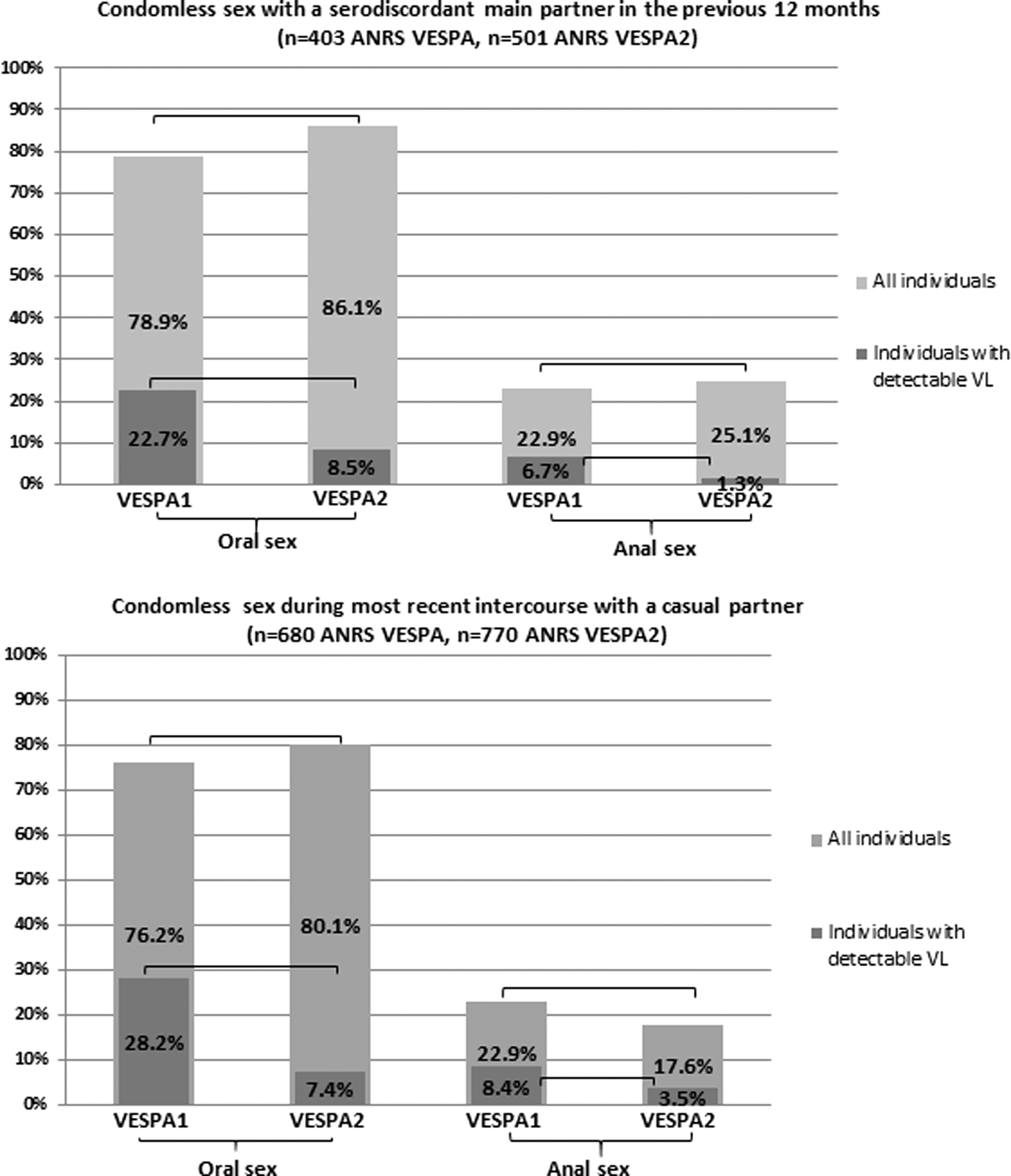
Patterns of condomless sex among sexually active MSM enrolled in the French national representative ANRS VESPA (n = 1040) and ANRS VESPA2 (n = 951) surveys. MSM, men who have sex with men.
At the most recent episode of intercourse with a CP, no overall difference in the proportion of condomless oral (76.2% [ANRS-VESPA] versus 80.1% [ANRS-VESPA2] p = 0.18) or condomless anal sex (22.9% versus 17.6% sex p = 0.07, respectively) was observed (Fig. 1, lower panel). MSM with a detectable VL in ANRS-VESPA2 survey were significantly less likely to report condomless sex than those in ANRS-VESPA (28.2% versus 7.4%, p < 10−3 for oral sex and 8.4% versus 3.5%, p = 0.02 for anal sex, respectively). Our analysis revealed no decrease in condomless intercourse in HIV-positive MSM between the two waves of the French national representative VESPA survey in 2003 and 2011, except among those with a detectable VL, that is, likely to transmit HIV. Both ANRS-VESPA and ANRS-VESPA2 were cross-sectional. Accordingly, we could not evaluate changes in sexual risk behavior before and after treatment initiation or VL suppression. In 2011, more than 62% of MSM had a CD4 cell count >500 cells/mm3 with more than 90% having a controlled VL, indicating improvements in clinical status since 2003. 7
In the French context of free widespread access to HIV treatment and care, we found that increased ART efficiency over an 8-year interval did not translate into increased sexual risk behavior. Yet, the overall trend suggested no decrease in condomless intercourse either, especially during anal sex, which is the most at-risk transmission practice. The latter fact might be the result of sexual disinhibition. Major changes in the field since 2003 may also explain this result, for example, the Swiss statement in 2008 4 and ART effectiveness in preventing HIV transmission. 5 Although we could not analyze the relationship between sexual risk behavior and patient awareness of the Swiss statement, of patient perception of transmission risk, or indeed of treatment and undetectable VL as prevention tools, the 2011 results do not support the argument for sexual disinhibition and overall remain comparable with those from 2003. 8,9
We used condomless sex to measure the pattern of sexual risk behavior, knowing that this does not necessarily mean unprotected intercourse. 10 The great majority of condomless intercourse was reported by virally suppressed MSM. The large decrease in condomless intercourse among MSM with a detectable VL in 2011 compared with those in 2003 may be thanks to transmission risk awareness and fear of transmission to partners. Moreover, we cannot exclude the possibility that MSM who engaged in condomless intercourse, whatever their VL, adopted risk-reduction strategies with serodiscordant partners (e.g., seroadaptive behaviors, strategic positioning, or withdrawal). 10
To have a real impact on the HIV epidemic in MSM, behavioral change interventions for those infected will not be enough. Improving HIV testing and treatment of undiagnosed MSM is crucial, as they are important drivers of the epidemic.
Footnotes
Acknowledgments
We thank all PLWH and all members of the medical staff who agreed to participate in the ANRS-VESPA2 survey, as well as the community-based organizations AIDES and Act-Up Paris who provided support throughout the survey. Finally, we thank Jude Sweeney for revising and editing the article. The ANRS-VESPA2 Study Group: F.L. and B.S. (scientific coordinators), Patrizia Carrieri, R.D.-S., Christine Hamelin, Nicolas Lorente, M.P., and M.S.-M., with the collaboration of Marion Mora. The VESPA2 survey was sponsored and funded by the French National Agency for Research on AIDS and Viral Hepatitis (ANRS).
Author Disclosure Statement
No competing financial interests exist.