
Abstract
Healthcare empowerment (HCE) is patient controlled and includes the process and state of being engaged, informed, collaborative, committed, and tolerant of uncertainty. Understanding psychosocial factors that impact HCE for persons living with HIV is critical for their treatment and care. A sample of 1494 male and female participants living with HIV in the United States with a mean age of 45.6 (standard deviation = 11.4) completed a one-time online survey about their demographic characteristics, social support, healthcare provider relationship, HIV treatment knowledge, perceived HIV-related stigma, lifetime trauma, depressive symptoms, HCE, and antiretroviral therapy (ART) adherence. A path analysis was conducted using structural equation modeling software to fit a theory-based model of HCE. Results included statistically significant direct pathways between depressive symptoms, healthcare provider relationship, lifetime trauma, and ART adherence, as well as between healthcare provider relationship, HIV treatment knowledge, and HCE. Specifically, ART adherence was positively linked to healthcare provider relationship and negatively linked to depressive symptoms and lifetime trauma. In addition, healthcare provider relationship and HIV treatment knowledge were positively associated with HCE. The indirect effects of healthcare provider relationship and HIV treatment knowledge on adherence through HCE were also significant. In particular, ART adherence was indirectly and positively affected by healthcare provider relationship and HIV treatment knowledge through HCE. Multi-level interventions are urgently needed to address the effects of these psychosocial factors on ART adherence.
Introduction
A
Informed by several theoretical frameworks, including Social Action Theory, 7 Stress and Coping Theory, 8 Social Problem Solving Theory, 9 and multiple derivations of the Health Belief Model, 10,11 the Healthcare Empowerment (HCE) model as proposed by Johnson (2011) is a promising structure for understanding and intervening on how PLWH perceive their participation in their healthcare in the United States. 12 HCE has been defined as the process and state of being in medical treatment that encompasses the following five facets of participation in healthcare: (1) Engaged (i.e., active participation in one's own healthcare), (2) Informed (i.e., understands own illness or condition, is aware of treatment options and the relative risks and benefits, and has a good understanding of the healthcare system), (3) Collaborative (i.e., involvement in clinical decision-making and perceives a partnership with healthcare providers), (4) Committed (i.e., maintains engagement and collaboration with healthcare providers and facilitates adherence to collaboratively derived treatment plans), and (5) Tolerant of Uncertainty (i.e., balancing of emotional needs and a rational approach to decision-making based on probabilities and relative risks). According to this model, the level of HCE in an individual dealing with a chronic medical condition or illness such as HIV in the United States is determined by a dynamic interplay of personal resources (e.g., social support, healthcare provider relationship, and HIV treatment knowledge), contextual/environmental factors (e.g., HIV-related stigma and trauma), and intrapersonal factors (e.g., depression). 12,13
Preliminary support for the HCE model in understanding patient engagement in HIV medical care conducted in the United States was reported by Johnson et al. (2012). 13 Cross-sectional data combined from two ongoing clinical trials of social and behavioral aspects of HIV treatment were used in their study to assess antecedents and clinical outcomes of HCE in the context of HIV treatment. Antecedents included cultural/social/environmental factors (e.g., demographics and HIV-related stigma), personal resources (e.g., social problem-solving, treatment knowledge and beliefs, treatment decision-making, shared decision-making, decisional balance, assertive communication, trust in providers, personal knowledge by provider, and social support), and intrapersonal factors (e.g., depressive symptoms, positive/negative affect, and perceived stress). Clinical outcomes included primary care appointment attendance, ART use, adherence self-efficacy, medication adherence, CD4+ cell count, and HIV viral load. The first trial was a 12-month cohort study of 254 male couples, in which one or both partners were living with HIV and taking HIV medications. The second was a 6-month randomized controlled trial of 148 PLWH not on ART at baseline despite meeting HIV treatment guidelines on CD4+ cell count cutoff for initiation of ART (i.e., ≤500 cells/mm3). In single-equation regression models, significant positive associations were found between HCE and recent primary care visit, greater treatment adherence self-efficacy, and higher adherence to ART. In addition, higher beliefs in the necessity of treatment and positive provider relationships were found among the antecedents of HCE. However, significant associations between HCE and HIV viral load and CD4+ cell count were not observed.
