
Abstract
The Max Clinic in Seattle, Washington is designed to engage patients who have extensive barriers to HIV care. In this article, we describe the clinic's evolution and outcomes of patients enrolled in the first 2 years. The clinic is a high-intensity, low-threshold, incentivized care model that includes walk-in access to primary care in a Sexually Transmitted Disease Clinic. Patients who have failed to engage in care and achieve viral suppression with lower intensity support are referred by clinicians, case managers, and the health department Data to Care program. The clinic offers food vouchers, cash incentives, no-cost bus passes, and cell phones, as well as intensive case management with cross-agency coordinated care. The primary evaluation outcome was the percentage of patients who achieved viral suppression (HIV RNA <200 copies/mL) at least once after enrollment. Secondary outcomes were continuous viral suppression (≥2 suppressed results in a row ≥60 days apart) and engagement in care (≥2 completed medical visits ≥60 days apart). During January 2015–December 2016, 263 patients were referred; 170 (65%) were eligible, and 95 (56% of eligible) were enrolled. Most patients used illicit drugs or hazardous levels of alcohol (86%) and had diagnosed psychiatric illness (72%) and unstable housing (65%). During the year after enrollment, 90 (95%) patients engaged in care. As of the end of 2016, 76 (80%) had achieved viral suppression, and 54% had continuous viral suppression. The Max Clinic successfully treated HIV in high-need patients and, to date, has been sustainable through a combination of federal, state, and local funding.
Introduction
M
Healthcare systems factors are commonly identified as barriers to HIV care. 4 –6 Obstacles such as limited appointment availability, the need for advanced scheduling, and appointment start times with limited flexibility require patients to be organized and familiar with the healthcare system to navigate successfully. For some patients with extensive psychosocial barriers to care—particularly those with substance use disorders, unstable housing, and inadequately treated mental illness—these barriers can be insurmountable, and engagement in HIV care as it is currently organized is simply not a realistic goal.
We developed the Max Clinic (“Maximum assistance” clinic) with the goal of engaging the hardest-to-reach PLWH by reducing healthcare systems barriers to care. We undertook this work after implementing and evaluating two strategies to reengage patients in HIV care that proved to be ineffective. The first was a health department Data to Care intervention 4,7,8 that showed no impact on relinkage to care or viral suppression in a randomized controlled evaluation. 8 The second was a clinic-based patient retracing strategy that improved relinkage to care compared to a historical control, 9 but the effect size was small (15% vs. 10%), and the intervention did not significantly impact viral suppression. Based on these experiences, we concluded that strategies focused on relinking patients to the same healthcare system that failed to engage them in the first place are unlikely to make a substantial public health impact. Further, in the context of high rates of viral suppression in Seattle & King County (81% of HIV-diagnosed individuals), 10 we recognized that more intensive interventions would be needed to engage the most vulnerable patients. In designing a new strategy to increase viral suppression, we reasoned that no single intervention was likely to have a meaningful impact, and that a more effective intervention would include an array of interventions and a fundamentally different model of care delivery. In this article, we describe the Max Clinic model and report the results of a descriptive analysis of patients enrolled in the first 2 years of the program.
Methods
Intervention components
Care at the Max Clinic includes high-intensity support, low-threshold access, and incentives for retention in care and viral suppression. The clinic is comanaged by the Public Health–Seattle & King County (PHSKC) HIV/STD Program and the Harborview Medical Center (HMC) Madison (HIV) Clinic. Key components include walk-in access to primary care in the public health sexually transmitted diseases (STD) clinic, walk-in access to intensive coordinated case management, food vouchers, no-cost bus passes, cell phones, and financial incentives for visits with blood draws, as well as achieving/maintaining viral suppression. As summarized in Table 1, the clinic substantially expanded over the first 2 years of operation.
The HMC Madison Clinic is a Ryan White Part C funded clinic housed within a medical center that is owned by King County government with medical staff from the University of Washington. HMC resources include a combination of Ryan White funds, local King County government funding, and funding from the UW.
HMC, Harborview Medical Center; ID, infectious disease.
Cross-agency care and case management coordination
The Max Clinic relies on the resources of HMC, the University of Washington (UW), and other organizations in the community. The clinic is administratively part of HMC Madison Clinic, but physically located within the STD Clinic on the HMC campus, a public hospital that offers comprehensive specialty medical and surgical specialty services. The Madison Clinic, funded in part by Ryan White Part C, includes HIV medical and case management services, a specialized HIV pharmacy, and subspecialty care.
