
Abstract
Transgender women are overrepresented in the Caribbean HIV epidemic. The study objective was to examine correlates of HIV infection and HIV testing among transgender women in Jamaica. We implemented a cross-sectional survey with transgender women in Kingston and Ocho Rios, Jamaica. We conducted multivariable logistic regression to identify factors associated with HIV testing and HIV infection. Among 137 transgender women [mean age 24.0; standard deviation (SD) 5.5], three-quarters (n = 103, 75.7%) had received an HIV test. Of these, one-quarter (n = 26, 25.2%) were HIV positive. In multivariable analyses, HIV testing was associated with: perceived HIV risk [adjusted odds ratio (AOR) 2.42, confidence interval (CI) 1.36–4.28], depression (AOR 1.34, CI 1.01–1.77), forced sex (AOR 3.83, CI 1.42–10.35), physical abuse (AOR 4.11, CI 1.44–11.72), perceived transgender stigma (AOR 1.23, 1.06–1.42), having a healthcare provider (AOR 5.89, CI 1.46–23.77), and lower HIV-related stigma (AOR 0.96, CI 0.92–0.99), incarceration (AOR 0.28, CI 0.10–0.78), and drug use (AOR 0.74, CI 0.58–0.95). HIV infection was associated with the following: homelessness (AOR 5.94, CI 1.27–27.74), perceived HIV risk (AOR 1.67, CI 1.02–2.72), depression (AOR 1.39, CI 1.06–1.82), STI history (AOR 56.79, CI 5.12–630.33), perceived (AOR 1.26, CI 1.06–1.51) and enacted (AOR 1.16, CI 1.04–1.29) transgender stigma, forced sex (AOR 4.14, CI 1.49–11.51), physical abuse (AOR 3.75, CI 1.39–10.12), and lower self-rated health (AOR 0.55, CI 0.30–0.98) and social support (AOR 0.79, CI 0.64–0.97). Transgender women in Jamaica experience high HIV infection rates and suboptimal HIV testing. Combination HIV prevention approaches should address transgender women's social and structural vulnerabilities.
Introduction
H
Jamaica is one of several Caribbean countries that has established a comprehensive response to the HIV epidemic, 6 resulting in a substantially reduced HIV incidence and a current HIV prevalence of 1.7% (95% CI 1.4–2.0) among the adult general population. 7 Yet the criminalization of “homosexuality” in Jamaica may contribute to elevated HIV infection rates among sexual and gender minorities (SGM). For example, the estimated HIV prevalence among men who have sex with men (MSM) in Jamaica is between 28% and 32%, among the highest in the Caribbean. 8,9 Scant research has examined HIV prevalence among transgender women in Jamaica, who face similar experiences of stigma and discrimination as MSM. Figuero et al.'s 9 study with MSM (n = 449) in Jamaica included 17 transgender women with reported HIV infection rates of 52.9%. We located no studies focused on assessing HIV prevalence, correlates of HIV testing, or correlates of HIV infection among transgender women in Jamaica.
Social and structural drivers that elevate transgender women HIV exposure include the criminalization of homosexuality, violence, stigma, and discrimination. Criminalization of SGM limits access to the HIV prevention and care continuum, 10 from HIV testing and diagnosis to viral suppression. 10 –12 Community-based organizations report pervasive violence toward SGM populations from both within their families and in the broader community. 13,14 Globally transgender women experience higher rates of violence and incarceration than nontransgender women. 15
SGM in Caribbean countries experience stigma and discrimination, family rejection, and a lack of human rights protection in employment, education systems, and the State. 16 These factors contribute to economic insecurity, including poverty and homelessness, which elevate HIV vulnerability 16,17 and decrease access to HIV testing. 18 Economic insecurity plays a role in the high rates of sex work among transgender populations, particularly in Caribbean and Latin American countries, with upward of 60% of samples reporting sex work involvement. 15,19 HIV-related stigma also presents a formidable barrier to HIV testing uptake in Jamaica. In a study of incarcerated men in Jamaica (n = 298), HIV-related stigma was associated with decreased likelihood of ever receiving an HIV test. 20 In a qualitative study with health and social service providers, PLHIV and SGM reported that both HIV-related and sexual stigma reduced uptake of, and access to, HIV testing, treatment, and care services. 21 The lack of confidentiality about sexuality and HIV in healthcare facilities leads to distrust that reduces health services utilization. 22
Understanding factors associated with HIV infection and HIV testing among transgender women in the Jamaican context is critical to enhance access to the HIV care cascade. HIV testing is the first step in the HIV care cascade, facilitating diagnosis and linkage to care, initiation of antiretroviral treatment, and viral suppression—which may optimize the health of transgender women as well as prevent HIV transmission. 11
Study objectives
The study objective was to enhance knowledge of correlates of HIV infection and HIV testing uptake among transgender women in Jamaica. We aimed to (1) determine HIV prevalence and the proportion of participants ever tested for HIV and (2) determine correlates of HIV infection and ever having received an HIV test.