The interplay of these various components of the HCE model has not been previously tested simultaneously using path analysis conducted via structural equation modeling (SEM) with simultaneous estimation of the indirect effects of antecedents on outcomes through HCE. The major benefit of using SEM to further evaluate the HCE model is that there are not widely and easily applied alternative methods for modeling simultaneous multivariate relationships, or for estimating point and/or interval indirect effects in the context of simultaneous equations. 14
The purpose of our study was to conduct a secondary data analysis to examine the interrelationships of psychosocial factors that constitute the HCE model using measures available in an existing data set to understand their association with ART adherence among PLWH in the United States. Although some of the measures used (e.g., social support and healthcare provider relationship) were single questions or items that may not fully capture the complexity of the factors under investigation, it has been argued by some measurement developers that single-item measures demonstrate equally high predictive validity as multi-item scales. 15,16 In addition to some of the antecedents used in the study by Johnson et al. described earlier, which were available in our data set, in the current study, we included trauma as an additional contextual and environmental factor as it has been identified in the empirical literature as impacting ART adherence among PLWH. 17 For the clinical outcomes, we focus specifically on ART adherence as this is a critical determinant of long-term physical and mental health outcomes in PLWH. 3 Following the theoretical literature on HCE, 12 we hypothesized that antecedent factors such as personal resources, contextual and environmental factors, and intrapersonal factors would directly impact ART adherence while also indirectly affecting adherence through HCE. The conceptual model, derived from earlier work conducted by Johnson et al., 13 implied by this hypothesis appears in Fig. 1. The model is adapted to reflect both the available variables in our data set and recent advances in the literature (e.g., the importance of trauma in affecting ART adherence).
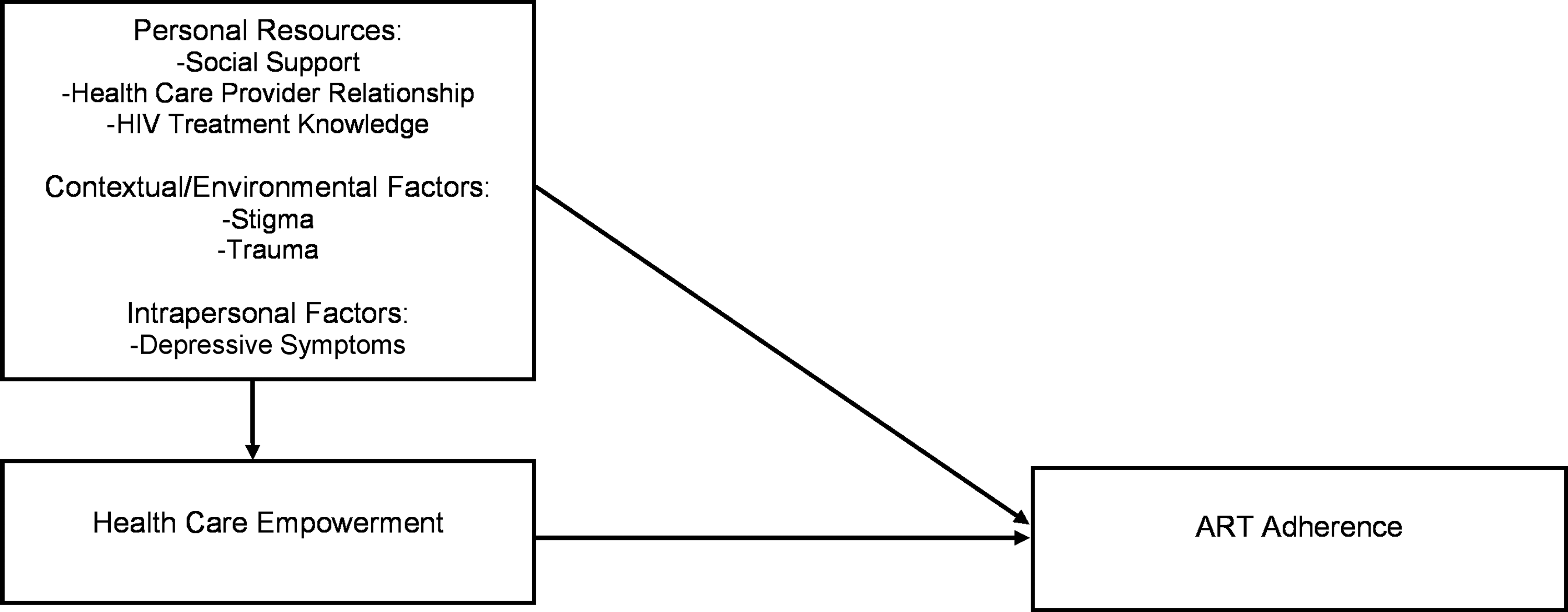
Conceptual healthcare empowerment model. The model depicted is a heuristic (i.e., conceptual) model, not a representation of a specific structural equation modeling to be tested. It is based on preliminary work conducted by Johnson et al. (2012) and updated to reflect the available variables in this study and the inclusion of new constructs from the literature post-2012 (e.g., trauma).
