
Abstract
HIV-associated neurocognitive disorders (HAND) remain frequent even among individuals receiving combined antiretroviral therapy (cART). In addition, HAND may adversely affect the quality of life and adherence to cART. There is scarce epidemiological information about HAND in Latin America. This cross-sectional study recruited HIV-infected patients from a tertiary teaching institution in São Paulo, Brazil, between May 2013 and February 2015. The patients were adults with at least 4 years of education and patients with current neurological or psychiatric diseases were excluded. HAND remain frequent even among individuals receiving cART, use of psychoactive substance, or inability to understand the content for neuropsychological evaluation. We used standardized tools to evaluate depression, use of psychoactive substances, and daily life activities, and we performed a comprehensive neuropsychological examination. HAND was classified using the Frascati criteria. Prevalence of HAND was estimated, and an associated variable of symptomatic HAND was identified by logistic regression. Four-hundred twelve HIV-infected patients were included [male: 281 (68%), mean age of 45.3 years]. Most of them [n = 340 (83.7%)] had an undetectable viral load. The prevalence of HAND was 73.6% (n = 303): 210 (50.9%) had asymptomatic neurocognitive involvement (ANI), 67 (16.2%) had mild neurocognitive disorder (MND), and 26 (6.3%) had HIV-associated dementia (HAD). The univariate logistic regression analysis showed that female gender, age older than 50 years, <11 years of schooling, CD4 count below 200 cells/mm3, presence of previous illnesses (e.g., diabetes, hypertension), opportunistic disease history, and a Beck Depression Inventory (BDI) score between 13 and 19 points were factors associated with symptomatic HAND (MND and HAD). However, a BDI score between 13 and 19 points was the single independent variable associated with symptomatic HAND. HAND was highly prevalent in São Paulo, Brazil, and ANI was the more frequent category of HAND. However, 22.5% of participants had symptomatic HAND. This finding constitutes a challenge in clinical practice. A BDI score between 13 and 19 points was the single independent variable associated with symptomatic HAND.
Introduction
T
HAND categories can be dynamic and bidirectional, and several patterns can now be identified 1,4 –8 making the immune scenario more complex because all HAND categories can be observed in moderate or even discrete immunosuppression levels. 4,9,10 Interestingly, cohort studies of HAND demonstrated the influence of low nadir CD4 counts, but not current CD4 counts or cART duration. 13
HAND may adversely affect the quality of life, 13 outpatient follow-up maintenance, and adherence to cART. 14 Therefore, considering the impact HAND may cause in patients with HIV and the lack of epidemiological information on these complications in Latin America, the purpose of this study is to estimate the prevalence of HAND in São Paulo, Brazil.
Patients and Methods
A cross-sectional study was conducted with outpatients who received follow-up at the Institute of Infectious Diseases Emilio Ribas (IIER), São Paulo, Brazil, between May of 2013 and February of 2015. The IIER is a tertiary teaching institution and referral center for patients with infectious diseases in Brazil.
The patient inclusion criteria were as follows: a serological diagnosis of HIV infection, a minimum of 18 years of age, at least 4 years of education—to avoid an important confounding condition due to lack of schooling—, and the ability to understand and sign the informed consent form to participate in the study.
The exclusion criteria were as follows: diagnosis of opportunistic neurological diseases in activity (e.g., cerebral toxoplasmosis, tuberculous meningitis, cryptococcal meningitis, progressive multifocal leukoencephalopathy), diagnosis of previous cognitive decline due to other types of dementia (e.g., Alzheimer's disease, vascular dementia), current use of psychoactive substance, inability to understand the necessary content for neuropsychological evaluation, coinfections (e.g., hepatitis C, hepatitis B, syphilis), psychiatric disorders (e.g., schizophrenia), and patients who scored higher than 19 (moderate and severe depression degrees) on the Beck Depression Inventory (BDI), because the high incidence of psychologic symptoms among HIV-infected individuals could be confounding the diagnosis of HAND. 15,16
Patients were approached at the IIER outpatient center, where they were invited to participate in the study. Then, the questionnaire to identify the inclusion and exclusion criteria was applied, and afterward, another date was scheduled for neuropsychological assessment and application of the standardized tools.
