
Abstract
HIV-related stigma remains a persistent global health concern among people living with HIV/AIDS (PLWA) in developing nations. The literature is lacking in studies about healthcare students' perceptions of PLWA. This study is the first effort to understand stigmatizing attitudes toward HIV-positive patients by healthcare students in Mwanza, Tanzania, not just those who will be directly treating patients but also those who will be indirectly involved through nonclinical roles, such as handling patient specimens and private health information. A total of 208 students were drawn from Clinical Medicine, Laboratory Sciences, Health Records and Information Management, and Community Health classes at the Tandabui Institute of Health Sciences and Technology for a voluntary survey that assessed stigmatizing beliefs toward PLWA. Students generally obtained high scores on the overall survey instrument, pointing to low stigmatizing beliefs toward PLWA and an overall willingness to treat PLWA with the same standard of care as other patients. However, there are gaps in knowledge that exist among students, such as a comprehensive understanding of all routes of HIV infection. The study also suggests that students who interact with patients as part of their training are less likely to exhibit stigmatizing beliefs toward PLWA. A comprehensive course in HIV infection, one that includes classroom sessions focused on the epidemiology and routes of transmission as well as clinical opportunities to directly interact with PLWA—perhaps through teaching sessions led by PLWA—may allow for significant reductions in stigma toward such patients and improve clinical outcomes for PLWA around the world.
Introduction
S
HIV-related stigma remains a persistent global health concern among PLWA in developing nations, further complicating prevention efforts and access to medications. 4 –6 UNAIDS defines HIV stigma as the negative beliefs, feelings, and attitudes toward people living with HIV that result in discriminatory behavior. 7 HIV stigma often results from a fear of transmission and the association of HIV with culturally sensitive activities such as sex, drug use, and prostitution that bring into question the character of an individual infected with HIV. 8 The stigma can present itself as verbal discrimination (gossiping, taunting, or blaming by community members), social discrimination (reduced visits by friends and family), physical discrimination (violence toward PLWA), and institutional discrimination (loss of employment and inequitable provision of healthcare services). 8,9 Consequently, PLWA often experience isolation and internalized stigma, wherein an individual with a disease state perceives himself or herself as less valuable than others in the community and produces negative self-perceptions. 8,10 Numerous studies have also reported that individuals affected by stigma suffer from negative psychosocial and mental effects 7,11 –15 as well as reduced adherence to ARTs and disclosure to sexual partners. 16 –19
Of particular interest to this study is stigma in healthcare settings, which manifests as neglect, denial of services, disclosure of HIV status to others without patient consent, and verbal abuse by healthcare providers. 20 There are several reports of healthcare-related stigma by providers contributing to the negative physical and mental health of PLWA. 20 –22 However, many of the healthcare providers surveyed in these previous studies may hold different values from the current healthcare students who are being raised in a different generation. Healthcare students stand as the future healthcare leaders of their communities and understanding their perceptions toward HIV-positive patients will provide insight into generational changes in perceptions of HIV. It will also act as a way to ascertain the potential need for incorporation of educational curricula that target reduction of HIV-related stigma.
To our knowledge, HIV-related stigma among healthcare students in Tanzania has never been studied. Further, no study has assessed stigma in healthcare students entering nonclinical professions, such as medical laboratory or health information management, which are indirectly involved with patient care. In this study, we surveyed healthcare students in Mwanza, Tanzania, entering both clinical and nonclinical fields for various aspects of HIV-related stigma to better understand its potential impact on PLWA.
Materials and Methods
Setting
The study was conducted over a 4-week period in June 2016 at the Tandabui Institute of Health Sciences and Technology (TIHEST) in Mwanza, Tanzania. Mwanza is the second largest city in Tanzania and has an ∼4.6% HIV prevalence rate. 3 TIHEST is a health professions training institute recognized by the Tanzanian Ministry of Health that offers certificates and diplomas in Clinical Medicine, Laboratory Sciences, Health Records and Information Management, Nursing, and Community Health.
Study participants
Study participants were drawn from Clinical Medicine, Laboratory Sciences, Health Records and Information Management, and Community Health classes at TIHEST. At TIHEST, Clinical Medicine students who complete 1 year of pre-clinical and 1 year of clinical training are given the title of Clinical Assistant, and those who pursue another additional year of clinical training are titled Clinical Officers.