Methods
Participants and recruitment
From May 7 to August 31, 2013, participants were recruited through study advertisements posted online to social networking sites, including Facebook, Twitter, LinkedIn, Craigslist, and Tumblr. Details on how these online sites were used for participant recruitment purposes have been described in detail elsewhere. 18 Inclusion criteria included the following: (1) being 18 years or older, (2) self-reported HIV-positive serostatus, and (3) currently living in the United States. This study was reviewed and approved by the University of California, San Francisco (UCSF) Committee on Human Research. In addition, the UCSF Center for AIDS Prevention Studies Community Advisory Board provided input on the study's design to improve participant recruitment efforts.
Study procedures
Study advertisements directed interested individuals to a study web link that included a consent form followed by a brief online screening survey that was created using Qualtrics Research Suite (Qualtrics, Provo, UT) to determine eligibility based on the study's inclusion criteria described earlier. Persons were excluded from participation if they had already completed the survey. This was determined by asking participants to report if they had previously taken the survey and by limiting access to those who attempted to take the survey more than once based on their Internet protocol (IP) address. The Qualtrics system terminated a survey if a participant tried to re-access the survey from the same IP address but the system did not report the IP address to the researchers (i.e., anonymized responses). For those determined to be ineligible, the Qualtrics system automatically prohibited them from completing the survey. Participant anonymity was ensured because personal identifiers were not collected. In addition, password-protected and encrypted servers at UCSF were used to further protect participant identity.
Monetary incentives were not offered to participants for completion of the online survey to prevent individuals from attempting to access and complete the survey multiple times for financial gain. Instead, five medically interesting “Fun Facts” (e.g., “Did you know that your tongue has a unique print similar to your fingerprints?” and “Did you know that your eyes can see about ten million different colors?”) accompanied by visually appealing and relevant pictures to the facts were strategically placed throughout the survey to increase participant motivation for completing the entire survey. Participants were also asked the following question before initiating the actual survey: “Do you know of a natural substance that can be potentially effective against HIV?” to further encourage interest and engagement in study completion. Participants took an average of 31 min to complete the survey. At the end of study, participants were presented with a link to video that discussed how bee venom is being studied as a potential drug to treat HIV at the Washington University School of Medicine. 19
Measures
Demographic characteristics
Participants' demographic characteristics were assessed, including age, current gender identity, race/ethnicity, sexual orientation, educational level, student status, employment status, and perceived financial stability.
Trauma
Lifetime trauma was assessed with a single question (“Have you ever been abused, threatened, or the victim of violence?”) that was dichotomized into a “yes/no” response (0 = “no”; 1 = “yes”). 20
Stigma
Perceived HIV-related stigma was assessed using a 5-item measure on a 4-point Likert-type scale (0 = “Not at all” to 4 = “Often”) with higher scores indicative of greater levels of stigma. Items include: “I've avoided getting HIV treatment because someone might find out about my HIV”; “I've felt people avoid me because of my HIV”; and “I've feared I would lose my friends if they learned about my HIV.” 21 Cronbach's alpha for the stigma items was 0.75.
Depressive symptoms
Symptoms of depression were assessed using the brief screening 9-item Patient Health Questionnaire (PHQ-9) 22 that asks participants to rate how often they were bothered by specific problems (e.g., “little interest or pleasure in doing things”; “feeling down, depressed, or hopeless”; and “feeling tired or having little energy”) over the last 2 weeks. Each item is scored from 0 to 3 (0 = “Not at all” to 3 = “Nearly every day”). Higher scores indicate higher levels of depressive symptoms. Cronbach's alpha for the PHQ-9 was 0.93.