Coordination between multiple service providers is a key part of the Max Clinic. Collaborating organizations include the Bailey-Boushay House Outpatient Program that provides medication adherence support and other resources to vulnerable PLWH in King County; housing support based at an AIDS Service Organization; the county jail release planning program; the HIV Enhanced Engagement Team, which provides intensive outreach support for PLWH who have substance use disorders, mental illness, and recent incarceration; organizations providing support services to homeless persons; and supportive housing facilities (and close coordination between inpatient staff at hospitals in the UW/HMC system).
High-intensity outreach
The “high intensity” approach of the Max Clinic model includes intensive patient support and outreach from nonmedical and medical case managers. A team of public health disease intervention specialists (DIS) coordinate the clinic, conduct outreach, and serve as a single point of contact for patients and service providers to facilitate care coordination. They are available to patients and service providers via one phone number that is directly answered without a phone tree and can receive text messages. The DIS receive automated text message alerts when Max Clinic patients present to an emergency department or are admitted to an inpatient hospital within the UW Medicine system. Medical case managers in the clinic provide intensive case management, including housing assistance and active referrals to mental health and substance use treatment services, at a ratio of ∼50 patients per case manager.
Low-threshold, incentivized care
The “low-threshold” aspect of the clinic includes minimal requirements for patients to access care, ART, and case management. A team of Infectious Disease physicians provides primary and urgent care on a walk-in basis five afternoons per week. Patients can access Max case managers (medical and nonmedical) on a walk-in basis five full days per week. The physicians provide buprenorphine treatment in coordination with the HMC nurse-managed office-based opioid treatment team, and hepatitis C treatment in coordination with the Madison Clinic pharmacy team. The Max Clinic team takes a harm-reduction approach to substance use; abstinence is not required for any services, including buprenorphine treatment and hepatitis C therapy. All patients are offered ART regardless of their adherence history, and in most instances start treatment on the day of their enrollment in the Max Clinic.
We designed the incentive strategy (Table 1) with the goal of increasing the priority of clinic visits for patients' in the context of competing needs (e.g., food and shelter) and providing a contingency management approach for completing laboratory orders and achieving viral suppression. To facilitate communication with patients, Max Clinic patients who do not have cell phones or active service plans can receive a program-funded cell phone. All clinic incentives are optional.
Patient eligibility and referral
Patients are eligible for the Max Clinic if they were not virally suppressed [i.e., viral load (VL) >200 copies/mL] at the time of last VL measurement or are no longer taking ART and have failed to engage in care and achieve viral suppression after lower intensity outreach and support. In King County, the lower intensity outreach includes health department and clinic-based relinkage programs described in detail elsewhere. 4,9 The Max Clinic team identifies candidates for enrollment through case manager and medical provider referrals, public health HIV/STD partner services, systematic review of clients who fail to engage in care after participating in the health department Data-to-Care program, and an automated information exchange with UW Medicine to identify poorly engaged PLWH who are admitted to the hospital or present to the HMC or UW ED. Although not planned, peer and self-referral of patients to the Max Clinic began in the first few months of its operation.
All Max Clinic referrals are reviewed by a medical provider, DIS, and medical case manager. If referred patients have recently completed a provider visit and appear to be engaging in traditional medical care, they are placed on a deferred decision (“watch”) list. For accepted referrals the Max team communicates with the primary care provider and case manager to determine whether they agree with transferring the patient's care to the Max Clinic. Once a referral is accepted, the nonmedical case managers attempt to contact patients by phone or when they appear in the hospital, ER or Madison Clinic. Case managers also contact community case managers and organizations where patients have received services to coordinate enrollment in the clinic.
Analysis
The goals of this analysis were to describe patient referrals to the Max Clinic during the first 2 years of the program (January 2015–December 2016) and to describe the characteristics, retention, and HIV health outcomes of enrolled patients.
Data sources
Max Clinic patients enrolled during the first 2 years were enumerated and identified through a combination of CareWare (a HRSA-funded database) and a Max Clinic database. For the purposes of this analysis, we defined the enrollment date as the date of the first completed visit at the clinic. We extracted data from the Madison Clinic electronic database for all enrolled patients, including all available CD4 counts, viral loads, and completed visits with medical providers. We conducted a chart review of electronic health records to obtain demographic information, substance use history, mental health history, housing status, and incarceration history. All these outcomes were defined as of the enrollment date in the Max Clinic, including data noted before enrollment or during intake.