While individuals trained in Clinical Medicine are not permitted to perform complex surgical procedures, they can conduct basic physical examinations, prescribe medications, and perform minor surgical procedures such as those involved in childbirth. Students who complete the Clinical Medicine program are not considered physicians; the purpose of Clinical Medicine training programs is to increase the number of individuals within developing nations who are able to provide basic medical care to regions lacking health services. 23 Laboratory Science students at TIHEST are extensively trained in diagnostics through a 2-year program, learning how to prepare specimens for microscopic viewing as well as how to identify pathology. Health Records and Information Management students take a 2-year program to learn how to manage patient health information, and Community Health students undergo a 1-year curriculum that prepares them to enter social work, nursing, or radiologic imaging.
A basic outline of the core courses of each program by year (Table 1), obtained from TIHEST administration, reveals that Clinical Medicine students are the only students who complete several clinical rotations and are directly involved in the handling and treatment of patients. They are also the only students specifically enrolled in an HIV/AIDS course during the optional third year of study. However, it is still important to consider the stigmatizing attitudes that other healthcare students entering nonclinical professions may hold toward HIV-positive patients as they will still be indirectly involved in patient care through diagnostics and/or handling private health information. Consequently, we classified the students into Clinical Medicine Year 1 (pre-clinical experience only), Clinical Medicine Years 2–3 (pre-clinical and clinical experience), or Other (Health Records and Information Management, Laboratory Sciences, and Community Health) for the purposes of our analysis of survey responses.
TIHEST, Tandabui Institute of Health Sciences and Technology.
Study design
The University of California, Irvine, granted Institutional Review Board approval for this cross-sectional study. A composite survey was developed utilizing questions from three previous studies 24 –26 to assess the healthcare students' perceptions of HIV-positive patients in three domains: personal or cultural beliefs about HIV, HIV education, and clinical interactions with HIV-positive patients. The finalized survey consisted of 18 questions: 9 questions assessed personal or cultural beliefs about HIV, 5 assessed HIV education, and 4 assessed clinical interactions with HIV-positive patients (Table 2). The survey was translated into Swahili, the primary language of Tanzania.
For each question, responses of “Agree,” “Disagree,” or “Don't know” were the possible options. “Don't know” was included as an option to ensure that participants did not leave questions unanswered. A scoring scheme was developed so that higher scores indicated lower levels of stigmatizing beliefs toward HIV. For questions 1, 3, 4, 5, 7, and 9–14, a response of “Agree” was given a score of 0, while a response of “Disagree” was given a score of 1 because a response of “Disagree” indicated a lower level of stigmatizing beliefs.
For questions 2, 6, 8, and 15–18, a response of “Agree” was given a score of 1, while a response of “Disagree” was given a score of 0 because a response of “Agree” indicated a lower level of stigmatizing beliefs. A response of “Don't know” was always given a score of 0. Consequently, the highest score that a student could receive for personal or cultural beliefs about HIV was 9, for HIV education was 5, and for clinical interactions with HIV-positive patients was 4, summing up to a perfect total score of 18. In addition to the survey, basic demographic information—age, gender, and student type (Clinical Medicine Year 1, Clinical Medicine Year 2, Health Records and Information Management, Laboratory Sciences, or Community Health)—was collected.
Recruitment
Study investigators invited potential participants to complete the voluntary survey and provided them with the survey and information sheets, available in both English and Swahili. A convenience sampling method was used to recruit participants as only those students who were present at the TIHEST campus over the course of the 1-month study period were actively recruited for survey completion. Participants gave verbal consent after speaking with coinvestigators about the study and reviewing the information sheet.
Participants were informed that no identifying information would be obtained, all responses were anonymous, and there were no repercussions for survey responses on school evaluations. If students were still unclear about the study after speaking with coinvestigators and consulting the information sheet, we enlisted the assistance of TIHEST administrative staff to clarify the study's purpose and its response anonymity in Swahili. While every effort was made by coinvestigators and TIHEST staff to ensure that students had a private space to complete the survey, in some cases when space was limited, study investigators monitored a classroom with participants to ensure they could not see one another's responses.