Social support
A single item from the Social Provisions Scale was used to measure perceived social support. 23 Participants were asked to indicate how strongly they agree or disagree with the following statement: “There are people I can depend on to help me if I really need it” rated on a 5-point Likert-type scale (1 = “Strongly disagree” to 5 = “Strongly agree”) to assess for social support. Higher scores indicate higher levels of social support.
Healthcare provider relationship
The quality of the relationship with their HIV care provider was assessed using a single statement that asks participants to indicate how strongly they agree or disagree with the following statement: “My HIV provider really knows me as a person” rated on a 5-point Likert-type scale (1 = “Strongly disagree” to 5 = “Strongly agree”). 24 Higher scores indicate a closer perceived relationship with the provider.
HCE
HCE was assessed using a shortened 8-item version of the HCE Inventory that was developed and validated by Johnson et al. (2012) 25 that covers two dimensions of HCE, including the state and process of being (1) Informed (e.g., “I prefer to get as much information as possible about treatment options”); Committed (e.g., “I take my commitment to my treatment seriously”); Collaborative (e.g., “I am very active in my healthcare”); and Engaged (e.g., “I try to get my healthcare providers to listen to my preferences for my treatment”); and (2) Tolerant of Uncertainty (e.g., “I accept that the future of my health condition is unknown even if I do everything I can”). Items are rated on a 4-point Likert-type scale with 0 = “Strongly disagree” to four “Strongly agree.” Higher scores indicate higher levels of HCE. Cronbach's alpha for the HCE inventory was 0.82.
HIV treatment knowledge
HIV treatment knowledge was assessed using the HIV Treatment Knowledge Scale (HTKS), 26 in which participants were asked to indicate whether they thought specific statements (e.g., “Once the HIV viral load results are undetectable, HIV medications should be stopped” and “One can get infected with a drug-resistant type of HIV”) were either “True,” “False,” or “Don't Know.” HIV treatment knowledge was scored as the number of items answered correctly, with higher scores indicating higher HIV treatment knowledge. Cronbach's alpha for the HTKS was 0.74.
ART adherence
ART adherence was assessed with a past 30-day rating scale using a single item (i.e., “Rate your ability to take all your medications”) scored from 0 (“Very poor”) to six (“Excellent”), with larger values indicating more adherence. In comparison to the 30-day visual analog scale or the detailed 3-day adherence measure developed by the AIDS Clinical Trials Group that asks about frequencies or percentages, this single item has been noted as providing more accurate ART adherence estimates, similar to those provided by medication event monitoring systems. 27
Statistical analyses
All descriptive and zero-order correlation analyses were conducted using IBM SPSS Statistics for Windows, Release 20.0.0 (©IBM Corp., 2011, Armonk, NY,
Since all available variables for analysis were observed rather than latent and because both direct and indirect pathways were of interest, the goal of this analysis was to use the general SEM framework to fit a saturated path analysis model containing the multiple regression equations implied by Fig. 1 and the direct effects simultaneously and to compute the indirect effects of personal resource variables on adherence through HCE, as predicted by the HCE model. The ART adherence rating item was treated as an ordinal categorical variable in the path analysis using the Mplus WLSMV estimator suitable for use with categorical endogenous variables. Evidence for mediation was determined if the indirect effect from the individual construct through the mediator to the outcome was statistically significant. Due to asymmetry of indirect effects, 5000 bootstrap replications were used to construct empirical bias-corrected (BC) confidence intervals. 29 The statistical significance of effects was determined by BC confidence intervals, which excluded zero. R2 statistics were reported for the endogenous HCE and adherence variables.
Global model fit tests were not used in the current study because the proposed conceptual model is a prespecified, fully saturated path analysis model derived from the theory of HCE developed by Johnson et al. (2012) 13 as described earlier using the observed variables available to us in an existing data set. For a fully saturated model, the global model fit is perfect and for that reason we do not report global model fit statistics. Standardized beta (β) regression coefficients are reported for each direct and indirect effect.
Results
Participant characteristics
The mean age of the sample was 45.6 years (standard deviation = 11.4). The majority of participants identified as male (93.1%), white (71.1%), and gay (86.8%). Most had some experience with college (51.5%) but were not currently in school (87.6%); 45.9% were working full-time. In addition, 46.9% reported that financially they were “barely getting by.” Table 1 provides participant demographic characteristics.
