
Abstract
Research has demonstrated the clinical effectiveness of pre-exposure prophylaxis (PrEP) for HIV prevention, but little is known about how factors at the individual-, interpersonal-, community-, and structural levels impact PrEP use for black men who have sex with men (BMSM). We advance existing work by examining how all levels of the ecological framework must be addressed for PrEP to be successfully implemented as an effective HIV prevention approach. We interviewed 31 BMSM three times each and 17 community stakeholders once each; interviews were taped, transcribed, and analyzed using the constant comparative method. Factors that influence how BMSM experienced PrEP emerged across all levels of the ecological framework: At the individual level, respondents were wary of giving medication to healthy people and of the potential side-effects. At the interpersonal level, BMSM believed that PrEP use would discourage condom use and that PrEP should only be one option for HIV prevention, not the main option. At the community level, men described not trusting the pharmaceutical industry and described PrEP as an option for others, not for themselves. At the structural level, BMSM talked about HIV and sexuality-related stigmas and how they must overcome those before PrEP engagement. BMSM are a key population in the US National HIV/AIDS Strategy, yet few individuals believe that PrEP would be personally helpful. Our research indicates the urgent need to raise awareness and address structural stigma and policies that could be substantial barriers to the scale-up and implementation of PrEP-related services.
Introduction
P
PrEP could help reduce HIV incidence among MSM, 6 who account for approximately two-thirds of new HIV infections in the United States. 7 Black MSM (BMSM) have the highest HIV incidence rates in the United States; reduction of such disparities is a vital part of the US National HIV/AIDS strategy. Though HIV disparities are stark for BMSM, PrEP has not been embraced in the way public health officials had hoped, even in resource-rich settings such as New York City (NYC). By spring of 2014, only 41% of MSM in NYC had heard of PrEP and only 3% had ever used PrEP. 8
The ecological framework and PrEP use
