
Abstract
HIV-1 infection requires the presence of the CD4 receptor on the target cell surface and a coreceptor, predominantly CC-chemokine receptor 5 (CCR5). It has been shown that individuals who are homozygous for a defective CCR5 gene are protected from HIV-1 infection. A novel self-inactivating lentiviral vector LVsh5/C46 (Cal-1) has been engineered to block HIV-1 infection with two viral entry inhibitors, conferring resistance to HIV-1 infection from both CCR5 and CXCR4 tropic strains. Cal-1 encodes a short hairpin RNA (sh5) to downregulate CCR5 and C46, an HIV-1 fusion inhibitor. Gene therapy by Cal-1 is aimed at transducing CD4+ T cells and CD34+ hematopoietic stem/progenitor cells in an autologous transplant setting. Pre-clinical safety and efficacy studies in vitro and in vivo (humanized mouse model and nonhuman primates) have shown that Cal-1 is safe with no indication of any toxicity risk and acts to decrease viral load and increase CD4 counts. Two clinical trials are underway using Cal-1: a phase I/II study to assess safety and feasibility in an adult HIV-1-positive population not on antiretroviral therapy (ART); and a second Fred Hutchinson Investigator Initiated phase I study to assess safety and feasibility in adults with HIV-1-associated non-Hodgkin or Hodgkin lymphoma.
N
There are a variety of approaches in clinical trials for HIV-1, ranging from antiretrovirals to immune approaches to vaccines to cell-delivered gene therapy. 8 –10 Calimmune, Inc. is a clinical stage biotechnology company focused on gene therapy and is currently working on early clinical stage development of HIV-1/AIDS gene therapies. Calimmune's HIV-1 program includes a gene-modified CD4+ T cell/stem cell therapeutic that is based on technology developed in the laboratories of Nobel Laureate Dr. David Baltimore (California Institute of Technology), Dr. Irvin Chen (University of California, Los Angeles), and Dr. Inder Verma (Salk Institute for Biological Studies). 11 –15 Calimmune's first therapeutic candidate, Cal-1, is currently in a Calimmune-sponsored phase I/II clinical trial 16 and an Investigator Initiated phase I clinical trial through the Fred Hutchinson Cancer Research Center (FHCRC). The clinical work for the Cal-1 phase I/II was funded, in part, by the California Institute for Regenerative Medicine (CIRM).
The HIV-1 life cycle begins when the virus binds to the CD4 receptor and one of two coreceptors, CCR5 or C-X-C chemokine receptor type 4 (CXCR4), on the surface of target cells (mainly CD4+ T lymphocytes). 1,17 –19 HIV-1 DNA is produced from HIV-1 RNA via reverse transcriptase and can enter the host cell's nucleus. Integrase facilitates the integration of HIV-1 DNA, called provirus, into the host DNA, and it can then replicate or remain dormant for several years producing a few to no new copies of HIV-1 in that time. 17,20 If dormant (latent), activation of the virus leads to transcription and translation, producing viral proteins. 17,20 In the cytoplasm, protease cuts long chains of HIV-1 proteins into smaller proteins, which are then combined with HIV-1 RNA producing new virus particles. 20,21 These newly assembled virions can bud out from the host cell and infect other cells. 17,20,21 Some potential points of inhibiting the HIV-1 life cycle include entry via cell surface receptors, reverse transcription, integration of the provirus, transcription and translation, and assembly and release of new virions. 8