Variable definitions
To describe the HIV stage of Max Clinic patients, we identified the CD4 at enrollment, defined as the most recent CD4 in the year before enrollment or, for patients with no CD4 history, the first CD4 measurement on or after enrollment. We categorized patients according to CDC staging, using the most recent CD4 count rather than the nadir CD4 count. We identified the most recent viral load within the past year at the time of enrollment and defined viral suppression dichotomously as <200 copies/mL (suppressed) or ≥200 copies/mL (unsuppressed), consistent with the CDC definition of viral suppression used for the HIV care continuum. 1
We defined substance use within the past year at the time of enrollment and mental illness as any history of psychiatric diagnoses noted in the chart. We categorized both these variables in a mutually exclusive, hierarchical manner using an adapted version of a previously validated approach. 11 We defined substance use hierarchy as follows: methamphetamine (with or without other substances); opioids (with or without cocaine, unhealthy alcohol use, or marijuana); cocaine (with or without unhealthy alcohol use or marijuana); unhealthy alcohol use (with or without marijuana); marijuana; or none of the above. Because methamphetamine use is the most commonly used substance in the population and the substance most strongly associated with HIV risk and outcomes in Seattle & King County, we began the hierarchy with methamphetamine instead of opioid use. Based on the validated definition, 11 we defined mental illness as bipolar disorder or personality disorder (with or without depression, anxiety or other diagnoses); depression or anxiety; or none of the above. We categorized housing as either stably housed, transitionally housed, unstably housed (medical motel, couch-surfing), or homeless.
For the evaluation of HIV health outcomes, we included all patients ever enrolled in the Max Clinic, regardless of whether they remained enrolled or actively engaged in the clinic at the end of 2016. The primary outcome of our evaluation was achieving viral suppression (HIV RNA <200 copies/mL) at least once after enrollment, before December 31, 2016. We analyzed this among all patients enrolled and stratified the analysis by the time since enrollment in the Max Clinic in 3 month intervals up to 18 months, restricting each period to patients who had been enrolled for the length of interval or longer. We defined patients with no VL in the analysis period as unsuppressed. Before implementation of the Max Clinic, we estimated that 33% of patients would achieve viral suppression within 9 months of enrollment.
Secondary outcomes included engagement in care (≥2 completed medical visits ≥60 days apart) and continuous viral suppression (≥2 suppressed HIV RNA results in a row ≥60 days apart) in the year after enrollment. Our rationale for using these metrics was that they aligned with specific goals of the Max Clinic (visits with laboratory measurements every 2 months for all patients), and the definition of engagement in care is consistent with the federal agency consensus metric for retention in care. 12 We also conducted a cross-sectional analysis of care engagement and viral suppression at the time of last report at the end of 2016 to provide a cross-sectional description of viral suppression in the population consistent with the usual approach to describing the HIV care continuum in a population. 1 Finally, we evaluated the mean increase in CD4 count from the time of enrollment to the time of the last available CD4 count among all patients at the end of 2016.
Results
From January 2015 to December 2016, 263 unique patients were referred to the Max Clinic. As shown in Fig. 1, 93 (35%) patients were excluded, most often because they were not eligible due to having a suppressed VL and taking ART, despite not consistently completing HIV primary care appointments, or because they were not virally suppressed but were otherwise well-engaged in primary HIV medical care (N = 53). An additional 31 patients had not yet received standard-of-care outreach assistance to engage in HIV care and were thus assigned to the lower intensity assistance group or the “watch” group. Six patients were excluded due to a history of violent behavior toward staff, and three were excluded based on the preference on their primary care providers after referral from another source. Of the 170 referred patients who were eligible for the Max Clinic, 95 (59%) had enrolled by the end of 2016, 50 (31%) were being actively recruited, and 22 (13%) did not complete enrollment due to patient refusal, relocation, disability requiring assisted living, or incarceration in prison.