Data analyses
Data were analyzed using XLSTAT 2016 for Windows. 27 All variables were characterized using descriptive statistics, with frequencies and percentages reported for categorical variables and means, standard deviations, and medians reported for continuous variables. Participants who did not complete all questions on the survey were excluded in all analyses.
Scores for each of the three survey categories were plotted to assess normality. Nonparametric tests were used for analyses, including Mann–Whitney tests for dichotomous variables (e.g., sex) and Kruskal–Wallis tests for categorical variables with multiple levels (e.g., student type). Due to the heavily skewed distributions, the subscore variables were split into two roughly even categories—low values, less than the median, and high values, greater than or equal to the median. A two-way ANOVA was conducted to compare the main effects of age (age ≤24, age >24) and student type (Clinical Medicine Year 1, Clinical Medicine Years 2–3, Other) and the interaction effect between the two variables on stigma scores. Associations between personal and cultural beliefs and HIV education subscores against clinical interaction subscores were assessed using chi-squared tests. A p-value <0.05 was considered statistically significant.
Results
A total of 255 students at TIHEST took the survey, but 45 students were excluded because they did not complete all questions on the survey, and the remaining sample consisted of 210 students. The mean age was 23.9 years, and the average age of students in Clinical Medicine Year 1 was 23.5 years, in Clinical Medicine Years 2–3 was 27.2 years, and in Other students was 21.6 years, with the differences between these ages being statistically significant (p < 0.0001) (Table 3). Of all students who took the survey, mean scores of 5.9, 3.6, and 3.4 as well as median scores of 6, 4, and 4 were obtained for personal or cultural beliefs about HIV (9 points total), HIV education (5 points total), and clinical interactions with HIV-positive patients (4 points total) subscores, respectively. As the subscores suggest, there was a negative skew in the distributions of subscores and the total score, pointing to an overall trend in low stigmatizing beliefs toward HIV (Fig. 1).
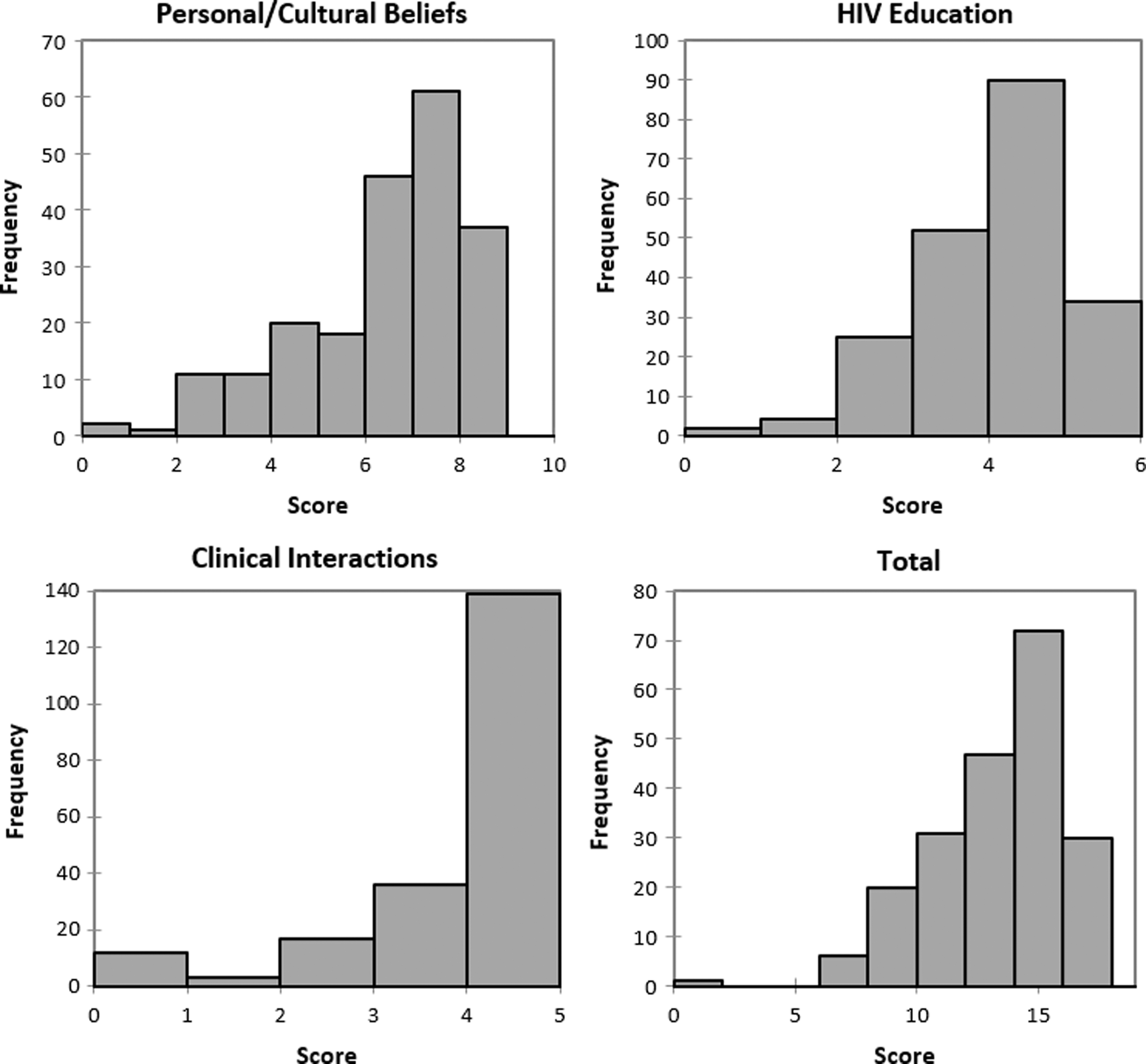
Distribution of each subscore and total score for the survey. Higher scores indicate lower stigmatizing beliefs.
SD, standard deviation.