Methods
Sampling and data collection
In collaboration with Jamaica AIDS Support for Life, a national AIDS Service Organization, we conducted a cross-sectional survey with transgender women in Kingston and Ocho Rios, Jamaica, as well as from surrounding areas of these cities between March 2015 and October 2015. Participants were eligible to complete the survey if they identified as transgender women over 18 years, currently residing in Jamaica.
We utilized purposive, nonrandom sampling methods to access this highly marginalized population. There were no print materials (e.g., flyers, posters) due to the lack of legal protection among transgender women in Jamaica. We recruited and trained seven peer research assistants (PRAs) across study sites who self-identified as sexual or gender minorities (lesbian, gay, bisexual, transgender). We used snowball sampling methods with PRAs and participants to recruit transgender women participants 23 ; snowball sampling methods facilitated reaching hidden populations, 24,25 such as transgender people. 26 PRAs in each venue were involved in conducting HIV outreach at Jamaica AIDS Support for Life, including a mobile testing service that provided HIV testing and access to HIV prevention materials (e.g., condoms, lubricant). The PRAs who were conducting HIV outreach shared study information with potential participants and also shared the study information with their social networks. Each participant of the study was also provided the opportunity to invite additional participants through sharing up to five study coupons with persons in their social networks, and participants received $500 Jamaican dollars (∼$4 USD) for each participant they recruited up to a maximum of five participants. PRA recorded the identification number for each coupon used for recruitment purposes. This process allowed for voluntary HIV testing of participants and matching HIV testing uptake and HIV test results to each participant survey ID.
The survey was interviewer administered on tablets in a location of the participant's choice (e.g., home, park, Jamaica AIDS Support for Life). The survey took 30 min to complete and participants received a $1000 Jamaican dollar (∼$8 USD) honorarium for their time. Participants were offered a $500 Jamaican dollar (∼$4 USD) phone card for completing voluntary HIV testing and post-test counseling at Jamaica AIDS Support for Life upon presentation of the coupon with their unique participant identification (ID) number. Tests were offered to all study participants, regardless of HIV status or self-reported past HIV testing. Tests were done by a trained nurse at Jamaica AIDS Support for Life using an immunochromatographic HIV rapid test kit (Alere Determine HIV-1/2). If the rapid HIV test result was positive, a blood sample was taken and sent to the National Laboratory to perform ELISA testing to confirm results. Research ethics approval was granted from the University of Toronto and the University of the West Indies Mona Campus.
Measures
Ever HIV tested and HIV status
HIV test ever was measured during survey data collection with the dichotomous question “I have had an HIV test in my lifetime.” We also included participants who presented their study coupon to receive a rapid HIV test at Jamaica AIDS Support for Life as having ever received an HIV test. If participants responded that they had received an HIV test, they were asked to self-report their HIV status. HIV status was measured by combining self-reported HIV status collected on the survey and HIV test results from participants who chose to complete HIV testing as part of this study. HIV serostatus was dichotomized to HIV positive and HIV negative. We assessed differences in sociodemographic and all study variables among persons reporting an HIV-positive status by self-report or in this study's laboratory test.
Sociodemographic factors
Sociodemographic variables included age and monthly income in Jamaican dollars, measured continuously, and city of residence (Kingston, Ochos Rios, with the option to list other places of residence), education level (less than high school, completed high school, attended some college, and completed college or higher), employment status (employed or self-employed full time, employed or self-employed part time, student, receiving assistance, no source of income), relationship status (married or living together, dating–not living together, casual dating, no current partner, and multiple partners/polyamorous), and housing status (own house or apartment, family, other people's house or apartment, living outside) measured categorically.