The clinical, demographic, and laboratory histories were evaluated, an interview was conducted through a structured questionnaire, and medical records as well as laboratory databases were reviewed. The data collected included age, sex, date of HIV infection diagnosis, and transmission mechanism; clinical information on opportunistic and metabolic diseases; antiretroviral drugs history; and laboratory information on CD4+ count, viral load quantification for HIV-1, hemoglobin, hematocrit, urea, creatinine, sodium, potassium, transaminase, lipid profile, and coinfection with hepatitis B or C and syphilis.
HAND diagnosis was established according to the Frascati criteria (ANI, MND, and HAD), 7 and a Z score was also calculated.
The Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST questionnaire) was used to evaluate the use of psychoactive substances. 17 The Lawton questionnaire was used to evaluate daily life activities, 18 and the Beck Depression Inventory (BDI-II) was used to evaluate symptoms of depression. 19
The neuropsychological profile of the patients was determined by formal neuropsychological assessment consisting of the following instruments: (1) Intellectual Functions; subtest Vocabulary and Matrix Reasoning using WAIS-III scale, 20 (2) Attention/Information Processing speed; Trail Making Test A and B 22 and WAIS-III Coding subtest; 20 (3) Memory: Short-term or Operational: Digit Span subtest in direct and indirect order using WAIS-III scale; 20 Immediate and Delayed Hearing capacity: The Rey Auditory Verbal learning test; 21 Immediate and Delayed Visual capacity: Rey Complex Figure Test; 22 (4) Executive functions: Trail Making B; 23 Phonemic Verbal Fluency Test (FAS) 24 and Categorical Verbal Fluency (Animal Naming); 25 (5) Visuospatial and visuoconstructive functions: Rey Complex Figure Test; 22 (6) Motor skills: Grooved Pegboard 26 and Finger Tapping Test. 27 The International HIV Dementia Scale (IHDS) was used for cognitive screening. 28 The choice of neuropsychological battery was made in accordance with the Frascati meeting recommendations. 7
A database was created with the collected data and processed by means of descriptive statistics, with percentage, median, and mean as well as standard deviation calculations. Prevalence of HAND and its categories were estimated. For the neuropsychological performance comparison among groups, variance analyses were performed for independent samples with 1 factor (one-way ANOVA) to identify potential covariates associated with the participants' neuropsychological performance (gender, age, education, and depression). After the establishment of covariates, an analysis of three groups was performed (ANCOVA) to eliminate the effect of these covariates, thereby reducing the variance error. The Bonferroni post hoc test was used to identify statistical differences in pairs of groups. To identify specific risk factors of symptomatic HAND (HAD and MND) prevalence, the variables were dichotomized using the χ 2 test, and p < 0.02 was set as the significance level and evaluated through univariate regression. The evaluation of associated variables to symptomatic HAND was calculated by logistical regression.
All quantitative analyses were performed using SPSS (21.0) and p < 0.05 was set as significance level.
Results
In this study, 1331 HIV-infected persons were screened to participate. Of these, 919 were excluded (Fig. 1).