The CDC and its partners are pursuing a “high-impact prevention” approach to reduce HIV infections. 9 Given the broad range of social (e.g., housing, employment, racism) and interpersonal factors that impact HIV vulnerability for BMSM, we applied the ecological model to frame our analytic approach of factors that shape MSM's engagement with PrEP. The majority of PrEP research has addressed the individual level, but HIV prevention research suggests that acknowledging all levels of Bronfenbrenner's (1979) ecological systems will be imperative for the successful implementation of PrEP. These levels include the: (1) individual (attitudes, knowledge); (2) interpersonal (friends, partners); (3) community (medical mistrust, healthcare settings); (4) and structural levels (stigma, healthcare policies). Each level uniquely contributes to how individuals engage with HIV prevention measures and come to understand PrEP (Fig. 1).
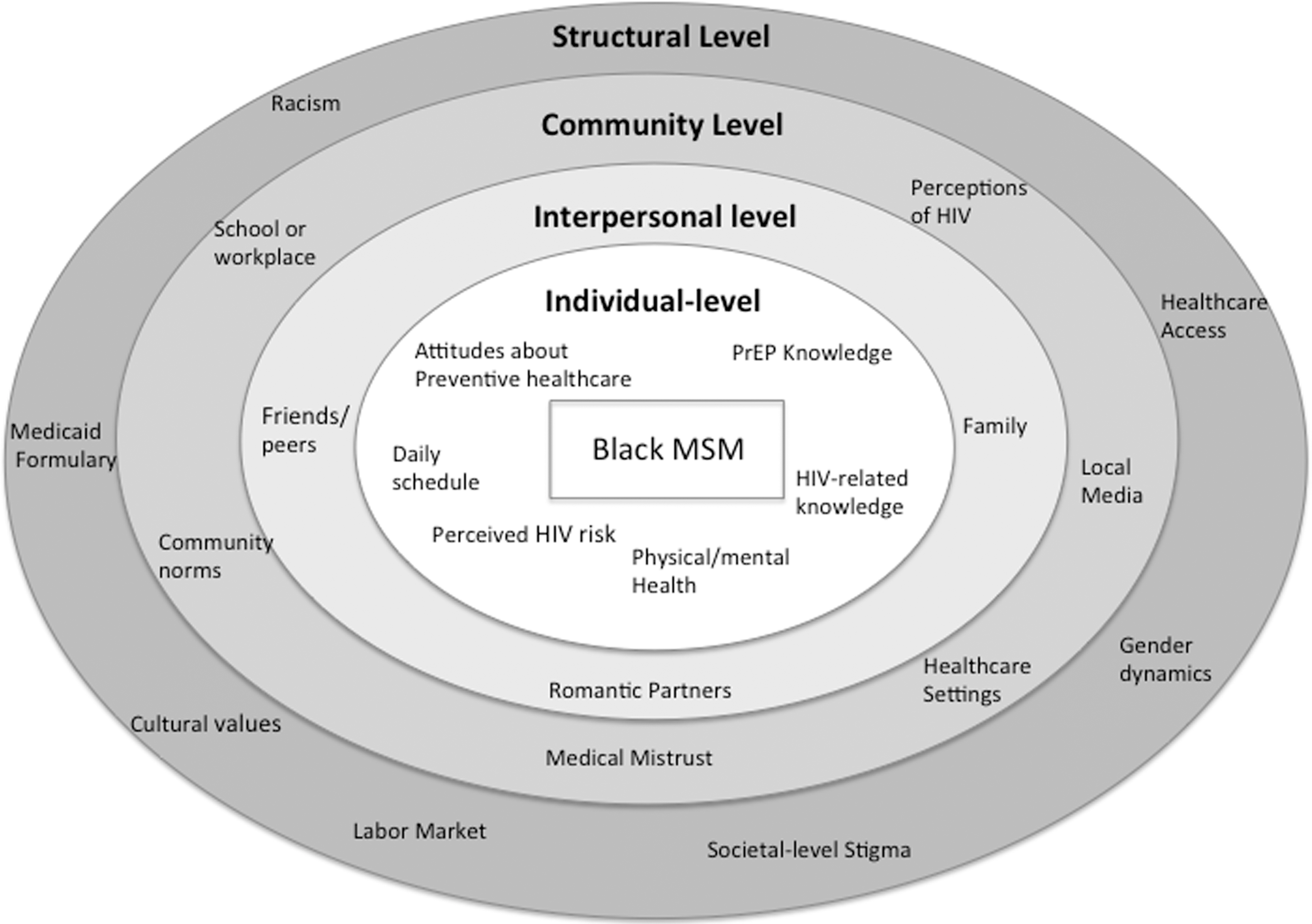
Ecological model of factors that impact pre-exposure prophylaxis attitudes and uptake among black MSM.
PrEP research on individual-level factors has found a range of PrEP-related knowledge and acceptability. 10,11 Men often lacked a comprehensive understanding of PrEP, though men aware of PrEP were also at the greatest risk of infection (e.g., due to having sex while high 12 ). The intent to use PrEP has also been associated with no perceived side-effects. 13 Researchers exploring interpersonal-level factors have cautioned that PrEP may lower perceived risk and increase condomless sex, 14 though results are mixed. 12 A recent study described the importance of community-level factors, finding that BMSM's interest in PrEP was contingent on cost, accessibility, and healthcare access, 15 particularly since many lacked health insurance. 16,17 Little research has examined medical mistrust and PrEP uptake, though one survey identified discomfort talking to physicians about sleeping with men and race-based medical mistrust as barriers to PrEP use. 18 Structural-level stigma has been associated with HIV risk and acquisition, as well as with lower adherence; studies have also demonstrated that lower PrEP-related stigma 19 and structural stigma 20 are associated with PrEP acceptability and use. 21
Purpose
Existing research into PrEP uptake has focused almost exclusively on the individual level of the ecological model. Here, we advance existing work by examining how all levels of the ecological framework must be addressed for PrEP to be successfully implemented as an effective HIV prevention approach.