Intrapersonal factors
Perceived HIV risk was assessed using a Likert-scale question “How much do you think you are at risk for HIV infection?” with the options of no risk, low risk, medium risk, or high risk. We used the two-item Patient Health Questionnaire-2 (PHQ-2) to screen for depression symptoms over the last 2 weeks 27 (Cronbach's α = 0.67 scale range 0–8). A higher score of PHQ-2 reflects increased depression symptoms. Self-rated health was assessed using the World Health Organization's single global self-rated health question [On a scale of 1 (poor) to 4 (excellent), how would you rate your overall health?] 28 measured on a 4-point Likert scale with a higher response indicating a higher self-rated health. We assessed substance use with the following question: “Have you drank alcohol or used drugs in the last 3 months (Yes/No)?” Participants were asked about drug use with the following question: “On a scale of 1 (never) to 8 (every day), how often have you used OTHER DRUGS (not alcohol) in the last 3 months?” Lifetime sexually transmitted infections history was measured using the following two questions: (1) I have had a sexually transmitted infections (STI) test (not including HIV) in my lifetime; and if yes, (2) What was the STI test result? Sex work involvement was measured by asking the following question: “In the last year have you ever had sex (oral, vaginal, or anal) in exchange for (please check all that apply) the following: (1) a place to stay, food, or transportation; (2) money; (3) drugs or alcohol; and (4) none of the above.” If the answer was affirmative for options (1) through (3), the response was coded as sex work involvement.
Interpersonal/social factors
We assessed factors related to experiences of forced sex: “In your life have you ever experienced forced sex (e.g., rape, sexual assault)?” and physical abuse. “In your life have you ever experienced physical abuse? (Abuse is any act to hurt you physically).” We measured social support using a brief social support scale 29 previously assessed for validity in a Caribbean context (Puerto Rico). The social support measure included two subscales: the need for social support (Cronbach's α = 0.83, range 5–35) and satisfaction with the quality of social support (Cronbach's α = 0.86, range 2–10). 29 We conducted confirmatory factor analysis (CFA) to assess the factor structure of the two subscales in the social support measure (TLI = 0.97, CFI = 0.99, RMSEA = 0.08, p < 0.05). To assess practices associated with increased risk of HIV acquisition, participants were asked how often they get drunk or high while having sex, measured on a four-point Likert Scale [1 (never) to 4 (always)], and lifetime number of sexual partners measured continuously.
Structural and healthcare access factors
HIV-related stigma was measured using Steward et al.'s 10-item perceived (also referred to as felt or felt-normative) stigma subscale, 30 with a higher score indicating a higher level of perceived HIV-related stigma (Cronbach's α = 0.89, range 0–100). Perceived stigma refers to awareness of negative attitudes, beliefs, and treatment toward a marginalized group, 31 for example, people living with HIV. This subscale was validated with HIV-negative MSM and transgender women in LMIC. 32,33 Items were measured on a 10-point Likert scale from 1 (none) to 10 (most people) (e.g., “In your community how many people think that HIV positive people have brought shame on their families?”).
We utilized an adapted version of Diaz et al.'s 34 Homophobia Scale to measure enacted (Cronbach's α = 0.77, range 7–28) and perceived stigma (Cronbach's α = 0.61, range 5–20) toward transgender persons. The scale was adapted to replace each item “because of your homosexuality” to “because you are transgender.” Enacted stigma refers to discriminatory acts, including violence, harassment, and mistreatment. 31 The perceived transgender stigma scale includes items such as “How often have you heard that transgender people are not normal?” and the enacted transgender stigma scale includes items such as “How often have you been hit or beaten up for being transgender?” We assessed the factor structure of the two-dimensional (perceived, enacted) transgender stigma scale using CFA (TLI = 0.91, CFI = 0.93, RMSEA = 0.11, p < 0.05).
Having a healthcare provider was measured dichotomously with the question “Do you have a regular healthcare provider?” A history of incarceration for being transgender was measured dichotomously with the question “Have you ever been in jail for being transgender?” Housing security was measured by asking, “In the past month, where have you usually slept? (a) In my own house or apartment; (b) in other people's house or apartment; (c) outside (homeless).”
Data analysis
We conducted descriptive analyses for sociodemographic variables (e.g., age, income) to determine frequencies and proportions for categorical variables, and means and standard deviations (SDs) for continuous variables. Descriptive analyses included all participants with available data. We conducted bivariate logistic regression followed by multivariate logistic regression controlling for factors correlated at p < 0.05 (age and monthly income) for each outcome (ever HIV tested and HIV status) separately. Multivariate logistic regression allows for the determination of appropriate estimates of the adjusted risk ratio for having ever received an HIV test and HIV serostatus among transgender women in Jamaica. We report the unadjusted and adjusted odds ratios (AORs) and 95% CIs, highlighting those significant at the 0.05 level. Missing responses were excluded from the analyses; the number of complete responses are reported for each variable. All statistical analyses were performed using STATA (version 12.0, College Station, TX).