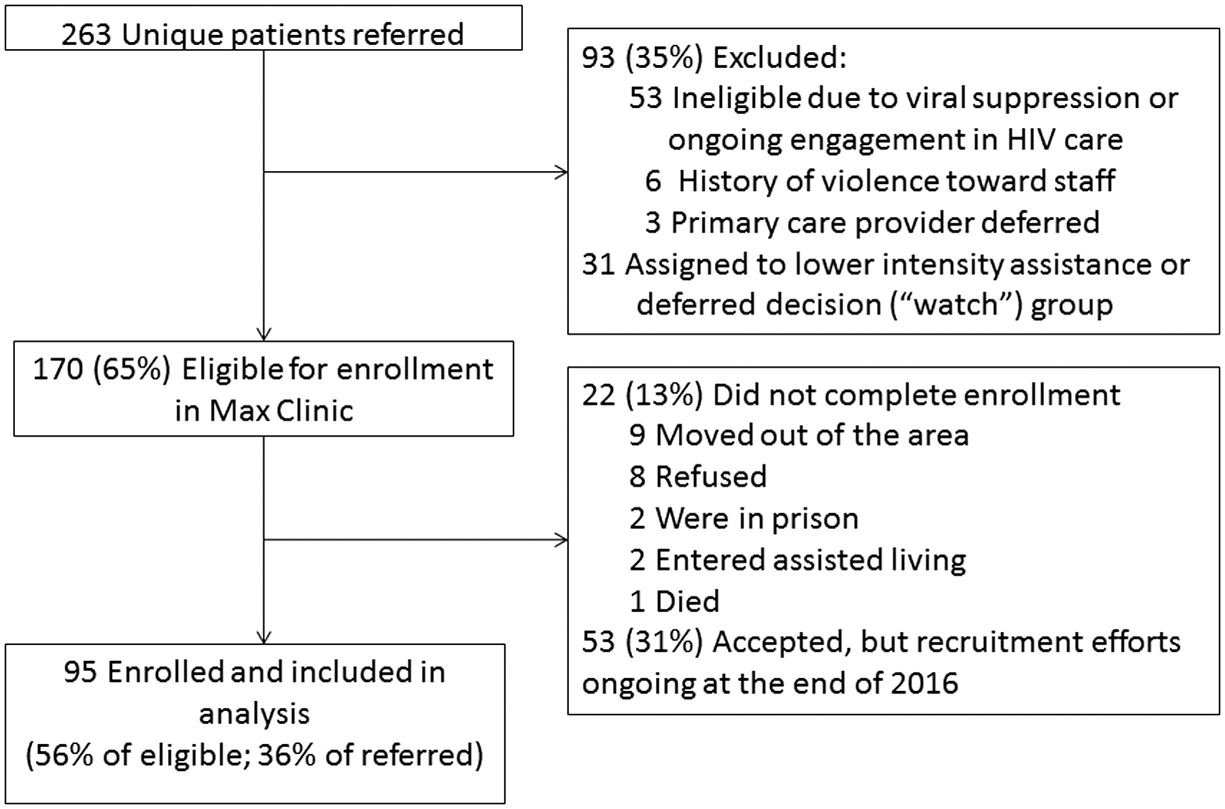
Flowchart of Max Clinic referrals, January 2015–December 2016.
Table 2 summarizes the characteristics of the 95 enrolled patients. The percentage of Max Clinic patients who were female was higher than that in the overall population of HIV-diagnosed persons in King County at the end of 2016 13 (23% vs. 12%, p < 0.001) as was the proportion who identified as transgender (5% vs. <1%, p < 0.001), although countywide surveillance data have not consistently captured gender identity information. The race and ethnicity distribution varied from that in the overall HIV-diagnosed population, with proportionately more American Indian or Alaskan Native (AIAN) patients (7% vs. 1%, p < 0.001) and proportionately fewer Hispanic patients (4% vs. 13%, p = 0.01) in the Max Clinic. Most patients were referred by a medical provider or case manager (51%) followed by health department staff (26%), an inpatient medical team (9%) or inpatient alert from the health information exchange (6%), and peer or self-referral (7%).
