
Abstract
Adolescents represent a growing proportion of people living with HIV worldwide and the highest risk population group for treatment attrition and AIDS-related mortality. There is an urgent need to design, implement, and test interventions that keep young people in HIV treatment and care. However, previous systematic reviews show scarce and inconclusive evidence of effective interventions for this age group. Recent years have seen an increase in focus on adolescent health and a rapidly changing programmatic environment. This systematic review article provides an evidence update by synthesizing empirical evaluations of interventions designed to improve antiretroviral therapy adherence and retention among adolescents (10–19) and youth (15–24) living with HIV, published between January 2016 and June 2018. A search of 11 health and humanities databases generated 2425 citations and 10 relevant studies, the large majority conducted in sub-Saharan Africa. These include six clinic-level interventions, one individual-level m-Health trial, and three community- or household-level interventions. Implications of their findings for future programming and research with young adults are discussed, in relation to previous reviews and the broader empirical evidence in this area. Findings highlight the need to further develop and test multi-faceted interventions that go beyond health facilities, to address broader social barriers to adherence and retention. In particular, further intervention studies with adolescents (10–19) should be a priority, if we are to retain these young people in treatment and care and aspire to achieve the United Nation's Sustainable Development Goals and 90-90-90 targets.
Introduction
The focus on treatment and care for adolescents living with HIV has increased considerably in recent years, and with good reason. The number of adolescents living with HIV globally is around 1.8 million and growing, as a result of children with perinatally acquired HIV surviving into adolescence and high rates of adolescent HIV infection. 1,2 This is especially the case in low- and middle-income countries (LMICs) highly affected by the epidemic; ∼1.5 million or 85% of HIV-positive adolescents live in sub-Saharan Africa. 2
Adolescents have the highest rates of attrition and loss to follow-up (LTFU) for HIV treatment and care at all stages of the treatment cascade. 3 –5 As a result they are a high-risk population group for onward HIV transmission and AIDS-related mortality; in fact youth, 13–24 years of age represent the only population group with increasing AIDS-related mortality rates. 6
The greater likelihood of detachment from health care among adolescents living with HIV may be partly explained by their unique psychological and medical needs 7 –9 ; in particular, adolescents perinatally infected with HIV may face additional health and developmental challenges. 1,10 It is clear that reaching the United Nation's health-related Sustainable Development Goals (SDGs) and 90-90-90 2020 treatment targets 11,12 is going to be particularly challenging in this population group, unless we develop more effective and scalable approaches to increase timely HIV treatment initiation, and ensure treatment adherence and retention. There is an urgent need to design, implement, and test interventions and services that are effective at keeping young people in treatment and care, by responding to their particular risks and needs.
However, to date, the programmatic evidence on what works for this age group has been scarce. This is highlighted by a number of—in part overlapping—systematic reviews on interventions for antiretroviral therapy (ART) initiation, adherence, and retention, published over the past 4 years. These review articles provide a useful synthesis of the state of the evidence up until 2015. Some did not specifically focus on youth or adolescents, but included studies with adolescents within a broader population of adults and children. 13,14 Moreover, most of these reviews limited their foci to specific types of interventions, for example, service delivery at health facilities, 15 subgroups of adolescents, for example, vertically infected adolescents 16 or groups of countries, for example, LMICs. 13,14
MacPherson et al. reviewed studies published between January 2001 and June 2014, evaluating the effectiveness of service delivery interventions to improve linkage from HIV diagnosis to ART initiation, retention in care and adherence to treatment for adolescents (10–19 years of age) living with HIV. 15 The authors concluded that interventions such as individual and group education and counseling, financial incentives, youth-friendly clinic services, and increased accessibility to clinics showed promise; however, given the limited number (11) and low-to-moderate methodological quality of available studies, these approaches required further investigation. Moreover, most (8 out of 11) studies reviewed were conducted in high-income countries (HICs) and not in countries with generalized HIV epidemics. 15
Two subsequent review articles, published in 2016, reinforced the potential effectiveness of phone-based, individual and family counseling approaches for ART adherence among youth 13–24 years of age, 17 and interventions, such as psychosocial and peer support, and financial incentives, specifically for perinatally infected adolescents. 16 Similar to the article by MacPherson et al., both 2016 reviews highlighted the predominance of studies deriving from HICs, mainly the United States, and the limited ability to generalize results from the low number of studies with small sample sizes and short follow-up periods. 16,17 Moreover, Judd et al. exposed a gap in studies focusing on the transition period from pediatric to adult care, which appears to be the most vulnerable time for LTFU and nonadherence. 3,16