Results
Participant characteristics
Table 1 reports participant sociodemographic characteristics, HIV testing and prevalence outcomes, and intra/interpersonal and structural factors (n = 137). The mean age was 24.0 years (SD 4.5). Two-thirds of the sample (67.2%) lived in the Kingston area. Participants reported an average monthly income of $225.5 USD (SD 337.9). Less than one-third of participants (n = 41, 30.4%) reported having enough money to afford a place to live. Less than one-third of participants (n = 42, 30.7%) had a regular healthcare provider. Three-quarters (n = 103, 75.7%) of participants had ever received an HIV test. One-quarter (n = 26, 25.24%) of those tested reported being HIV positive: 15 participants were HIV positive from our study's laboratory test and 11 self-reported being HIV positive. Bivariate analysis (T-test, chi-square, or ANOVA) revealed that there were no significant differences in sociodemographic or other variables between participants who self-reported being HIV positive and those who received an HIV-positive result in this study's laboratory test.
Percentages calculated from nonmissing responses for each variable.
SD, standard deviation.
Univariate and multivariate modeling of HIV testing among transgender women
In univariate analyses (Table 2), perceived poverty, living in Ocho Rios compared to Kingston, perceived HIV risk, depression, forced sex history, physical abuse history, perceived transgender stigma, and having a healthcare provider were associated with increased odds of ever having received an HIV test. Having multiple partners/polyamoury compared to being married, drug use, getting drunk or high when having sex, and HIV-related stigma were associated with decreased odds of ever having received an HIV test.
Adjusted for age and monthly income.
In multivariate analyses (Table 2), HIV testing was associated with intrapersonal (perceived HIV risk [AOR 2.42, CI 1.36–4.28], drug use [AOR 0.74, CI 0.58–0.95], and depression [AOR 1.34, CI 1.01–1.77]), interpersonal/social (getting drunk or high when having sex [AOR 0.49, CI 0.25–0.95], forced sex history [AOR 3.83, CI 1.42–10.35], and physical abuse history [AOR 4.11, CI 1.44–11.72]), and structural (perceived transgender stigma [AOR 1.23, 1.06–1.42], HIV-related stigma [AOR 0.96, CI 0.92–0.99], incarceration history for being transgender [AOR 0.28, CI 0.10–0.78], and having a healthcare provider [AOR 5.89, CI 1.46–23.77]) factors. The lifetime STI history result