Nearly half of the patients (46%) had a most recent CD4 count <200 cells/mm3 at the time of enrollment, and among the 60 patients (63%) with a CD4 count in the past year, the median was 165 (IQR: 52–384) cells/mm3. Among the 59 patients (62%) with at least one VL in past year, the median viral load was 14,970 (IQR: 889–89,660) copies/mL. An additional 13 (14%) patients had a VL <200 at the time of last measurement within the past year. These patients had either discontinued ART in the interim, achieved viral suppression during an inpatient hospitalization during which ART was started concurrent with the referral to the Max Clinic, or were enrolled on a case-by-case exception to enrollment criteria due to extenuating circumstances. A large majority of patients (86%) were actively using substances other than marijuana at the time of enrollment, most commonly methamphetamine (59%). Psychiatric illness was common (71%)—including 27% with psychotic, bipolar, or personality disorders–as was homelessness or unstable housing (65%). Only 5% (N = 5) of Max Clinic patients were not affected by unstable housing, psychiatric illness, or substance use; 45% of patients were affected by all three factors. Most patients (58%) had a history of incarceration noted on chart review.
At the end of 2016, 91 (96%) patients remained enrolled in the MAX Clinic; three moved, one died, and one patient was unenrolled for threatening staff. Patients had been enrolled a median of 423 [interquartile range (IQR) 289–560 days]. By the end of 2016, 76 (80%) of all 95 patients enrolled achieved viral suppression at least once; 51% within 6 months and 66% within 9 months after enrollment (Fig. 2
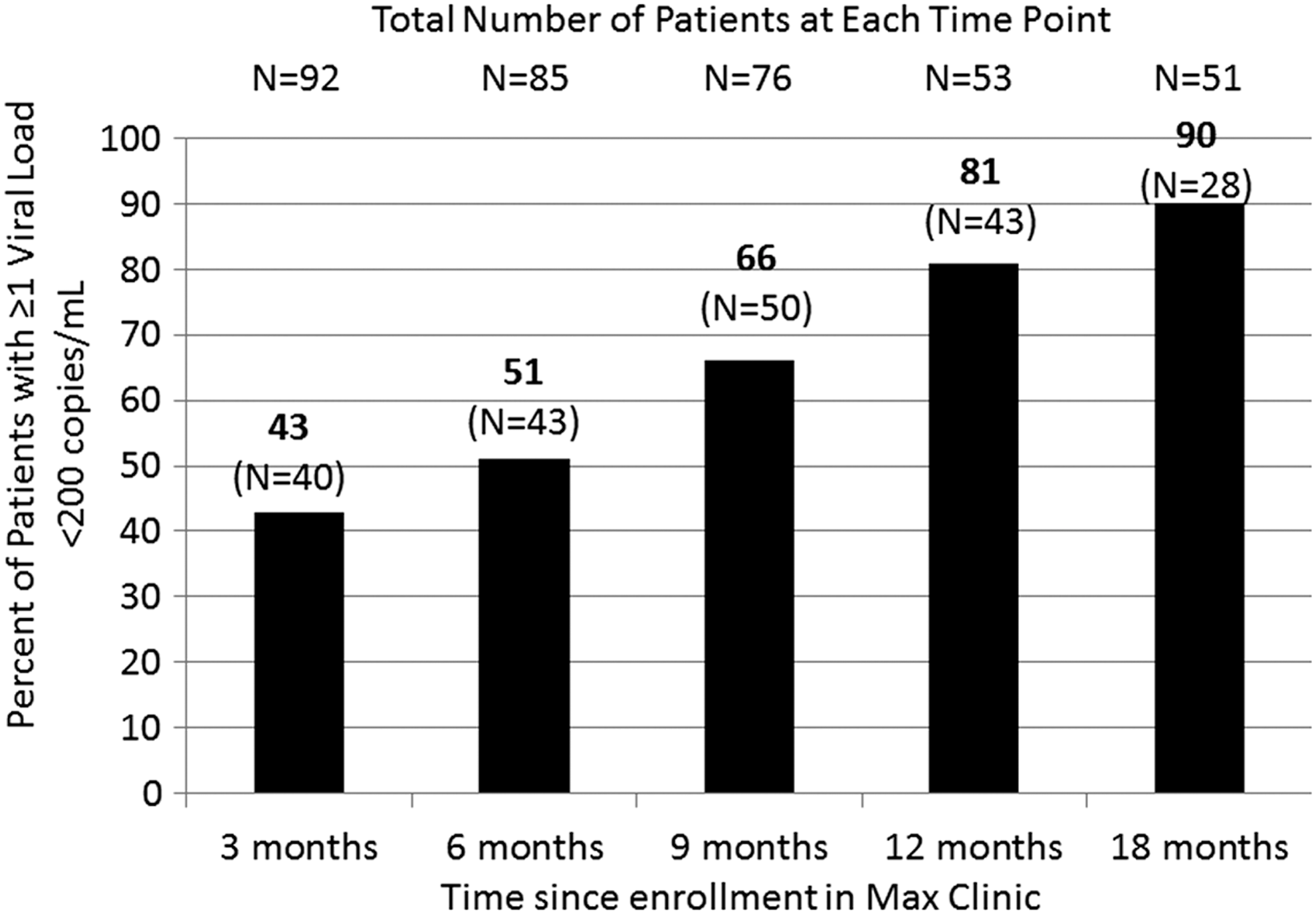
Timing of viral suppression after Max Clinic enrollment among patients enrolled January 2015–December 2016 (N = 95).