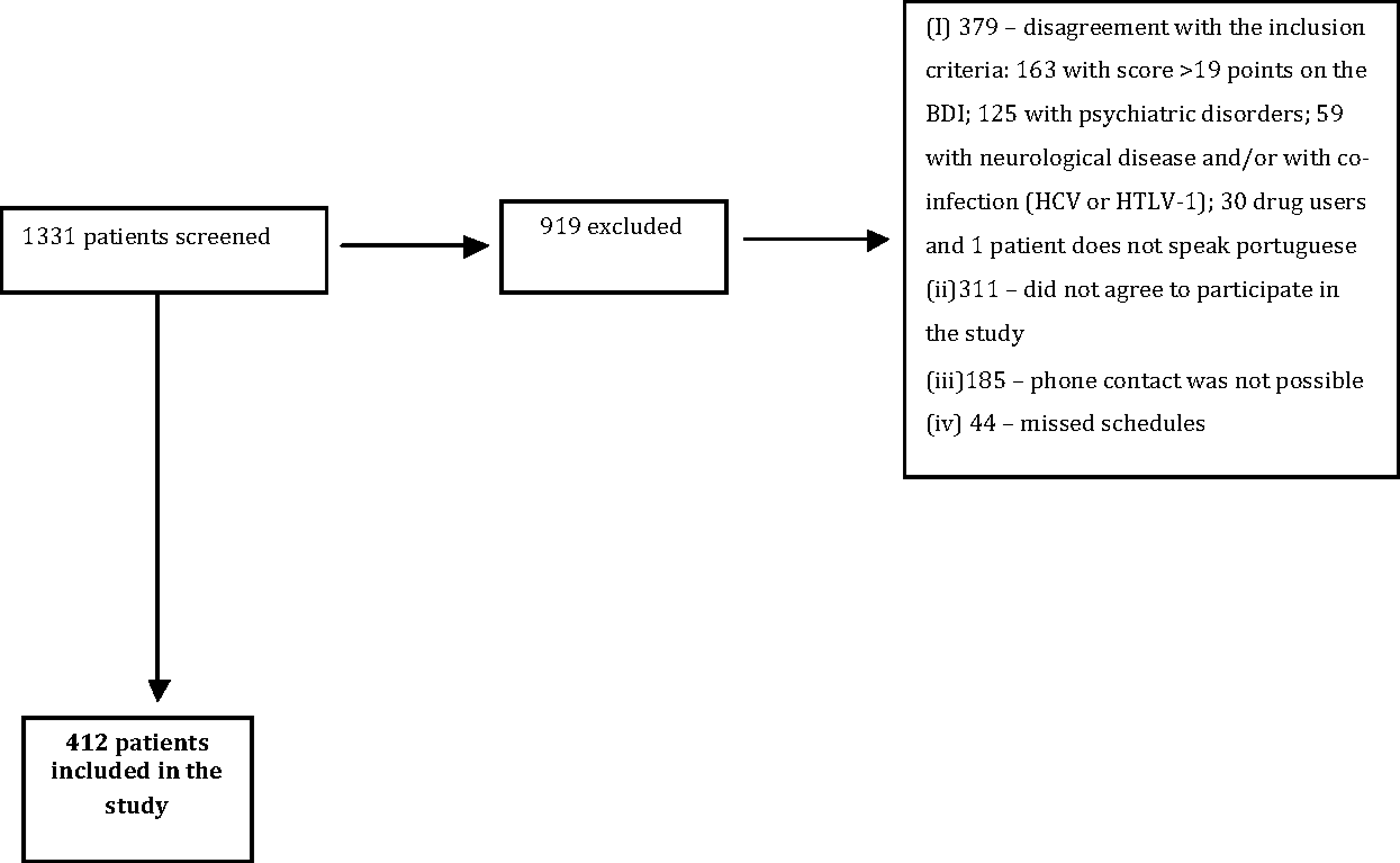
Flowchart of screened, excluded, and included HIV-infected persons. OBS: completar “919 patients excluded,” no lugar de apenas “919 excluded.” Não consigo acrescentar no requadro.
Finally, 412 individuals were included. The sample consisted mostly of male participants 281 (68%), having a mean age of 45.30 years [standard deviation (SD) = 10.70], predominantly single 209 (51.7%) and a mean education of 12.07 (SD = 3.59).
Using the HAND classification criteria, we found 109 participants (26.4%) with normal cognitive performance, 210 participants (50.9%) with ANI, 67 participants (16.2%) with MND, and 26 participants (6.3%) with HAD. The associations that presented statistical significance found in the association for HAND were as follows: female gender (p < 0.01); years of education (p < 0.01); prior opportunistic disease (p = 0.04); and prior disease (p < 0.01). Table 1 shows the demographic and clinical characteristics of the participants, depending on the HAND classification.