Methods
This study (June 2013–May 2014) included three in-depth interviews each with 31 BMSM (average, 90 min) in NYC who were at least 15 years of age, male, and reported sex with a man in the past year. Men were recruited through outreach in bars, clubs, community health centers, and the Internet, with the goal of diversity related to sexual identity, age, insurance coverage, and income, though lower SES men were overrepresented in the final sample (Table 1). Interview topics included family, education and work history, sexual history, sexual and racial identity, healthcare seeking, and knowledge and attitudes toward HIV prevention and PrEP. Men received a total of $150 for participation ($40 for the first two interviews and $70 for the third). We also conducted 17 semi-structured interviews (average, 60 min) with community stakeholders (e.g., outreach workers, community mobilizers, healthcare professionals) who were involved in HIV prevention and/or BMSM health. They were asked about institutions and support available to BMSM and knowledge and attitudes about BMSM and HIV prevention. Stakeholders were compensated $50.
PrEP, pre-exposure prophylaxis.
All participants provided verbal informed consent: Their understanding was assessed by a series of follow-up questions; data analysis began after verbal consent. The Medical Center Institutional Review Board approved all aspects of this study.
Interviews were digitally recorded and transcribed verbatim. Interview data were analyzed and triangulated between and across cases using Atlas.ti 7.0 qualitative software. These analyses employed a codebook that was developed based on domains (code families) derived from the interview guides and line-by-line coding. The analysis for this article used the constant comparative method 22 to explore the varied ways that men talk about PrEP, seem willing to engage with PrEP, and understand PrEP. Descriptions of PrEP did not vary significantly between BMSM and community stakeholders; their responses are, therefore, combined in this article.
Results
Participants' average age was 29, and most were unemployed or unstably housed. More than half had Medicaid or were uninsured and were identified as gay or same-gender loving (Table 1). Approximately three-quarters of the men attended community clinics, though primarily for HIV testing and not routine check-ups. The majority of participants had never heard of PrEP, despite PrEP's availability in multiple clinics and inclusion in the state Medicaid formulary. We use the ecological framework to organize our presentation of the numerous factors men described that both supported and challenged their desire for, and ability to take, PrEP. Additional quotes are included in Table 2.
Individual level
In addition to PrEP-related challenges reported elsewhere (e.g., daily adherence and cost), 12 major individual-level barriers to PrEP engagement were confusion about effectiveness and concerns about potential side-effects.
Beliefs about PrEP effectiveness
Many men expressed confusion over the meaning of a 90% effective pill, and whether the effectiveness referred to risk per sex act or meant that some people were more protected than others. Men grappled with whether 90% effectiveness was sufficient to offset additional risks, and with what 90% effective actually means (e.g., being “1 out of the 10” as opposed to transmission risk per sex act). As one man noted: “It was 90% chance that it's preventative. I'm like, 10% is still pretty big. You know, even 1%—somebody has to make up the 1%, so it still happens” (22, gay).
Fears of side-effects and providing medication to healthy people
The majority of men questioned whether PrEP's efficacy was sufficient to counteract the potential side-effects, which some participants used as a rationale for eschewing PrEP: “It reduces your bone density and how do you correct that? There's really nothing you can do once your bone mass is lost. So taking that pill, it's basically damaging you” (20, discreet). This was described as particularly true since other HIV prevention methods lack side-effects. Some men were adamant that healthy people should not put drugs in their bodies, especially if they already struggled with adherence to medications for existing conditions (e.g., diabetes or asthma). One man shared how “doctors and clinics don't want to voluntarily give medicine to healthy people…‘cause they're healthy people and you're just like, you're voluntarily giving them a drug regimen’” (22, gay).
Interpersonal level
Interactions with friends, family members, and sexual partners also influenced the desire for PrEP. Principle concerns expressed by participants included risk disinhibition and sexually transmitted infections (STIs), and how PrEP fit into a range of prevention options.
Risk disinhibition and STI risks
Some men expressed concern that PrEP use would decrease condom use among their partners and sexual networks. Men saw condoms primarily as an HIV prevention tool and thus something that would be used in lieu of, not in combination with, PrEP. Responses depicted how behaviors might shift with PrEP use: “You're going to give me a pill and tell me that with this pill I cannot catch HIV, which means that it's going to make people feel as if it's okay for me to go out and have unprotected sex…Why would you want to do that?” (24, gay). Some men repeated that PrEP would not project against other STIs, and that condoms should still be used. One community stakeholder saw this tension as particularly dangerous: “I think it actually does more harm because it leaves us open for other diseases. The condom is the reason for syphilis and gonorrhea and other things that are sexually transmitted.”