Anti-HIV-1 genes have been shown to provide resistance to HIV-1 infection. 5,8,22 –27 Building on the experience from the “Berlin patient,” there is evidence that gene therapy could lead to a cure. 5,7,22 HIV-1 mainly infects blood cells; therefore, protecting these cells and precursors is a logical step. One strategy of gene therapy is to deliver anti-HIV-1 genes via a lentiviral vector to autologous HSPCs that can give rise to both CD4+ cells via T lymphocyte development, and macrophages via myeloid development. Delivery in this manner to HSPCs would have the potential for long-term protection. In addition, delivery of anti-HIV-1 genes to CD4+ T cells may be able to confer short- to medium-term protection. 28 Cal-1 is a combination gene therapy to prevent attachment, fusion, and entry of HIV-1. The lentiviral vector Cal-1 encodes a short hairpin RNA (sh5) to downregulate CCR5, and C46, an HIV-1 fusion inhibitor. 25 Sh5 was selected from a library of more than 1600 clones. 11,15,29 It has been shown to be active against R5 tropic forms of HIV-1 both in vitro and in vivo 11,15,30 and includes 10 years of simian safety data. 15,31 Over a decade of research has been conducted on C46. 23,25,32 It has been engineered for expression on the cell membrane with no systemic toxicity. 32 C46 exhibits strong anti-HIV-1 activity against both R5 and X4 tropic strains and was shown to be safe with no immunogenicity in a phase I trial. 32 Internal promoters introduced via self-inactivating lentiviral vector drive sh5 and C46 with consistent expression. 25
Cal-1 is active against both R5- and X4-tropic strains of HIV-1. 24,25,33 The combination of sh5 and C46 anti-HIV-1 agents is more effective than either agent alone, utilizing two points of inhibition for R5-tropic HIV-1, and mitigates against resistance of HIV-1. 24,25,33 The biological activity of Cal-1-transduced HIV-1-negative primary human peripheral blood mononuclear cells (PBMC) showed simultaneous knockdown of CCR5 and C46 expression. 25 Multiple safety and toxicity studies were conducted on Cal-1 giving no indication of any toxicity risk. 24,25,31,33 The studies included cell progenitor colony assessment (using methylcellulose colony progenitor assays on CD34+ cells), apoptosis (caspase assays on primary human PBMCs), proliferation studies (in primary human PBMCs), inflammation studies (via IFNγ, TNFα, and IL6 ELISA), recombination and replication competent lentivirus formation, mutagenic potential of Cal-1 and insertional mutagenesis, and safety and toxicology assessment of Cal-1-transduced CD34+ HSPCs in NOD/SCID/IL2rγ−/− (NSG) mice. 24,25,31,33 Efficacy studies were done using tissue culture, mouse models, and a nonhuman primate (NHP) model; all exhibiting the ability of Cal-1 to inhibit HIV-1 infection and promote target cell survival. 24,25,31,33 When Molt4/CCR5 cells were transduced with Cal-1 and then challenged with R5 tropic Bal or X4 tropic NL4-3 HIV-1 strains, the gene-modified cell lines were able to confer cellular resistance from HIV-1 infection as measured by viral p24 antigen. 25 Similarly, primary human PBMCs transduced with Cal-1 and then challenged with R5 tropic NFNSX or X4 tropic NL4-3 HIV-1 strains were capable of inhibiting HIV-1 infection. 25
Efficacy studies were conducted in NSG humanized bone marrow, liver, thymus (BLT) mouse models. Irradiated NSG mice received human fetal liver-derived CD34+ HSPCs, and then, the animals were divided into two groups: one control group that received nonmodified CD34+ HSPCs and one treatment group that received CD34+ HSPCs transduced with Cal-1. Both groups received CD34+ HSPCs transplanted with thymic stromal tissue and Matrigel under the mouse kidney capsule. At week 12 post-transplantation, animals that survived with >10% human CD3+ T cells were designated for balanced ex vivo and in vivo HIV-1 challenge assays. Ex vivo challenge experiments using splenocytes from BLT mice humanized with Cal-1 showed protection from infection by R5 (Bal) and X4 (NL4-3) tropic strains. In vivo studies resulted in protection of CD4+ T cells and reduction of HIV-1 viremia. 24