SD, standard deviation.
Means, standard deviations, and zero-order correlations for constructs of interest
Table 2 presents scale means and standard deviations for all constructs of interest, including ART adherence, lifetime trauma, HCE, perceived HIV-related stigma, depressive symptoms, healthcare provider relationship, social support, and HIV treatment knowledge. Zero-order correlations were also examined between the constructs of interest. Significant relationships were found for each zero-order correlation, with ART adherence significantly correlated with lifetime trauma (r = −0.071, p < 0.05), HCE (r = 0.090, p < 0.01), perceived HIV-related stigma (r = −0.080, p < 0.01), depressive symptoms (r = −0.195, p < 0.001), healthcare provider relationship (r = 0.114, p < 0.001), social support (r = 0.061, p < 0.05), and HIV treatment knowledge (r = 0.072, p < 0.05). Based on effect sizes, the relative strengths of these correlations indicate that depressive symptoms had the largest/most robust effect on adherence followed by healthcare provider relationship.
Note: * p < 0.05, ** p < 0.01, *** p < 0.001. Pairwise Ns for correlations ranged from 1107 to 1243.
N/A = not applicable.
Path analysis
Figure 2 displays the statistically significant direct effects from the theoretical model. Simultaneous modeling of the regressions of ART adherence onto HCE and ART adherence and HCE onto the independent variables revealed statistically significant positive associations between healthcare provider relationship and HCE (β = 0.118, p < 0.01) and HIV treatment knowledge and HCE (β = 0.236, p < 0.01). Turning to the ART adherence outcome, higher levels of HCE were significantly associated with ART adherence (β = 0.089, p < 0.05). In addition, higher healthcare provider relationship ratings were positively associated with ART adherence (β = 0.105, p < 0.01), but higher depressive symptom scores (β = −0.187, p < 0.01) and lifetime trauma (β = −0.088, p < 0.05) were negatively associated with ART adherence. Indirect effects of independent variables on ART adherence via HCE were statistically significant and positive for healthcare provider relationship (β = 0.010, p < 0.05) and HIV treatment knowledge (β = 0.021, p < 0.01), suggesting that as provider ratings and HIV treatment knowledge ratings increase, HCE scores also increase, which in turn are associated with higher levels of self-reported ART adherence (Table 3). The R2 for HCE was 8.8% and the R2 for adherence was 8.5%. These standardized effects are between small (2%) and medium (13%), closer to the medium threshold. 30