A breakdown of responses to each question of the survey was reviewed, with several notable points emerging that the subscores themselves did not elicit (Table 2). With regard to personal and cultural beliefs about HIV, 23.1% of all participants believed that HIV is a punishment for bad behavior and 30.8% believed that people who got HIV from drug use or sex deserved to become infected. Additionally, more participants cited that they would feel ashamed if they themselves became infected with HIV than if someone close to them was infected. Further, despite an overall high HIV education subscore among participants, 69.2% believed that individuals who are HIV positive could have avoided infection if they wanted to and 26.0% believed that HIV-positive patients have had many sexual partners. Despite this, the overwhelming majority of participants would be willing not only to work with HIV-positive patients but also to provide an equitable quality of care to other patients with whom they would interact.
An analysis of subscores was conducted in the context of demographic variables and in relationship to one another. While subscores were similar between male and female respondents, students older than 24 years were more likely to obtain a higher personal and cultural beliefs about HIV subscore than were those younger than 24 years old (7.0 vs. 6.5, p = 0.03; Table 4). There was also a significant difference between the personal and cultural beliefs about HIV subscore means between students in different programs, with Clinical Medicine Years 2–3 students exhibiting the highest score (6.8 for Clinical Medicine Year 1 vs. 7.1 for Clinical Medicine Years 2/3 vs. 6.2 for Other, p = 0.01). This difference in HIV stigma levels among the three student types remained significant when the subscores were totaled (13.8 vs. 14.3 vs. 13.6, respectively, p = 0.04) (Table 4).
The interaction between age and student type on total score was not significant (p = 0.22) (Table 5). However, when the effects of age and student type on total score were analyzed simultaneously, there were no significant main effects of age (p = 0.40) or student type (p = 0.28) on total score. Students with high personal and cultural beliefs about HIV subscores were more likely than those with low subscores to achieve high clinical interaction scores (73.9% vs. 54.3%, p = 0.005) (Table 6).
p values were extracted from two-way ANOVA test.
Age group: age ≤24 versus age >24.
CM2/3, Clinical Medicine Years 2 and 3; CM1, Clinical Medicine Year 1; O, Other.
p values were extracted from chi-squared test. Low personal/cultural beliefs is score of 0–6; high personal/cultural beliefs is score of 7–9; low HIV education is score of 0–3; high HIV education is score of 4–5; and high clinical interaction is score of 4. Median of personal/cultural beliefs score was 7; median of HIV education score was 4; and median of clinical interaction score was 4.