No single solution
Most men described PrEP as simply one more option for HIV prevention, and they suggested the importance of maintaining as many means of prevention as possible. One community stakeholder suggested that PrEP messaging focus on integrating PrEP and condoms, “I think the messaging needs to be very clear that…it's important to continue to promote the importance of condoms and screenings for STDs and make sure that you're STD free if you're gonna start using PrEP.” Another individual noted that, due to the diversity of BMSM, PrEP should be framed as part of a toolkit, not the only option: “I feel like we need a whole lot of different options when it comes to prevention—the community is so diverse…condoms is one thing. Being abstinent is one thing. Being tested and being with only one partner is one thing but it's important to have pills also to help you stay negative and also therapy. I feel like all that is important” (29, gay).
Community level
Community-level themes include medical mistrust and the framing of social risk, specifically viewing PrEP as something that only other people need.
Medical mistrust
Mistrust of both the pharmaceutical industry and healthcare providers was widespread. Some men explicitly referred to historical abuses by pharmaceuticals and research (e.g., Tuskegee Syphilis Study), and how they profit from BMSM: “You would have a hard time selling that [even with] 99.9 percent efficacy coming from pharmaceutical companies…particular to people of color.” Some of the younger men were less vocal, but they still harbored skepticism. One participant noted that, although the pill might work, he still wanted to wait: “I'm not gonna start taking it off the bat, give it a couple more years, see what studies are done, and the information about it” (19, bisexual).
Who needs PrEP?
Men frequently discussed the concept that social researchers would define as “social risk,” and how HIV-related stigma challenged their willingness to accept their own actions as potentially risky. The majority of men described their behaviors as “normal,” or even declined to discuss them at all, and thus did not feel the need to take a daily pill to prevent HIV. When men were asked who should take PrEP, responses focused on the type and amount of sex that people were having, and often involved words such as “slutty,” “promiscuous,” or sexual positioning (i.e., bottoms versus tops). One man felt that PrEP users should be “people who have lived the lifestyle of just hooking up or being out there, just being free…If you're out there and just living life and meeting guy after guy after guy” (18, gay). Men consistently talked about PrEP as something that would be useful for others, but not for themselves. One participate summed it up explicitly, “I think it is good for the whole world, it's good for the community, so yeah, it's gonna work, it just ain't gonna work for me… I don't want to know about the pill because I don't care about the pill. I ain't never fucking taking the pill” (45, straight).
Structural level
The structural level includes social institutions, cultural dimensions, economic organizations, and political structures that affect society as a whole. The high levels of stigma (a social and cultural structure) attached to HIV/AIDS, sexuality, race, and gender performance shaped BMSM's everyday lives and attitudes toward PrEP. The interviewees also described how economic factors such as housing instability and the labor market would impact their ability to take PrEP.
Stigma and PrEP
Most men described how PrEP use could result in HIV stigma, and they feared that friends, family, or sexual partners might see a PrEP bottle and assume they were HIV positive. This would require people to take the pill in secret, which complicates adherence: “People don't like taking any medicine in front of people. Maybe they feel like a stigma would develop from what you are taking? People be nosy, like what's that you taking?”(27, same-gender loving). A few men also described how internalized stigma could impact PrEP uptake. Asking for PrEP would force a man to accept that he was having sex with other men, often without a condom, and was thus at risk for HIV. As one community stakeholder described, “You've got to accept within yourself that you love and enjoy sex with a man every single day, and you may like it raw 90 percent of the time. But then that's like accepting, ‘Oh, I'm going to get HIV. Oh, I'm just another fag.’”