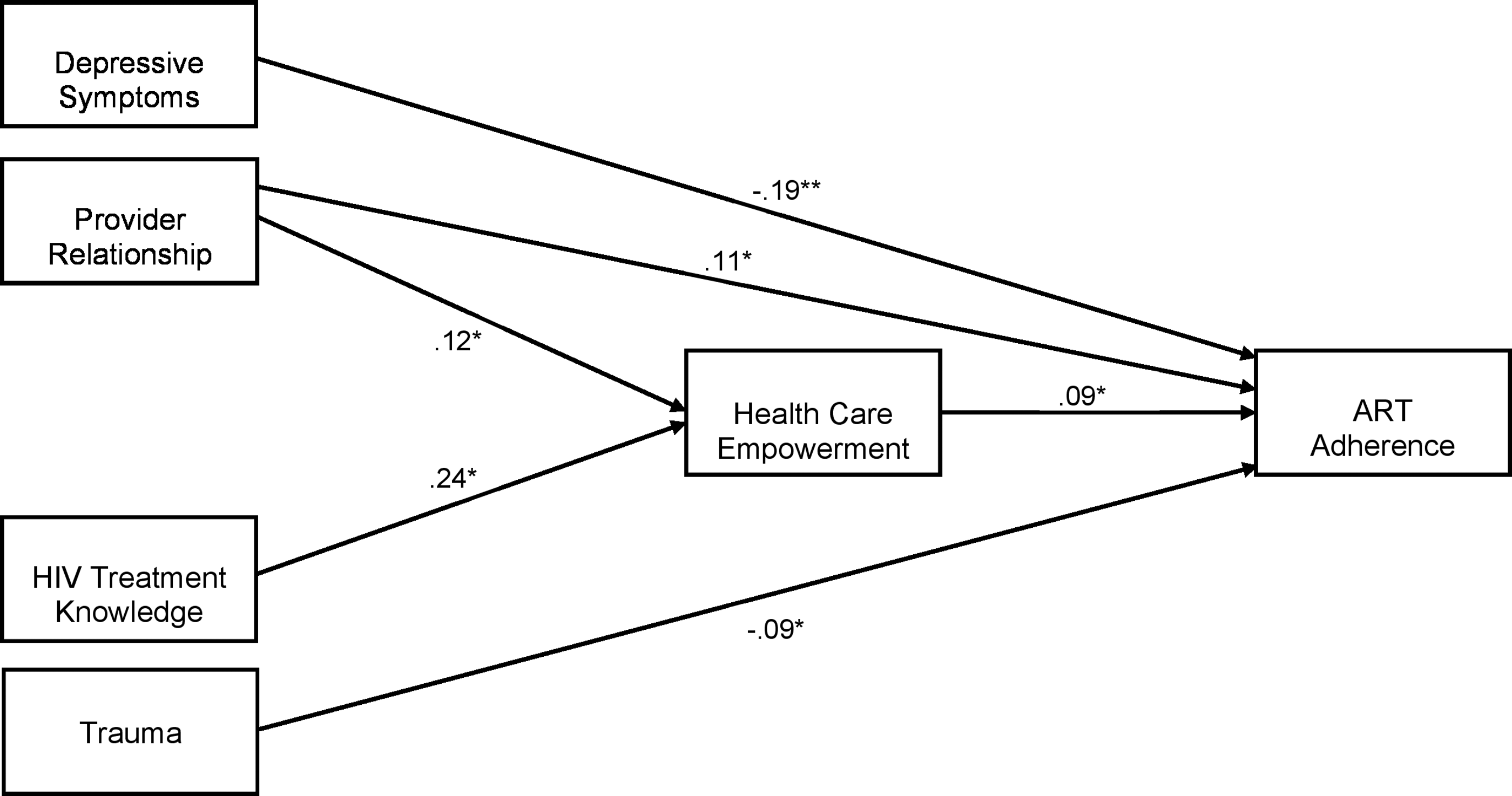
Standardized coefficients for statistically significant direct effects (N = 1302). *p < 0.05; **p < 0.01. To maintain clarity, the exogenous variables stigma and social support, which had no significant direct or indirect relationships with healthcare empowerment and ART adherence, are included in the analysis but excluded from the figure. Similarly, correlations among exogenous variables (e.g., depressive symptoms, provider relationship) are assumed and estimated, but not depicted in the figure. All variables depicted in the figure are observed, not latent. ART, antiretroviral therapy.
B is the unstandardized regression coefficient; 95% CI is the 95% bias-corrected bootstrap confidence interval of B. β is the standardized regression coefficient.
p < 0.05; ** p < 0.01 (determined via 95% and 99% confidence intervals' exclusion of zero, respectively).
HCE, healthcare empowerment.
Discussion
Empowering PLWH to obtain the healthcare that they need to live longer and healthier lives is critical. As predicted by the HCE model, depressive symptoms, healthcare provider relationship, and lifetime trauma all directly impacted ART adherence. Specifically, we found that ART adherence was positively linked to healthcare provider relationship and negatively linked to depressive symptoms and lifetime trauma, with depressive symptoms having the strongest direct effect of these three variables on adherence. In addition, as anticipated, healthcare provider relationship and HIV treatment knowledge were positively associated with and directly influenced HCE. While both provider relationship and HIV treatment knowledge are statistically significant contributors in explaining variance in HCE, the standardized regression coefficient of HIV treatment knowledge is twice that of provider relationship, suggesting that HIV treatment knowledge is the primary correlate of HCE. Finally, as expected, ART adherence was indirectly and positively affected by healthcare provider relationship and HIV treatment knowledge through HCE.