is omitted because all participants with a lifetime STI history had received an HIV test. With a 1 U increase in HIV-related stigma, the likelihood of HIV testing decreased by 4%. Figure 1 portrays that if a participant scored 25 on the HIV-related stigma scale, the predicted probability of HIV testing was 97.2%, whereas if a participant scored 100 on the HIV-related stigma scale, the predicted probability of HIV testing was 58.4%.
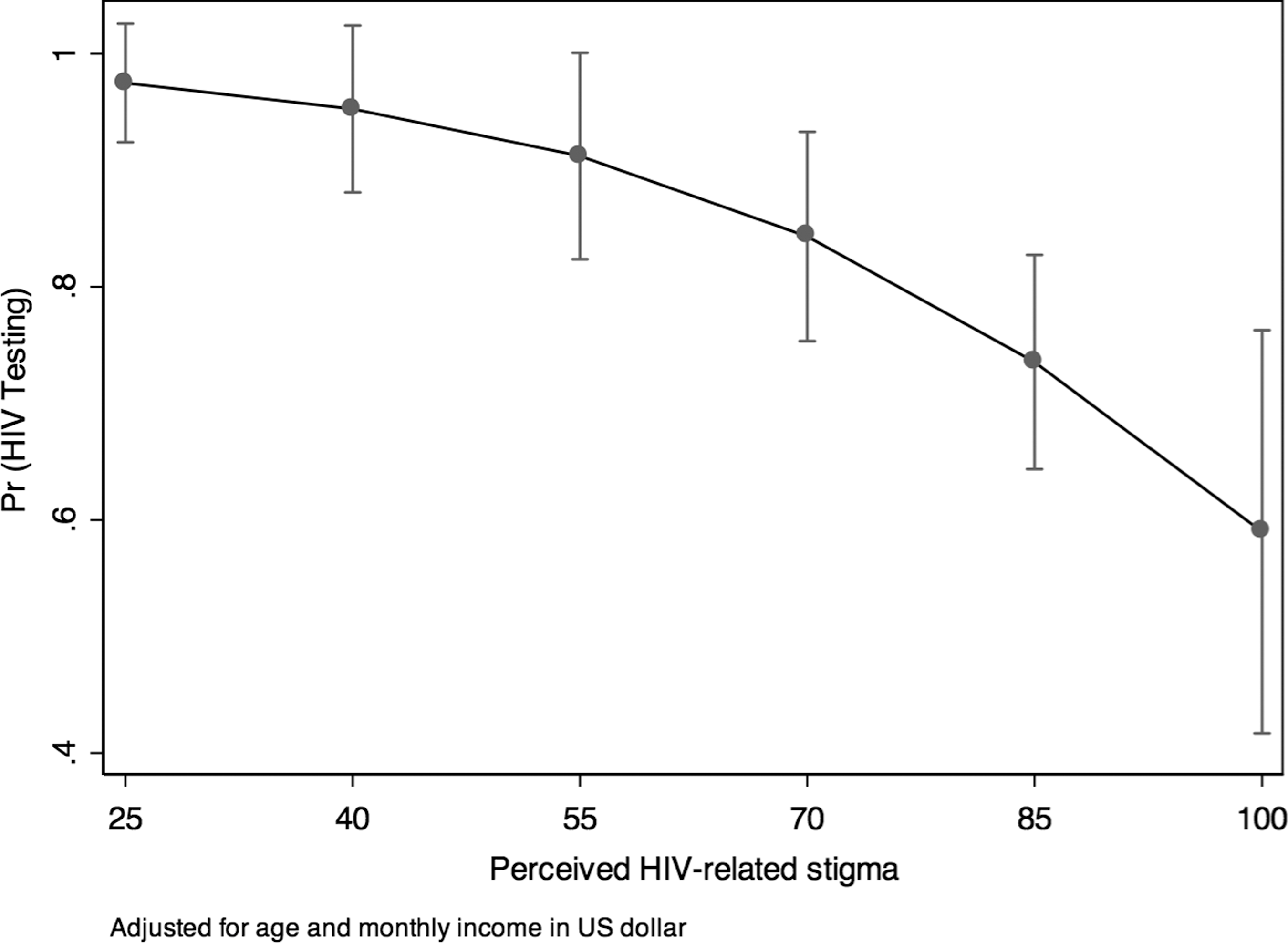
Predicted probability of HIV-related stigma on HIV testing with 95% CI. CI, confidence interval.
Univariate and multivariate modeling of HIV status among transgender women
In univariate analyses, perceived poverty, perceived HIV risk, depression, need for social support, forced sex history, physical abuse history, perceived transgender stigma, enacted transgender stigma, lower self-rated health, and homelessness were associated with increased odds of being HIV positive. Being employed and having higher quality of social support were associated with decreased odds of being HIV positive.
In multivariable analyses (Table 2), being HIV positive was associated with intrapersonal (perceived HIV risk [AOR 1.67, CI 1.02–2.72], depression [AOR 1.39, CI 1.06–1.82], self-rated health [AOR 0.55, CI 0.30–0.98], and lifetime STI history [AOR 56.79, CI 5.12–630.33]), interpersonal/social (need for social support [AOR 1.09, CI 1.01–1.18], quality of social support [AOR 0.79, CI 0.64–0.97], having forced sex history [AOR 4.14, CI 1.49–11.51], and physical abuse history [AOR 3.75, CI 1.39–10.12]), and structural (perceived transgender stigma [AOR 1.26, CI 1.06–1.51], enacted transgender stigma [AOR 1.16, CI 1.04–1.29], and homelessness [AOR 5.94, CI 1.27–27.74]) factors.
Perceived and enacted transgender stigma were higher among HIV-positive participants. With a 1 U increase in the perceived transgender stigma score, the likelihood of being HIV positive increased by 26.5%. As shown in Fig. 2, the predicted probability of being HIV positive if a participant scored 5 on the perceived transgender stigma scale was 2.2%, whereas the probability was 27.9% if the participant scored 20. With a 1 U increase in the score on the enacted transgender stigma scale, the likelihood of being HIV positive increased by 15.7%. Figure 3 depicts that the predicted probability of being HIV positive if a participant scored 7 on the enacted transgender stigma scale was 6.2%, whereas the probability was 54.8% with a score of 30.