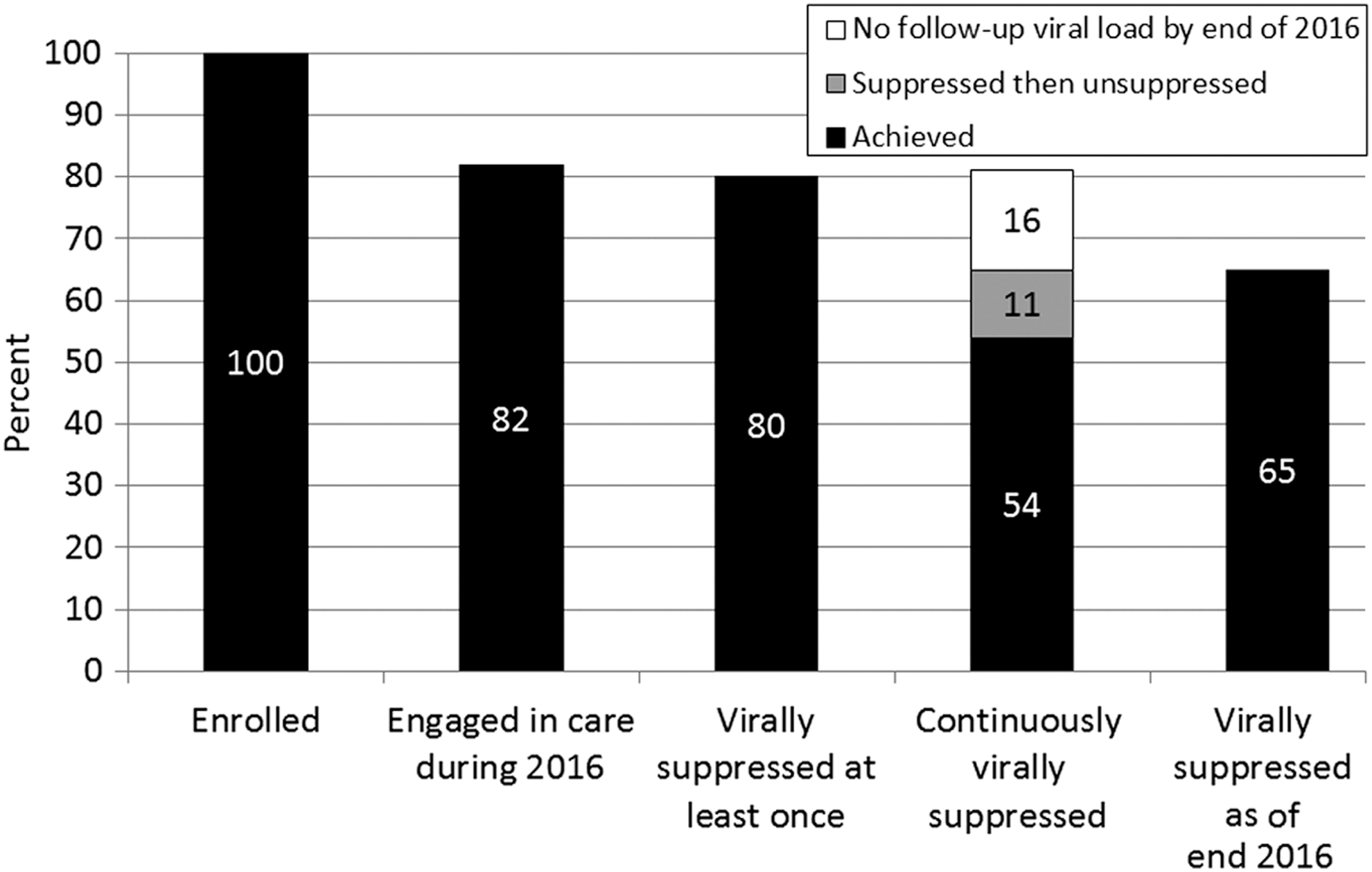
Care engagement and viral suppression outcomes as of January 31, 2016 among patients enrolled January 2015–December 2016 (N = 95).