Cal-1 was also tested using an autologous stem cell transplant model in NHPs. 31 Juvenile pigtailed macaques were primed with granulocyte colony-stimulating factor (G-CSF) and stem cell factor (SCF) before bone marrow harvest. CD34+ HSPCs, enriched from bone marrow, were prestimulated with cytokines and then transduced with Cal-1. Irradiated animals were infused with autologous gene-modified cells followed by SHIV-1 challenge 9–11 months postautologous transplant. Infused animals exhibited long-term, multi-lineage engraftment of gene marked cells. Animals were protected from SHIV-1-mediated immunodepletion and CD4+ T cell counts gradually returned to prechallenge levels. The plasma viral load set point was significantly reduced and continued to decrease over time. Following SHIV-1 challenge, a preferential increase in gene marking was detected in both CD3+ and CD4+ peripheral blood subsets. 31 In addition, there was polyclonal engraftment detected with an enrichment of clones observed within the CD3+ subset following SHIV-1 challenge. 31 It is of note that the NHPs appear to mount an effective cytotoxic T cell and antibody response to SHIV following C46 stem cell transplantation. 34
Based on pre-clinical in vitro and in vivo safety and efficacy studies, Cal-1 is currently in clinical testing in a phase I/II trial to treat HIV-1 infection in adults who were treated with antiretroviral therapy (ART), but who are not currently taking it due to concerns over toxicity of treatment fatigue 16 and in a separate Investigator Initiated phase I study to treat patients with HIV-associated Hodgkin and non-Hodgkin lymphoma. 35
The therapy is engineered for cellular resistance to HIV-1 infection by selective survival of the Cal-1 containing cells; selection is mediated by ongoing HIV-1 infection. Administration of Cal-1-modified cells is potentially a one-time outpatient procedure. For the phase I/II clinical trial, the first major step is to harvest CD4+ T cells by apheresis, isolate these cells, and then activate them before transduction with Cal-1 lentiviral vector. Subsequent to transduction, these cells are expanded in culture to increase the number of HIV-1-resistant cells before reinfusion. The second major step is to administer G-CSF before collection of HSPCs from the patient. CD34+ HSPCs are isolated, activated using cytokines (SCF, Flt-3, and TPO), and similarly transduced with Cal-1. Following cell manufacturing, the two cell populations are separately frozen and tested to ensure genetic modification and sterility. To make bone marrow “space,” the patient is treated with busulfan (4 or 6 mg/kg) thereby enhancing engraftment of transplanted gene-modified cells. This cell manufacturing process is shown in schematic form in Fig. 1. In the Investigator Initiated Study, the first step is ART washout followed by G-CSF administration before HSPC harvest. Only CD34+ HSPCs will be separated, activated, grown (SCF, Flt-3, and TPO), and transduced with Cal-1. Because these subjects have lymphoma, they will receive high-dose conditioning by chemotherapy with BEAM [carmustine (BCNU), etoposide (VP16), cytarabine (Ara-C), and melphalan] or chemoradiotherapy with TBI/CY/VP16 [total body irradiation (TBI), cyclophosphamide (CY), and VP16] before transplant of genetically modified cells.