Two more recent systematic reviews report interventions to improve retention 13 and ART adherence 14 among adolescents and adults in LMICs; these include studies published during the 5 years between November 2010 and November 2015. Despite a specific interest in adolescents, these reviews found only four studies conducted with or disaggregating data for the 10–24 age group. Only two pilot studies—one working with adolescents 10–1318 and the other with youth 15–2419—pointed to the potential effectiveness of group counseling for adherence, incorporating HIV and ART information, psychosocial support, and empowerment. 14 The reviews also identified interventions that showed promise with adults and would need to be further investigated for effectiveness with adolescents; these included decentralization of health care, task-shifting and community-based adherence support, nutritional support, and differentiated care that targets resources toward high-risk patients. 13,14 Overall, interventions that included community-based services provided the strongest evidence base for improved retention among adults. 13 The authors recommended further investigation on youth-friendly services—a widely promoted and utilized approach, but not supported by adequate evidence—and an extension of the focus beyond health facilities, to individual-, community-, or policy-level interventions. 13
While the systematic reviews cited above identify specific types of interventions that show promise for ART adherence and retention in care, they also highlight the very limited number and low quality of many studies on adolescent adherence and retention published up until 2015. There have been no published systematic reviews synthesizing evidence beyond 2015, notwithstanding the increase in focus on HIV-positive adolescents and the rapidly changing global policy, funding, and implementation environment in which HIV programming operates. An updated review, covering all types of interventions, would be useful to identify recent studies that may potentially reinforce the previous limited evidence for specific types of promising interventions, as well as broaden the synthesized knowledge base to include new and innovative interventions for this population group.
This systematic review aimed to (i) identify and synthesize empirical evaluations of interventions designed to improve ART adherence or retention in care among adolescents (10–19 years) and youth (15–24 years) published since January 2016, and (ii) discuss implications of these findings, in relation to previous reviews and empirical evidence, for future programming and research with adolescents and youth. Taking into account the expected limited number of studies with adolescents only, we extended the population age range to include youth; however, given the specific interest in adolescents, findings will be presented separately by age group (adolescents 10–19 years; youth 15–24 years; adolescents and youth 10–24 years), where age-disaggregated data are available. Moreover, this review was not limited to interventions at health facilities, but instead aimed to incorporate a broader range of initiatives, including community- and individual-level interventions.
Methods
The literature review was conducted between May and November 2018; the review protocol was registered with PROSPERO (Registration No. CRD42018110343). The systematic search strategy, including examples of search strings used, is illustrated in Table 1. We searched 11 health and humanities databases, including PubMed, ProQuest Health & Medical Complete, SocINDEX, and the Cochrane Library (see Table 1 for full list).
Systematic Review Search Strategy
PICO, Participants, Interventions, Comparisons, and Outcomes.
Composite search strings were created using keywords to indicate the population of interest (adolescents and/or youth living with HIV and enrolled in an ART treatment program) and the outcomes of interest (HIV treatment adherence and retention in care), drawing from Cochrane Collaboration guidelines 20 and search strategies used by previous reviews. 14,15 In particular, guidelines from the Cochrane Handbook for Systematic Reviews of Interventions were used to refine our review objectives and develop inclusion and exclusion criteria for studies. 20 The acronym PICO (Participants, Interventions, Comparisons, and Outcomes) refers to the following components of the research question that need to be specified to inform eligibility criteria for inclusion in a review: the types of population (participants), types of interventions (and comparisons), and the types of outcomes that are of interest. 20 These in turn inform the search strategy and search terms.
We identified the PICO components for this review and, after crosschecking with search terms used in similar previous reviews for completeness, 14,15 developed composite search terms that included keywords for the population and outcomes of interest (Table 1). Also, in line with the Cochrane guidelines, we limited our primary outcomes of interest to a small number of outcomes identified as meaningful for this review (adherence to ART and retention in HIV care), and aimed to include studies with both adverse and beneficial outcomes. 20 However, given the potential wide range of interventions and low expected number of relevant studies, the search strategy did not include keywords for types of interventions; this was assessed manually. Also, no geographical or language limiters were used.
All references from the online databases were imported into Endnote, where duplicates were identified and removed. The authors independently examined titles and abstracts for inclusion. Full text of potentially relevant studies was retrieved and independently examined by the authors. Reference lists of articles deemed relevant were also hand searched to identify further potentially relevant studies. Summaries of each article were developed using a standardized form, similar to those used for previous reviews 13 –15 that extracted key information and characteristics of each study (Table 2).
Description of Intervention Types and Sample Age Groups
ART, antiretroviral therapy; CACs, community-based adherence clubs; CBS, community-based support; HAART, highly active antiretroviral therapy; SMS, Short Message Service; STI, sexually transmitted infection; YAFS, youth- and adolescent-friendly services.