Discussion
We designed the Max Clinic to engage high-need, complex patients who had not engaged in traditional HIV medical care. Our approach evolved substantially over the first 2 years of the clinic's operation to include additional staff and increased coordination with other agencies serving the same patient population. The principal finding of our descriptive analysis is that the majority (80%) of the 95 patients enrolled in the first 2 years of the clinic's operation achieved viral suppression by the end of 2016, exceeding our expectations (66% observed vs. 33% expected by 9 months postenrollment). Most patients had complex comorbidities and barriers to care: 86% used hazardous levels of alcohol or illicit substances other than marijuana; 72% had a diagnosed psychiatric illness, and 65% were either homeless or had unstable housing.
This primary strength of this report is that it describes a novel intervention designed for high-need, out-of-care PLWH and demonstrates an approach that successfully engages patients. To date, all elements of the clinic have been sustainable through a combination of federal, state, and local funding. Although the financial incentives, snacks, bus passes, and cell phones were initially supported by research funding, the support for each of these has been successfully transferred to a nonresearch source from state or local funds. A primary limitation of our analysis is that it was not controlled. Further, we implemented this intervention at a single site, and the generalizability of our results is uncertain. We focused our analysis on patients who were successfully recruited into Max Clinic, but we did not recruit all referred eligible patients (50 [31%] referred patients not enrolled). We did not analyze the nonmedical visits to Max Clinic in this analysis, which were substantially more frequent than medical visits, nor did we track staff effort in sufficient detail to report the time involved in achieving the observed outcomes. However, it is clear that the Max Clinic is a resource-intensive effort since it currently requires DIS, case manager, and physician effort plus the costs of the financial incentives, food vouchers, transportation, and cell phones. Even with these limitations, our experience is informative and our results are encouraging. Interventions to improve viral suppression among hard-to-reach patients are badly needed, and our report describes one potentially effective approach.
There are few evidence-based interventions to improve engagement in HIV care available in the literature, 14 and those described have been limited in their ability to successfully contact and reengage patients who are truly disengaged from medical care. Health department Data to Care efforts have been limited by inaccuracies in HIV surveillance data and low levels of successful contact with individual PLWH. 8,15 –18 Moreover, most Data to Care interventions focus on relinkage to care (completing one visit) rather than achieving sustained engagement in care or achieving viral suppression. Several reports describe care coordination and case management approaches to engaging hard-to-reach PLWH. 19 –21 The Max Clinic is distinct from these approaches because it offers a fundamentally different structure of care to a relatively small subset of patients. To our knowledge, the approach of coupling a low-threshold, open-access clinic with intensive case management for PLWH has not been well-described in the literature, but this approach certainly exists in practice. For example, two HIV clinics in Vancouver, British Columbia provide low-threshold open-access HIV care [the Maximally Assisted Therapy (MAT) Program of Vancouver Coastal Health and the British Columbia Centre for Excellence in HIV/AIDS and the Vancouver Native Health Society].
The Max Clinic incorporates cash incentives as one strategy for engaging patients. Previous research on financial incentives to support patient engagement in the HIV care continuum 22 has shown that such incentives can increase viral suppression, although that effect is often small. The HIV Prevention Trials Network 065 (TLC-Plus) study provided financial incentives for viral suppression to all patients testing HIV positive at multiple sites in the Bronx, NY, and in Washington DC and found that incentives increased viral suppression among persons who had not been previously consistently virally suppressed by 4.9%. 23 The Project HOPE trial enrolled a more selected population of substance-using, unsuppressed hospitalized patients and provided them with financial incentives couple with multi-session navigation services; 24 this intervention increased viral suppression 11% relative to usual care, although that effect was not sustained once the financial incentives were withdrawn. Similar to Project HOPE, the Max Clinic enrolls a highly selected, difficult to treat populations. It provides them with an intervention that is much more intensive than has been previously studied in trials of financial incentives. Although not a randomized controlled trial, the prepost effect size we observed in this study was large relative to that reported in prior studies. We believe that our findings are consistent with prior reports and suggest that financial incentives are best used as part of a comprehensive package of interventions provided to selected high-need patients.