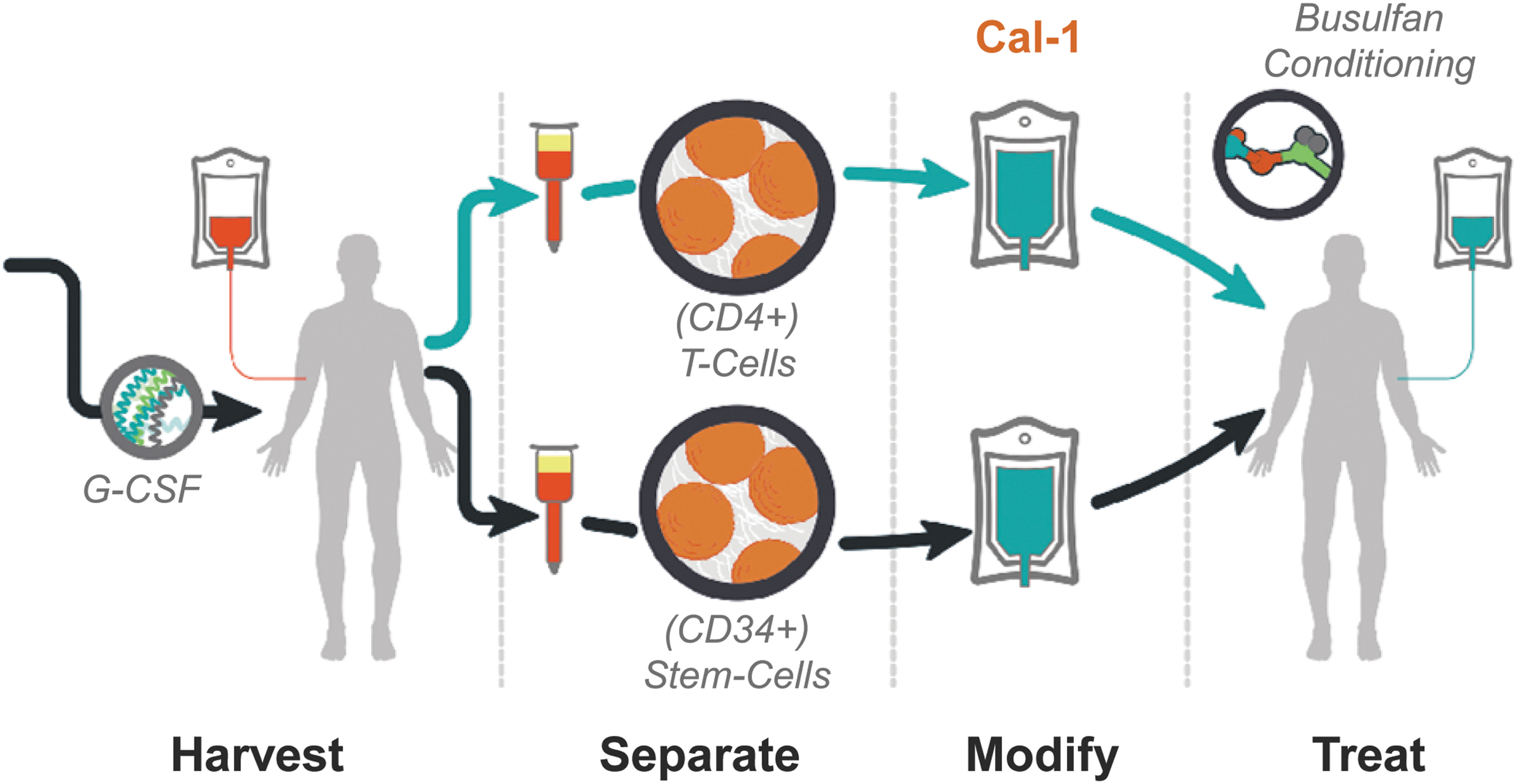
Cell delivered gene therapy process. Cell harvest comprises two aphereses. One before (CD4+ T cells) and one following (CD34+ stem cells) administration of G-CSF. Purified cells (CD4+ T cells and CD34+ stem cells) are transduced with Cal-1. Treatment commences with busulfan conditioning before autologous transplant of both genetically modified cells. G-CSF, granulocyte colony-stimulating factor.
The path to the clinic has involved many steps over several years. Lentiviral vector (Cal-1) production was carried out at small scale and then at good laboratory practice (GLP) and good manufacturing practice (GMP) levels. GLP-grade vector was used in pre-clinical experiments, pharmacology/toxicology studies, and feasibility and potency tests of cell processing. 24,25,33 The total timeline was in the order of 4 years of research and development and the therapeutic approval process followed a regulatory path governed by the National Institutes of Health Recombinant DNA Advisory Committee (NIH RAC) and the US Food and Drug Administration (FDA), including filing an Investigational New Drug (IND) application. The IND comprises the pre-clinical data, the pharm/tox study, the clinical protocol, and the investigator brochure, all with quality assurance overlay.