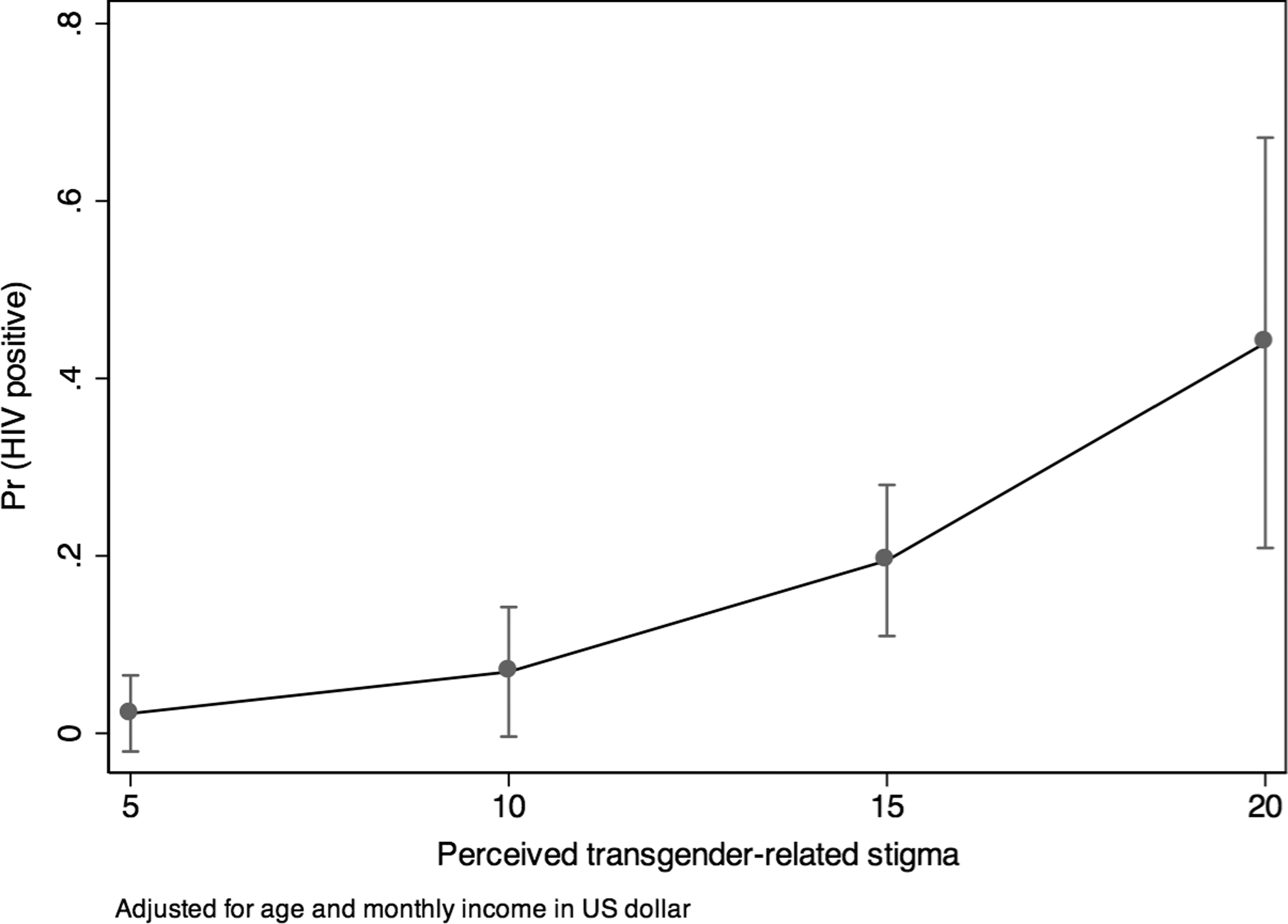
Predicted probability of perceived transgender stigma on HIV status with 95% CI.