Studies were considered eligible for inclusion in this review if they (i) evaluated the effects of or associations between an intervention and ART adherence or retention in care or related biomedical outcomes (e.g., viral suppression or CD4 count); (ii) reported quantitative measures of key outcomes; (iii) worked with or included samples of adolescents (10–19) and/or youth (15–24) living with HIV and enrolled in an HIV treatment and care program; and (iv) were published between January 1, 2016 and June 30, 2018. Given the limited research on this topic, we included randomized control trials (RCTs) as well as nonrandomized studies (e.g., cohort studies, case–control studies, retrospective studies using routinely collected facility or program data, pre–post assessments).
Studies were excluded if they were not conducted with the population age group of interest or did not disaggregate and report on data specifically for this age group (e.g., studies with children or adults, whether or not including youth/adolescents), if they did not test a specific intervention (e.g., correlational analyses), if they were not full peer-reviewed articles based on new empirical analyses (e.g., editorials, commentaries, reviews, abstracts), or if they focused only on pre-ART care or linkage to care.
The authors independently reviewed each included study for methodological quality; discrepancies in this assessment were resolved through discussion. This review applied the same quality assessment tools used by the systematic review of MacPherson et al., 15 in part to allow for greater consistency between quality assessments of earlier studies included in previous reviews and the (more recent) studies included in this review: these are the Cochrane Collaboration's Tool for assessing Risk of Bias for randomized controlled trials, 21 and a modified version of the Newcastle–Ottawa Scale for nonrandomized studies. 15,22 A judgment of “UNCLEAR” was made for individual risk of bias items within these tools, where the study report did not provide adequate information. Each study was allocated a final quality of evidence rating of “low,” “moderate,” or “good” quality, based on the assessment of overall risk of bias.
Results
Figure 1 shows the PRISMA diagram illustrating the selection process for inclusion of studies. The review generated 2425 citations from the online databases, 1068 after duplicates. Ten studies were identified as relevant and eligible for inclusion in the review. Characteristics of these studies are summarized in Tables 1 and 2.
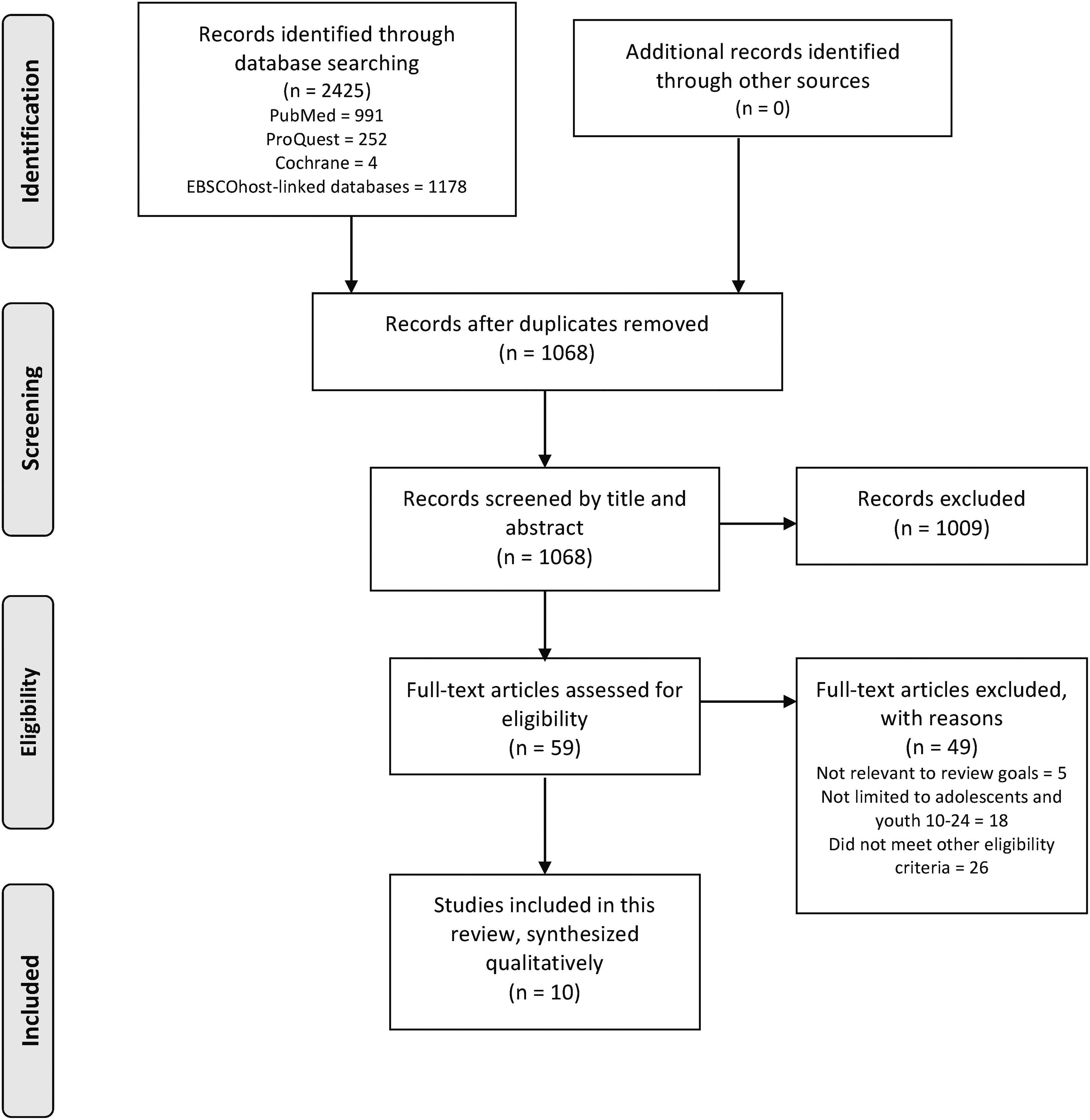
Selection process for inclusion of studies.