There are some key considerations that have been taken into account to improve clinical outcomes.
1. First, as noted previously, Cal-1 is a dual therapeutic targeting the host rather than the virus. Cal-1 combination protects against both CCR5 and CXCR4-tropic HIV-1 strains while mitigating development of resistance. Engineering host resistance to HIV-1 allows selection of modified cells.
2. The use of doses (4 or 6 mg/kg) of busulfan conditioning to create bone marrow “space” based on successful dosing in other gene therapy stem cell trials 36 –41 or high-dose conditioning via chemotherapy with BEAM or chemoradiotherapy with TBI/CY/VP16 in the phase I Investigator Initiated Study to treat patients with lymphoma. 35
3. Subjects will have selection pressure from HIV-1. In the Calimmune study, subjects have ceased ART for at least 6 weeks before starting the study, thereby having active HIV-1, which will likely supply selective pressure on transduced cells. In the Investigator Initiated Study, there is the possibility for a structured ART treatment interruption (STI) based on the level of engraftment of genetically modified cells within 18 months post-transplant.
4. The protocols used populations of cells that can provide benefit: CD34+ HSPCs to provide long-term benefit with or without CD4+ T cells to provide short- and medium-term benefit. 16
The Calimmune study (Fig. 2a) involves 12 patients in three cohorts with 4 patients per dosing arm: no conditioning; low-dose busulfan (4 mg/kg); and intermediate-dose busulfan (6 mg/kg). The study design timeline starts with eligibility screening and enrollment (4–14 weeks) followed by CD4 apheresis, mobilization, CD34 apheresis, and transduced cell manufacturing and release testing (6–8 weeks); busulfan conditioning and infusion followed by analysis of end-points last 48 weeks. The primary end-points include safety and feasibility, while secondary end-points include marking and expression in bone marrow and gut-associated lymphoid tissue at 12 weeks, viral load, thymopoiesis, T cell count, and progression of HIV-1 disease.