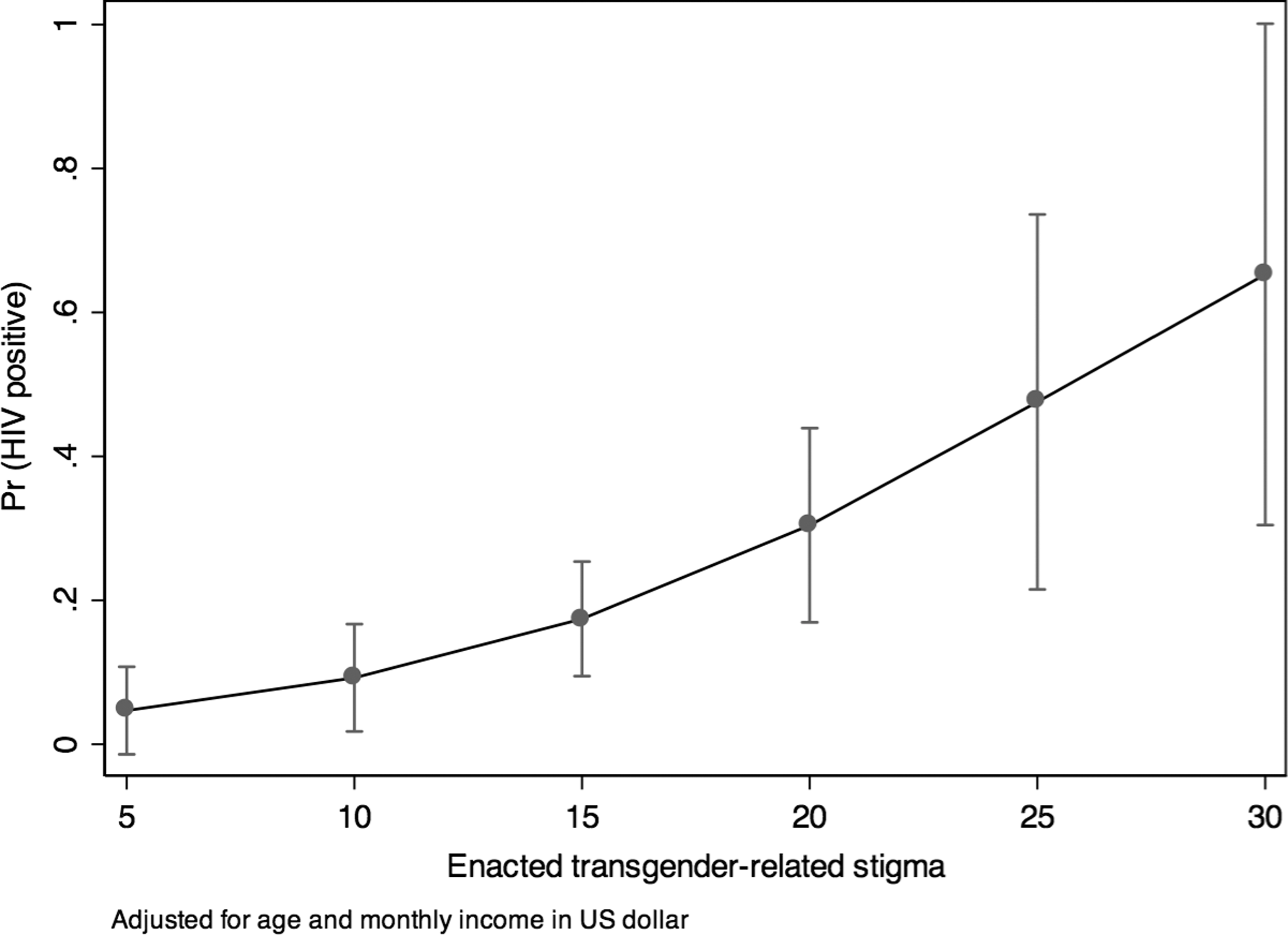
Predicted probability of enacted transgender stigma on HIV status with 95% CI.
Discussion
The high HIV prevalence in this study highlights transgender women in Jamaica as a key population to involve in the HIV prevention and care continuum. Lifetime history of other STIs was highly associated with being HIV positive, underscoring the need to include STI testing and prevention as part of the HIV prevention and care continuum in the Jamaican context. One-quarter of participants were never tested for HIV; with a 25% rate of seropositivity, this rate of testing is concerning as it is likely that a proportion of our sample are living with HIV undiagnosed, limiting their access to early treatment, care, and support. Importantly, our findings suggest that participants who engaged in practices that elevate the risk of HIV exposure (drug use, getting drunk, or high when having sex) were less likely to have received an HIV test. Tailored educational interventions to increase perceived HIV risk among highly marginalized populations (e.g., transgender women who use drugs) may promote HIV testing uptake. Strategies are required to increase accountability, sensitivity, and privacy in HIV testing and care services.