Structural barriers to PrEP use
Even men who expressed interest in taking PrEP reported structural barriers that reflected intersecting inequalities of race, sexuality, and socioeconomic status. Nearly all BMSM reported unstable housing, often as a result of their sexuality (e.g., being kicked out of their home for having sex with men), which complicated daily pill taking: “You gotta find a place to take medicine cause they don't want everybody in their business. From what I hear, everybody's nosy in the shelter, everybody's in your business” (27, same-gender loving). Men also described how fluctuations in daily routines—due to factors such as housing and job instability—would complicate maintaining what was already a strict daily regimen.
Discussion
This ethnographic study explored how BMSM think about, understand, and engage with PrEP. Even men who had heard of PrEP reported an incomplete understanding of PrEP's efficacy, the potential side-effects, and the frequency of use. Also, the view that PrEP was a useful tool for others, but not for oneself, cut across, and was informed by, all aspects of men's lives (e.g., their personal attitudes, relationships, community norms, and structural stigma).
Personal level
Similar to previous research examining facilitators and barriers to PrEP use, 15,23 –26 two primary factors influenced study participants' PrEP desires: perceived efficacy and side-effects. 25 Concerns about effectiveness suggest that men see PrEP as a standalone prevention method rather than as something to pair with condoms. A PrEP messaging study found uncertainty among men about how to interpret numerical estimates and whether clinical trial results would predict personal effectiveness; 27 men in this study expressed confusion about what 90% effectiveness meant for their own HIV risk. Study participants also felt conflicted about healthy people taking medication, especially one with side-effects. Particularly since other means of HIV prevention lack side-effects, men reported wariness about whether the benefits outweighed the risks. This echoes other research with HIV-negative MSM, which found potential side-effects (particularly long-term ones) to be the biggest barrier to uptake. 28 –30 Moreover, potentially reflecting how medical mistrust might amplify concerns about side-effects, MSM of color were more likely than white MSM to state that they would avoid PrEP because of side-effects. 31 Men were also loathe to put something in their bodies that could not be taken out again; this suggests that injectable PrEP, which has been discussed as a way of solving PrEP's adherence challenges, may also create new barriers to uptake.
Interpersonal level
Respondents worried about declines in condom use for men on PrEP and those having sex with men on PrEP. Participants emphasized that the PrEP uptake would allow them to avoid condoms and that regular condom use would eliminate the need for PrEP; the few respondents who described joint PrEP and condom use as realistic were community stakeholders. Previous studies reported mixed sentiments about risk disinhibition; 4 of 10 studies in a review 12 reported that risk disinhibition would occur, 24,25,32,33 whereas 6 did not. 15,34 –38 A study of MSM in serodiscordant relationships showed that the use of PrEP might reduce condom use and increase risk behaviors, and it found that desire for condomless sex was a major reason to take PrEP. 34 Other studies showed that men would forgo condoms if PrEP had an efficacy of more than 50%. 12 Men within this study had conflicting narratives about PrEP and condom use. Men described how risk disinhibition among partners and sexual networks would increase their risk for HIV, particularly since PrEP is neither 100% effective, nor does it protect against other STIs. However, others, particularly community stakeholders, felt that PrEP's lack of STI protection should be highlighted as a rationale for continued condom use.
Community level
Two primary factors impacted whether men would seek PrEP: medical mistrust and the framing of social risk (i.e., believing that only others should take PrEP). Although research has examined the intersection of medical mistrust, healthcare seeking, and race, little work exists about how mistrust of the pharmaceutical industry (i.e., of biomedicine writ large) might limit PrEP uptake. Medical mistrust research primarily focuses on patient–provider relationships, with one study finding race-based medical mistrust as a barrier to PrEP use; 18 another reported that “medical mistrust and perceived discrimination create barriers for sexual behavior disclosure to clinicians,” which study authors believed could impede PrEP access. 39
The men saw PrEP messaging as confusing, because although BMSM were targeted by many campaigns, they did not see themselves as at risk and in need of PrEP. Other studies report such confusion and showed that perceived HIV risk was associated with PrEP uptake. 40 Willingness to use PrEP is associated with a higher perceived risk of HIV acquisition, 37,41 which supports why the men we spoke with who did not see themselves as at risk felt that PrEP was something that only other people should engage with. This suggests that communications strategies must help men imagine themselves as PrEP users, in addition to presenting technical dimensions of PrEP, such as its effectiveness. This social framing of risk also suggests the need to examine the stigma associated with HIV and sex between men. Addressing risk denial through stigma reduction may help counteract how some men actively resist seeing their behaviors as making them vulnerable to HIV and thus in need of PrEP.