Discussion
HIV-related stigma has public health consequences that complicate lifelong treatment of affected patients beyond access to ARTs. This study is the first effort toward understanding stigmatizing attitudes toward HIV-positive patients by healthcare students in Tanzania, not just those who will be directly treating patients but also those who will be indirectly involved through nonclinical roles, such as handling patient specimens and private health information. In this study, we provide a point-by-point interpretation of significant findings.
Individual survey item responses
While healthcare students generally scored well on the overall survey, responses to individual questions indicate gaps in knowledge about HIV and in personal or cultural beliefs about PLWA. With regard to HIV education, over two-thirds of respondents believed that PLWA could have avoided HIV if they wanted to, and over one-fourth believed that PLWA have had many sexual partners. This suggests that the students were less aware of the routes of HIV infection beyond behavioral routes such as drug use and sex with same sex or different sex partners. Education about the routes of transmission outside of an individual's control, such as mother-to-child transmission, may foster a greater sense of empathy in these future healthcare leaders. In fact, qualitative studies have found that community members are more supportive of PLWA who contracted HIV without participating in socially improper behaviors, such as women who become infected from their husbands, children who become infected from their mothers, and healthcare workers infected while working. 8
With regard to personal and cultural beliefs about HIV, nearly one-fourth of the students believed HIV is a punishment for bad behavior and nearly one-third believed people who contracted HIV through drug use or sex deserved to become infected, suggesting that while students generally scored high on personal and cultural beliefs about HIV, they still exhibit blame toward PLWA.
Notably, survey responses showed that more students would feel ashamed if they themselves became infected with HIV than if someone close to them was infected. This may be suggestive of internalized stigma, which can be influenced by stigma from those around the affected patient, and has been found to contribute to several mental and public health consequences, namely depression, social isolation, poor disclosure of HIV status, and unsafe sex practices. 28 –31 Since more students would feel ashamed of their own infection than that of others, it appears that internalized stigma plays a contributory role in that shame. It is important, therefore, that students learn not just about HIV infection and stigma by one's community but also about how to tackle the mental health issues that PLWA experience as a result of internalized stigma.
Age and HIV stigma
Students who were older than the sample mean of 24 years had a significantly higher personal and cultural beliefs about HIV subscore than students who were younger than 24 years. This suggests that older students may exhibit less stigmatizing personal or cultural beliefs about PLWA than younger students. One possible explanation for this trend could be found in previous findings that report lower stigmatizing attitudes in individuals with higher levels of education. 32 –34
While we did not collect information about the educational backgrounds of the participants in the study, it may be possible that older students have had more educational experiences (in the form of other degrees or programs of study) than younger students in the same program. Importantly, further analyses revealed that second and third-year Clinical Medicine students were significantly older than first-year Clinical Medicine students, likely due to being further along in the program and in their education. It is important to note that this association was reduced to a nonsignificant p-value when student type and age were analyzed simultaneously.
Student type and HIV stigma
Student type had an association with stigmatizing attitudes, with Clinical Medicine students in their second or third year of study having a significantly higher personal and cultural beliefs about HIV subscore as well as overall score on the survey instrument than first-year Clinical Medicine students and students in other healthcare fields. To note, this association lessened when student type and age were examined simultaneously; although this relationship is not to the extent of being statistically significant, we believe the prevailing low p-value suggests that student type is still somewhat associated with HIV stigma scores, namely the personal and cultural beliefs about HIV subscore and the total score.
The major difference between second and third-year Clinical Medicine students and all other students may involve two factors. First, second- and third-year Clinical Medicine students uniquely receive clinical training, and thus the opportunity to interact with patients and PLWA, as part of their program to complement the pre-clinical courses they took during their first year. Indeed, previous studies have found that pre-clinical students are more stigmatizing and less willing to work with PLWA than clinical students. 35,36 Our finding also supports the contact hypothesis, which claims that interpersonal interactions with individuals in a particular group can reduce prejudice toward that group. 37 Previous studies in the context of HIV have found benefits of the application of the contact hypothesis in reducing stigmatizing attitudes and beliefs toward HIV-positive patients. Individuals who have had direct contact with PLWA have been found to exhibit less blame, 38 increased tolerance, 39 and overall reduced stigmatizing attitudes 40 –43 toward PLWA.