Consistent with prior research, the majority of factors we investigated in this study were related to ART adherence. For instance, the positive relationship between healthcare provider relationship and ART adherence is in line with findings from other studies. 31,32 That is, the stronger an individual's relationship is with their healthcare provider the better that individual will be at adhering to his or her medication regimen. Similarly, the negative link between depressive symptoms and ART adherence was expected based on prior work. 33 Further, higher rates of post-traumatic stress disorder have been associated with lower rates of ART adherence among PLWH in the United States. 34
Our study extends prior research on the HCE model 12,13 and contributes to the extant literature on HIV treatment adherence. The value added by our study is that we used (1) a theoretical framework to understand psychosocial factors that play a dynamic role in affecting ART adherence among PLWH; (2) path analysis to fit the multiple simultaneous equations implied by this theory-based model of HCE as a way of identifying specific intervention targets for addressing individual factors (e.g., healthcare provider relationship, depressive symptoms) to improve ART adherence; and (3) lifetime trauma to extend the HCE model to include this additional factor that has been shown to significantly impact ART adherence among PLWH. 17 Implications of our findings for PLWH and the healthcare providers who provide them with treatment and care are explored in detail below.
Our findings have important implications for both PLWH and the healthcare providers who treat them. Multi-level interventions to increase knowledge about current HIV treatment options, decrease mental health concerns related to depressive symptoms and lifetime trauma, and encourage empowerment to obtain the kind of healthcare needed to increase ART adherence are crucial among PLWH. Moreover, healthcare providers who can be taught to promote HCE among their patients living with HIV will likely see improvements in their patients' engagement and retention in care, which in turn may facilitate better ART adherence leading to virologic suppression and decreased HIV transmission to others. 35,36
Our results suggest that improved ART adherence will occur when PLWH are engaged, informed, collaborative, committed, and tolerant of uncertainty in their healthcare. Engagement in care and treatment includes that both PLWH and their healthcare providers are active participants in the healthcare decision-making process. From a patient perspective, this means being guided toward and having access to appropriate care based on his or her health condition(s); receiving assistance in attending medical visits with appointment reminders; access to affordable transportation and child care; and being able to communicate with one's healthcare providers in multiple ways that may include talking by phone, texting, or online correspondence in between visits. 37 –40
Being well informed and having the ability to convey up-to-date knowledge about a particular illness or condition are imperative for the empowered patients and their healthcare providers. Healthcare providers can make sure that PLWH clearly understand their illness/condition, have an awareness of all treatment options and the relative risks and benefits, and recognize how to navigate the healthcare system to receive the best care possible. 41,42 For example, this may include having providers review rights and privileges, benefits and resources, and any other policies with the patient. New technologies could be used to present this type of information or to administer questionnaires with validated measures relevant to the patients' condition or illness as they are sitting in the waiting area before being seen by their providers. For instance, a report could then be generated and sent to providers with the patients' responses to the questions and total scores for the validated measures with interpretations that could be reviewed by providers before meeting with the patient.
A collaborative relationship between the healthcare provider and patient that is perceived by both parties as being mutually beneficial is imperative for improved adherence to care. To be successful, patients and providers need to work together in making treatment and care decisions for the patient. Providers can help patients learn how to effectively convey their concerns and questions using active communication styles and patients can identify when providers are talking to them about something related to their healthcare that patients do not comprehend. Increasing level of trust in the patient–provider relationship and in the healthcare system in general is also central to building strong, long-term alliances. 43 –46
Essential to the concept of HCE is demonstrating a commitment to a patient's health and treatment plan. Commitment is a key ingredient for a successful union between the patient and provider, especially when there are unforeseen setbacks in treatment or unanticipated disease progression. When this occurs, healthcare providers can help PLWH reassess their current treatment plan and set more realistic goals or expectations based on the patient's present circumstances. With respect to ART adherence, healthcare providers can help patients view engagement in adherence as a continually evolving process. 47 Thus, allowing for flexibility in the treatment plan is important when desired or expected outcomes are not being seen. 48
When an individual is dealing with a life-threatening illness such as HIV, tolerance for uncertainty is paramount. While advances in treatment options have improved substantially for PLWH over the last two decades, there is a level of unpredictability that any person with HIV has to contend with to remain motivated and to stay on track with their treatment and care. Providers can help PLWH manage their emotions regarding the uncertainty of the illness or condition by acknowledging their patients' feelings and concerns while simultaneously providing their patients with information that is informed by assessing the relative risks and benefits of potential treatments based on the provider's own clinical knowledge or by consulting specialists who have the necessary expertise. Balancing the patients' emotional needs while also providing them with rational decision-making for treatment and care on the part of the provider are vital to the patients' health and well-being. 49,50
Even in a busy HIV clinic setting, healthcare providers, including physicians, pharmacists, nurses, psychologists, social workers, case managers, and front desk staff, can work together as a cohesive team to implement the aforementioned strategies to create an empowered healthcare environment for PLWH. For example, physicians, pharmacists, and nurses can educate their patients about current HIV treatment options and answer any medical questions patients may have during or after their visits. Psychologists and social workers can provide patients with ongoing mental health treatment to decrease depressive symptoms, trauma, or any other psychological challenges. Case managers can review policies and procedures with patients, facilitate transportation and child care for patients, and send appointment reminders to patients. Front desk staff can greet patients in a friendly, nonjudgmental manner and administer questionnaires to patients in the waiting area. Inspiring and fostering HCE is about how well the entire system of healthcare functions synergistically and efficiently.