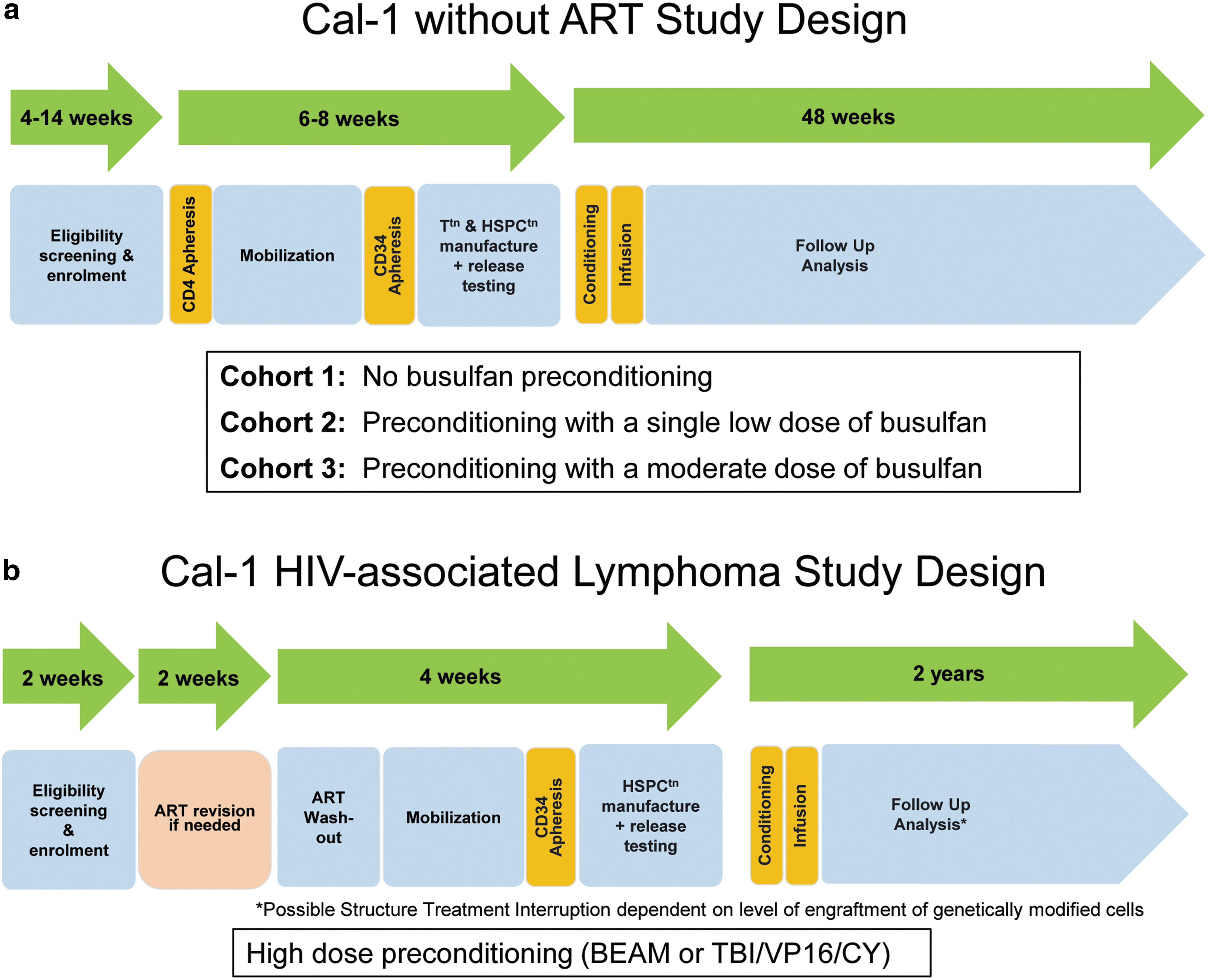
The FHCRC Investigator Initiated Study uses ex vivo gene therapy to modify CD34+ HSPCs in adults with HIV-1-associated non-Hodgkin or Hodgkin lymphoma 35 (Fig. 2b). Up to five patients will be treated and each patient will undergo high-dose conditioning chemotherapy with BEAM or chemoradiotherapy with TI/CY/VP16 as standard of care for high-risk lymphoma. The primary end-points include safety and feasibility with secondary end-points, including marking and expression, viral load, T cell count, and progression of HIV-1 disease. The study design timeline starts with eligibility screening and enrollment (2 weeks) followed by ART revision if needed (2 weeks), and then, 4 weeks for ART washout, mobilization, CD34+ apheresis, and transduced cell manufacturing and release testing. Conditioning and infusion are followed by analysis of end-points out to 2 years.
The near-term clinical development plan for Cal-1 will establish safety and feasibility, determine selection of modified cells, test the level of conditioning necessary to achieve sufficient stem cell engraftment, and determine the level of impact the therapy has on viral load and CD4+ T cell counts. Enrollment of all three cohorts in the Cal-1 phase I/II trial is nearly complete, with no serious adverse events relating to the procedure. The FHCRC Investigator Initiated Study is open and actively recruiting participants. In summary, Cal-1 appears safe and provides strong inhibition of HIV-1 in tissue culture and animal models. Two clinical trials are underway that may indicate a way to provide an alternative paradigm for treating HIV-1/AIDS.
Footnotes
Acknowledgments
Funding for the pre-clinical work on Cal-1 was provided, in part, by Calimmune. Funding for the Calimmune Cal-1 Clinical Trial was provided, in part, by the California Institute of Regenerative Medicine and Calimmune. Funding for the Cal-1 Fred Hutchinson Investigator Initiated Study was provided by Calimmune.
Author Disclosure Statement
The authors G.S., J.B., M.T., and L.B. are employed by Calimmune, Inc.