Tests applied: Chi-Square*, Kruskal–Wallis.**
ANI, asymptomatic neurocognitive involvement; HAD, HIV-associated dementia; MND, mild neurocognitive disorder.
Demographic data were evaluated, and their statistical association with forms of HAND classification was performed according to the impairment degree, that is, the analysis was performed with the classifications “without neurocognitive changes” and ANI versus MND and HAD. Statistical significance was found between HAND classifications and age (p = 0.04); gender (p = 0.01); years of education (p = 0.04); prior opportunistic disease (p < 0.01); and prior disease (p < 0.01) (Table 2).
Test applied: Chi-Square.
Table 3 shows the laboratorial results, use of efavirenz and BDI score of the participants, depending on the HAND classification. Most patients included in this study showed immunological and virological control. The CD4 mean (SD) was 625.78 (291.09), and 340 (83.7%) of participant had undetectable viral load (Table 3). The majority of patients did not use efavirenz (62.1%), and there was no statistical association between efavirenz use and symptomatic HAND.
Tests applied: *Chi-Square, **Kruskal–Wallis.
Table 4 shows similar variables than Table 3 in grouping the HAND categories (“without neurocognitive changes” and ANI versus MND and HAD). Only BDI score showed statistical difference (p < 0.01).
Test applied: Chi-square.
The univariate logistic regression analysis showed that female gender, age older than 50 years, <11 years of education, presence of prior diseases (e.g., diabetes, hypertension), opportunistic disease history, and a BDI score between 13 and 19 points were variables significantly associated with symptomatic HAND (MND and HAD) (Table 5). However, multiple logistic regression analyses identified that the single variable that remained independently associated with the presence of symptomatic HAND was a BDI score between 13 and 19 points (Table 6).
HAND, HIV-associated neurocognitive disorders.
Model: Y = −2.124 + 1.126*Beck +0.507*Education +0.532*Opportunistic Disease +0468*Gender.
BDI, Beck Depression Inventory.
Discussion
In this study, a high prevalence of HAND was found (73.5%) among 412 outpatients at a referral center in São Paulo, most of them under immunological and virological control. The prevalent HAND categories were as follows: ANI: 50.9%; MND: 16.2%; and HAD: 6.3%. This result confirms that a significant number of patients continue to exhibit measurable cognitive dysfunction in the cART era, despite the fact that Brazil presents a well-structured HIV care program with universal and free access to cART.
High HAND prevalence has also been described in some studies. 1,8 However, lower frequencies have usually been described. A study conducted in the United States among 1555 HIV-infected individuals found a frequency of 47%. 7 Another study conducted in China among 134 HIV-infected patients found a HAND frequency of 37%. 29 In Brazil, the observed frequency of HAND in two studies was around of 50%. 30,31 However, in one of these studies the target public was elderly with HIV, 30 while another study had the objective of validating the IDHS questionnaire. 31
The high frequency of cognitive impairment identified in this study is justified, at least partially, by the neuropsychological battery chosen, as more precise instruments were used to detect cognitive changes. Several studies used IHDS and usually three or four neuropsychological instruments. 28 –32 In this study, in addition to IHDS, we used 12 neuropsychological instruments, which could have increased the sensitivity of the assessment.
In our study, there were a higher proportion of patients with ANI (50.9%). The clinical implications of this HAND category are still controversial and are usually reserved for research. Nevertheless, longitudinal results of the CNS HIV Antiretroviral Therapy Effects Research (CHARTER) showed that patients with ANI at baseline were from 2 to 6 times more likely to develop symptomatic HAND during varying time periods during the follow-up, when compared with those considered normal. 8
One of the variables postulated for this phenomenon is the availability of drugs with different CNS penetration levels. However, we found no statistical differences between the penetration degree of antiretroviral drugs in the CNS and the cognitive impairment degree. Currently, the available evidence supporting the benefit of schemes with better CNS penetration levels is controversial, and recommendations are conflicting. 33 –36 Further studies are necessary before these findings can be translated into clinical practice, but they alert of a potential risk for patients with asymptomatic neurocognitive forms evolving into symptomatic forms.