The challenge of engaging high-need patients is not unique to HIV care or to the United States, although the structure of the US healthcare system poses some unique challenges to service delivery and care coordination for vulnerable patients. In a large survey of primary care physicians in 10 countries, US doctors were among the least likely to report that their practice was well prepared to manage the care of patients with multiple chronic conditions, severe mental health problems, and substance use-related issues. 25 The Camden Coalition model is one approach to caring for patients with extensive medical and social needs, 26 which provides primary care for healthcare “super-utilizers” using an intensive, multi-disciplinary team-based intervention. The objectives of the Max Clinic differ somewhat from this approach and similar models focused on reducing hospital readmissions, in which cost reduction is a primary outcome. Many of the Max Clinic patients were not super-utilizers of healthcare. On the contrary, they were almost entirely disengaged from the healthcare system, at risk for death and, in some instances, at risk of transmitting HIV to others. Engaging Max Clinic patients is resource-intensive. Whether this approach could be cost-effective in the long-term is uncertain, but it is not likely to be cost-saving. King County's current goal is to achieve 90% viral suppression among diagnosed PLWH. Inherent in the commitment to reach that goal is a willingness to pay a premium to effectively care for the most vulnerable populations.
Our results have implications for both HIV care providers and public health HIV programs. Despite 80% of patients in the Max Clinic achieving viral suppression at least once, fewer had continuous viral suppression (54%) or were suppressed at the end of 2016 (65%). Maintaining suppression is more difficult than achieving it once and surmounting barriers to care and treatment is not a one-time event. Periodic, sometimes cyclical, disruptions in patient's life, such as loss of housing, incarceration, substance use relapse, and relationship dissolution, pose repeated challenges to care and medication adherence. Max Clinic patients visit with case managers much more frequently than they complete medical visits with the doctors, and many attend the clinic on a near weekly basis. Our findings are relevant to health departments because our experience, in the context of previous reports, suggests that alternate structures of HIV care for high-need, out-of-care PLWH are a key component of Data to Care efforts. While the Data to Care approach in King County once focused entirely on relinking patients to their previous HIV care provider—an approach that we found to be unsuccessful—our strategy has evolved to focus on a spectrum of patient needs.
In summary, we have demonstrated that a model of low-threshold, high-intensity support with incentivized care can effectively engage hard-to-reach patients with HIV. Future research will include a controlled analysis and a qualitative study to assess patient perceptions of each of the components of the clinic. In addition, research is needed to evaluate strategies that can be adapted to environments with fewer resources than King County, Washington and understanding what factors predict success within this model.
Footnotes
Acknowledgments
The authors acknowledge Chris Bell for data management assistance, Megan Touhey for chart review; the Max Clinic and HIV care relinkage team (Rachel Patrick, Mark Fleming, Angela Nunez, Mike Nicholson, and Katherine Lincicum), and our many collaborators in Seattle & King County working with the Max Clinic patients. We also acknowledge the Seattle Transitional Grant Area (TGA) Planning Council, the Ryan White Part A & B programs in Seattle & Washington State, and the WA State Department of Health, and Madison Clinic and pharmacy leadership (Pegi Fina, Reid Branson, Ji Lee, Bob) who have been instrumental in the Max Clinic.
Funding
This work was supported by a grant to J.C.D. from the National Institute on Drug Abuse (R03 DA 042668); the University of Washington Center for AIDS Research (CFAR), an NIH funded program under award number P30AI027757 which is supported by the following NIH Institutes and Centers (NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS, NIDDK); a CFAR supplemental grant (P30 AI 027757-28S1) and programmatic funding from the Health Resources & Services Administration to Public Health–Seattle & King County and the Washington State Department of Health and from the Centers for Disease Control and Prevention to the Washington State Department of Health.
Author Disclosure Statement
J.C.D. has conducted research unrelated to this work supported by grants to the U.W. from the following companies: Hologic, Genentech, Curatek Pharmaceuticals, ELITech and the Quidel Corporation. J.C.D. received an honorarium for speaking at a continuing medical education event on retention in HIV care sponsored by Gilead and attended a meeting on retention in HIV care sponsored by Gilead. All other authors have no competing financial interests exist.