The current study has some limitations that are important to highlight. First, our findings may not generalize to all PLWH in the United States because our participants were predominately white and gay men and we sampled users of online social media. Despite this, Internet-based surveys have been lauded for their ability to reach large numbers of individuals living in various geographic regions and hard-to-reach populations who may not otherwise participate in research studies where they must reveal their identities to the interviewer because of the in-person nature of the interaction. 51 Second, the possibility of duplicate or false responses by participants arises with any research conducted online. However, we tried to minimize these concerns by not providing monetary incentives for participation and using the Qualtrics program that automatically disqualifies individuals who attempted to access the online survey more than once based on duplicate IP addresses. Third, social desirability or other reporting biases are potential problems with self-report data. Biological indicators (e.g., viral load, CD4) should be collected in future research to confirm our findings based on self-report. Nevertheless, as previously noted, these issues may be lessened with the use of an online survey that maintains participant anonymity. 51 Fourth, due to the need to balance participant burden and likelihood of completing the online survey with psychometric rigor, some of the measures used (e.g., social support and healthcare provider relationship) were single questions or items that may not fully capture the complexity of the factors under investigation. On the contrary, some measurement developers have argued that single-item measures demonstrate equally high predictive validity as multi-item scales. 15,16 Fifth, this study uses a cross-sectional design, which does not allow for causality to be determined and opens up the possibility that our results may have been impacted by other unmeasured factors. Longitudinal data testing the relationships among the constructs investigated in the current study would help to address some of these shortcomings. Finally, a limitation of the current study is the use of path analysis with observed variables. To address this concern, it is recommended that future studies incorporate latent constructs measured by multiple indicators so that measurement error can be isolated from the structural part of the model and so that global model fit can be evaluated formally. To optimally evaluate the stability of the model, new samples would be required. 52 Despite these limitations, this study offers promising support of the HCE model for understanding the dynamic interplay of psychosocial factors that directly and indirectly impact ART adherence among a large sample of PLWH in the United States.
Multi-level interventions with PLWH and their healthcare providers are urgently needed to address the effects of the investigated psychosocial factors on ART adherence. Further investigation is needed to determine if higher HCE scores among PLWH may predict improved long-term engagement and retention in care, which in turn may lead to better ART adherence and virologic suppression, followed by lower morbidity and mortality among this population. Future work is warranted to test our HCE model longitudinally and with diverse populations of PLWH in terms of race/ethnicity, sexual orientation, and gender to replicate and confirm our findings. It is also important for additional research to determine how much each of the five components (engaged, informed, collaborative, committed, and tolerant of uncertainty) contributes to the experience of HCE separately or in conjunction with one another by PLWH for ART adherence.
Footnotes
Acknowledgments
The authors are greatly appreciative of the members of the UCSF Center for AIDS Prevention Studies Community Advisory Board, and are especially grateful to all of the individuals who participated in this study. The authors specially thank Maria Isabel Fernández, PhD, and the Adolescent Medicine Trials Network for HIV/AIDS Interventions Scholars Program that helped to initiate and foster this collaboration. Preliminary data from this research were presented at the 11th Annual International Conference on HIV Treatment and Prevention Conference in Fort Lauderdale, Florida. This project was supported, in part, by the National Institutes of Health (NIH) Providence/Boston Center for AIDS Research (CFAR) (P30 AI042853, PI: Cu-Uvin), NIH UCSF-Gladstone Institute of Virology & Immunology CFAR (P30 AI027763, PI: Volberding), and NIH Career Development Awards (K23 MH097649, PI: Saberi; K24 DA037034, PI: Johnson; K24 MH087220, PI: Johnson). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author Disclosure Statement
No competing financial interests exist.