Our study highlights complex, multi-level factors associated with HIV testing and HIV infection that reflect the social ecological model. Social ecological perspectives situate HIV risk in larger social and structural contexts, including intrapersonal (e.g., mental health), interpersonal/social (e.g., social support), and structural (e.g., healthcare access, stigma) factors. 35 HIV-related stigma was a barrier to HIV testing, corroborating qualitative work in Jamaica 21 and quantitative work in other contexts. 33,36 –38
Transgender stigma was higher among participants who had ever received an HIV test in comparison with those never tested and among HIV-positive participants in comparison with HIV-negative participants. It is plausible that transgender women encounter transgender stigma upon accessing HIV testing and care services. For example, a recent study in Jamaica and the Bahamas with 332 healthcare and social service providers reported stigmatizing attitudes, most strongly in relation to MSM living with HIV. 39 Prior research in Jamaica has highlighted healthcare worker resistance to working with sexual minorities and PLHIV. 39 –41 It is also possible that transgender stigma could be a distal HIV risk factor and elevate HIV infection risks—longitudinal studies are warranted to better understand the associations between HIV-positive serostatus and transgender stigma. There is a growing body of literature that suggests HIV self-testing, administered in a location of an individual's choosing, is acceptable to transgender women and may address concerns with privacy, confidentiality, and stigma (HIV related, transgender) often encountered by transgender women in the context of clinic-based HIV testing. 42 –44 However, in the absence of structural interventions to address stigma in healthcare settings, transgender women living with HIV may continue to experience barriers accessing the HIV care continuum. 42
HIV-positive participants were sixfold more likely to be homeless, and a history of incarceration was associated with substantially (>70%) reduced odds of ever receiving an HIV test. Forced sex and physical violence were associated with both increased odds of being HIV positive and having received an HIV test. Number of sexual partners was only marginally associated (p = 0.041) with being HIV positive. It is plausible that HIV infection occurred early in sexual debut; sexual violence may also have increased HIV exposure. Addressing transgender women's survival needs, and reducing violence targeting transgender women, in Jamaica may be key to reducing vulnerability to HIV infection and engaging them in the HIV prevention and care continuum.
There are a few limitations inherent in our study design. The nonrandom sampling method, while necessary in accessing such a hidden and vulnerable population, limits generalizability of findings to other transgender women in Jamaica. The cross-sectional study design precludes understanding causality and necessitates a cautious interpretation of our findings. Data collected were self-reported and is therefore subject to recall bias and social desirability bias. While we found having multiple partners/polyamoury was associated with HIV testing uptake, future studies could examine multiple partners/polyamoury as a distinct category rather than a relationship status, as persons of various relationship statuses can have multiple partners. We found an overall HIV prevalence of 25% through combining self-reported HIV status with HIV-positive laboratory test results in our study. However, HIV testing was voluntary and only 22% of participants chose to receive an HIV test in this study. The low rate of testing uptake could be related to high rates of baseline seropositivity; it is also possible that participants who had ever received an HIV test did not feel the need to receive another. Our findings could therefore underreport HIV infection rates among this sample of transgender women.
Despite these limitations, this was among the first studies to assess HIV status and testing rates among transgender women in Jamaica, a highly vulnerable population among whom we identified extremely high HIV prevalence. Combination HIV prevention approaches may be crucial for Jamaican transgender women given the many social-structural vulnerabilities identified; these might include the following: increased access to voluntary HIV testing and counseling; psychosocial support for depression and substance use; gender-based violence prevention; HIV and transgender stigma reduction campaigns; access to survival needs, in particular employment and housing; and legal protection from discrimination. Future research and interventions could address the syndemics 45,46 of violence, economic insecurity, and mental health challenges that elevate HIV vulnerability among this population. Addressing social ecological contexts of HIV risk is necessary to advance HIV prevention among transgender women in Jamaica.
Footnotes
Acknowledgments
We would like to thank all the participants, peer research assistants, and collaborators: Jamaica AIDS Support for Life; JFLAG: Jamaica Forum for Lesbians, All-Sexuals and Gays; Caribbean Vulnerable Communities (CVC); Grata Foundation; QCJ: Quality of Citizenship Jamaica; Ashe; Colour Pink Group; Aphrodite's Pride; and the University of the West Indies, Mona Campus. This research was funded by the Canadian Institutes of Health Research Operating Grant 0000303157; Fund: 495419, Competition 201209.
Author Disclosure Statement
No conflicting financial interests exist.