Second, third-year Clinical Medicine students are the only students who take a specific course about HIV. While we did not distinguish between second- and third-year students in our data collection, it is possible that this specific education allows for third-year students to have lower overall stigmatizing beliefs toward PLWA. Indeed, previous literature has cited that more knowledge about HIV contributes to lower stigmatizing beliefs. 44 Clinical Medicine students in their second and third years of training had the lowest overall score on the survey, suggesting that clinical experience or an HIV education course plays a role in their low stigmatizing beliefs. This finding is meaningful because it suggests the need for all students, not just Clinical Medicine students, to have patient contact as part of their training curriculum as well as knowledge-building HIV courses.
Further, there was a significant positive association between the personal and cultural beliefs about HIV subscore and clinical interactions subscore, suggesting a relationship between students' personal opinions about PLWA and the way they handle such patients in a clinical setting. The contact hypothesis may be one explanation, in that the patient interactions and clinical experience gained by second- and third-year Clinical Medicine students could play a role in improving personal and cultural beliefs about HIV. However, students' personal opinions contrarily could change the way they treat patients, or other factors may be at play. Future studies are needed to further investigate the relationship between personal beliefs about HIV and clinical interaction.
Educating future healthcare providers
Generally, students obtained high scores on the overall survey instrument, pointing to low stigmatizing beliefs toward PLWA and a willingness to work with and treat PLWA with the same standard of care as other patients. However, there are gaps in knowledge that exist among a large proportion of students, such as a comprehensive understanding of all routes of HIV infection beyond unsafe sex and drug use. It is vital for healthcare students and providers alike to be educated about the biology and psychosocial aspects of HIV infection as it will allow them to establish trusting relationships with PLWA. A poor relationship with healthcare providers—either a lack of trust in the provider or poor treatment on the part of the provider—has consistently been found to be associated with negative health outcomes and retention of care, not just in Tanzania but also in other developing and developed communities around the world. 45 –48
Our study suggests that students who interact with patients as part of their training are less likely to exhibit stigmatizing beliefs toward PLWA. We believe that requiring all students to complete a comprehensive course in HIV infection—covering the basic science, clinical, social, and mental health aspects of the virus—that includes opportunities to interact with PLWA may allow for significant reductions in stigma toward such patients and improved clinical outcomes for PLWA around the world. A recent study pointed to the benefits of such a program, where even inviting PLWA to be instructors for medical students—a patient instructor model—has been found to reduce the stigmatizing attitudes of those students. 49 Unfortunately, such a practice has not yet been implemented on a large scale. Therefore, future studies should investigate the merits of programs that incorporate direct contact with PLWA in changing the potentially stigmatizing perceptions of healthcare students.
Study limitations
This study is not without limitations. Because the study relied on survey responses to assess stigmatizing beliefs, there is the potential for response bias. While we surveyed participants over the course of a month in an attempt to survey as many students available on campus as possible, we inevitably could not collect data from all students at TIHEST due to time constraints. Additionally, this study only surveyed healthcare students at TIHEST and thus findings cannot be extrapolated to all Tanzanian or African healthcare students. Finally, given the limited resources of the school and the region in general, it was difficult to obtain a private room for each student to complete the survey, and it is possible that the presence of other students in the same room taking the same survey may have influenced some responses. Regardless of these limitations, this study is the first to investigate healthcare students' perceptions about HIV and PLWA in Tanzania and to survey students who are not directly involved with patient care, but are still intimately involved with the healthcare process.
Footnotes
Acknowledgments
The authors would like to express their gratitude to Erick Oguta for his persistent efforts in forming relationships with the various partners on the ground in Mwanza. They would also like to thank the Tandabui Institute of Health Sciences and Technology (TIHEST) for allowing them to conduct the study and use resources such as classroom space and staff for survey administration. Finally, the authors would like to thank Jackline Mueni Muthoka and Johnes Ghati Kitololo for their assistance in translating the survey instrument and study information sheet into Swahili. This work was supported by the Infectious Disease Society of America Medical Scholars Program; University of California, Irvine, School of Medicine Global Initiative; and PENdulum Global.
Author Disclosure Statement
No competing financial interests exist.