Structural level
The men we spoke with reported that PrEP use might also cause stigma from friends, family, and partners. PrEP uptake involved substantial social risk, including revelations about having sex with men, which many men chose to not disclose to their families and friends. The few studies that have addressed the intersection of PrEP and stigma focused almost exclusively on interpersonal-level factors (e.g., relationships) and reported that men see PrEP use as a marker of infidelity 30 and fear disclosure of PrEP use, in part due to HIV-related stigma. 42,43 In contrast, the men in this research described stigma on a structural level and focused on how it constrained their ability to accept themselves as BMSM with other men, and to thus recognize the need to engage in HIV prevention.
Structural barriers to PrEP use—felt acutely in a sample in which the majority of men lacked both health insurance and a primary care provider—included unstable housing and lack of access to medical care and HIV prevention services. The iPrEx trial showed that PrEP's effectiveness varies according to adherence, suggesting that PrEP's success at both the individual and population level will depend on ensuring BMSM's access to HIV prevention services (e.g., condoms, STI treatment, HIV testing, and counseling) and primary care 1 —which are not always available at either low or no cost to BMSM. In addition, the majority of study participants lacked access to a social worker or case manager who could facilitate access to the housing and employment that would provide the stability necessary to begin taking PrEP or to the medical services in which men might actually receive PrEP. Strategies focused on enrolling BMSM in primary care, for example, by using Affordable Care Act health navigators, could also help lay the groundwork for increased PrEP uptake. Lastly, we must ensure that Medicaid formularies across the United States cover PrEP-related care and treatment.
Limitations
Although participants varied by age, sexual identity, and insurance status, they were primarily low SES. Also, New York is unique in terms of available HIV-related services. However, this suggests that the barriers to PrEP would only be more substantial across the United States, since many other states have either not added PrEP to their Medicaid formularies or have less generous funding for Medicaid or fewer BMSM-oriented prevention programs. Though we described PrEP in the interview guide, and answered any resulting questions, participants did not have an extended period to think through all of PrEP's benefits and limitations, which may have limited their capacity to comment.
In conclusion, findings demonstrate that PrEP will only become a successful intervention if all levels of the ecological framework are addressed. Specifically, our findings show that PrEP-related communications strategies should be as detailed as possible about efficacy and explicitly address tensions between PrEP and condom use. Community- and structural-level factors such as medical mistrust and societal stigma can impact PrEP use; potential intervention approaches could include a rights-based, anti-homophobia, approach to mitigate HIV-related stigma as well as community engagement around HIV prevention. To realize the promise of PrEP, future research needs to examine how biomedical prevention can be integrated into the lives of BMSM across all levels of the ecological framework.
Footnotes
Acknowledgments
This research was supported by a grant from the National Institute of Mental Health (R01 MH098723, PIs: Paul Colson and J.S.H.). Additional support came from the Center for the Study of Culture, Politics and Health and the Society, Psychology, and Health Research Lab (SPHERE). Dr. M.M.P. is supported by an NIMH training grant (T32-MH19139 Behavioral Sciences Research in HIV Infection; PI: Theodorus G.M. Sandfort, PhD) located within The HIV Center for Clinical and Behavioral Studies (P30-MH43520; PI: Robert Remien, PhD). The principal contributions of each of the authors of this article are as follows: M.M.P. as primary author led the study analysis and interpretation of the data and contributed significantly to the drafting and revision of the article; C.M.P. contributed significantly to the analysis and interpretation of the data and revisions of the article; R.G.P. and P.A.W. contributed to the study design and revision of the article; J.G. conducted the majority of data collection and contributed to the revisions of the article; and J.S.H. led the study design and contributed to the analysis, interpretation of data, and revisions of the article.
Funding: This study was funded by R01 MH098723.
Author Disclosure Statement
No conflicting financial interests exist.