Nowadays, in contrast to what is observed in developed countries, efavirenz continues to be the preferred drug for first-line therapy in most developing countries. This drug commonly causes early self-limiting neuropsychiatric toxicity and recent studies have highlighted its probable long-term neuropsychiatric effects, including neurocognitive impairment. 36,37 In contrast to this assumption, in the present study, we did not find association between efavirenz and symptomatic HAND.
The diagnoses of less severe forms of HAND (especially ANI) rely on the outcomes of neuropsychological testing, and a high proportion of HIV-infected patients with effective cART may be classified as neurocognitively abnormal, using the Frascati criteria because the definition of ANI is not stringent; and results in between 16% and 21% of the population with HIV diagnosed as asymptomatic cognitive impairment being classified as abnormal. 38,39
In the present study, a BDI score between 13 and 19 points showed statistical significance with symptomatic HAND in multivariate analysis. Within the BDI questionnaire, there are questions that assess concentration difficulties, apathy, and slowness in thinking and solving problems. These same symptoms are usual characteristic of symptomatic HAND. 40 Thus, self-reported symptoms in BDI are consistent to those described in the literature regarding HAND. This finding was also observed in other studies. 38,39
The brain reserve hypothesis has been used to explain the relationship between years of education and dementia risk. 40 It is known that the educational level is directly associated with lower cognitive reserve, thus becoming a risk factor for developing dementia. 41 In our study, an educational level below 11 years was identified in the multivariate model, but there was no statistical significance. Other studies carried out in Africa had already identified an association between education and cognitive dysfunction. 34,42,43
Regarding the history of opportunistic diseases, a variable was also identified in the multivariate model, but that was also not statistically significant, we can postulate that this variable reveals that, at some point in the course of HIV infection, the patient probably had a nadir of CD4 lower than 200 cells/mL. Previous studies have identified that low levels of CD4 nadir is one of the most cited risk factors in the literature for the development of cognitive impairment. 1,2,44 Nevertheless, the presence of some opportunistic infections does not necessarily mean that the CD4 was lower than 200 cells/mL, but it likely indicates poorer immune function in the past.
The other variable identified in the multivariate model was female gender, but it did not demonstrate statistical significance. The literature is conflicting regarding the association between gender and HAND. Some studies reported an association between female gender and HAND. 41 Another study identified that different domains were impaired in men and women. 29 Women, in general, have fewer years of schooling, experience less favorable socioeconomic conditions, are more often exposed to alcohol and substance abuse, and exhibit a higher prevalence of psychiatric disorders, all of which are factors related to poor performance on neuropsychological tests. 29
This study probably reflected the reality of many Brazilian outpatient services, and perhaps the reality in other developing countries, particularly from Latin America. The high prevalence of HAND serves as an alert to healthcare professionals to promptly identify this condition for an appropriate follow-up on these patients.
Normative data from HIV-negative controls were not available, which limited the ability to estimate the prevalence of HAND. Nevertheless, we used the normative data of the Brazilian population. Neuropsychological assessment involves the intensive study of behavior through interviews, questionnaires, and standardized tests that allow relatively precise performances.
In summary, this is the largest study performed in low- and middle-income settings of prevalence of HAND and associated factors of symptomatic HAND. Neurocognitive disorders were highly prevalent in São Paulo, Brazil. Although ANI was the more frequent category of HAND, 22.5% of participants had symptomatic HAND. This finding constitutes a challenge in clinical practice. A BDI score between 13 and 19 points was the single independent variable associated with symptomatic HAND.
Footnotes
Acknowledgments
The authors thank the Department of STD/AIDS and Viral Hepatitis of the Ministry of Health of Brazil, and Center for Psycho-surgical Studies (CEPSIC), for providing financial support for this study.
Author Disclosure Statement
No competing financial interests exist.