Characteristics of relevant studies
As illustrated in Table 1, three studies were conducted only with adolescents (between 10 and 19 years), 5,23,24 three studies with youth (between 15 and 24 years), 4,7,25 and four studies with adolescents and youth (between 10 and 24 years). 26 –29 The large majority of studies (8) were conducted in sub-Saharan Africa (South Africa, Kenya, Uganda, and Malawi); of the remaining two studies, one was conducted in the United States 28 and one in Haiti. 5 Two studies were identified as randomized controlled trials, 24,25 one as a nested case–control study, 23 and the remaining seven as retrospective cohort studies. 4,5,7,26 –29 Total sample sizes ranged from 6228 to 6706, 29 however, with the exception of the article by Ingerski et al., all studies worked with samples greater than 200.
As illustrated in Table 1, six studies were clinic based: five of these studies evaluated youth-friendly clinics or youth-friendly services 5,7,23,26,27 and the sixth reported a placebo pill trial. 28 One study tested an individual-level mHealth mobile phone message intervention, 25 whereas the remaining three assessed family- or community-based initiatives, respectively, comprising: an economic empowerment intervention; 24 a community home-based health care intervention; 29 and community HIV treatment adherence club support groups. 4
Key outcomes of interest and their measurement also differed across studies. One study measured treatment adherence through pill bottles with electronic monitoring systems, triangulated with self-reported adherence. 25 Four studies used some measure of retention in care or, conversely, LTFU, indicated by the patient's absence at the clinic or nonattendance of clinic visits over a given period of time, where possible, after checking for documented death or transfer. 5,7,23,26 Three studies used some combination of LTFU and biomedical outcomes (e.g., viral suppression measured through viral load; CD4 counts). 4,27,29 Lastly, two studies used only biomedical measures of CD4 count and/or viral load data as outcomes. 24,28
Given the small overall number of studies with these population groups, the range of different settings and populations, intervention types, outcomes, and outcome measurement approaches, we determined that meta-analysis of these studies' results would not be reliable. We have therefore provided a qualitative synthesis, whereby we discuss the types and modalities of interventions that have and have not shown success, and relate these to previous intervention evaluations among similar and broader population groups.
Findings of relevant studies
This section will describe findings of included studies in relation to their effectiveness for adherence and retention or related biomarkers. These will be described for each individual type of intervention, as per the categories indicated in Table 2, that is: youth-friendly clinics or services, the placebo pill trial intervention, the mHealth intervention, and household- or community-based interventions. Greater detail on the nature of each type of intervention and findings of each intervention study are provided in Tables 2 and 3.
Characteristics of Included Studies
CHC, community health center; CSA, Child Savings Account; LTFU, loss to follow-up; MEMS, medication event monitoring system; VL, viral load.
“Youth-friendly” clinics or services
As indicated above, the most frequent types of interventions tested were youth-friendly clinics or youth-friendly clinic services within existing facilities. There was considerable heterogeneity in the “basket” of services and characteristics included within the definition of “youth- or adolescent-friendly.” These included combinations of services, such as HIV- or other health-related education, psychosocial support and counseling, referrals, screening for sexually transmitted or opportunistic diseases, defaulter tracing and adherence support, recreational activities, and characteristics such as accessibility of clinic location and hours, the nature of the clinic environment, and the youth-specific knowledge or competency of clinic health workers. All of the five studies in this category focused on retention as an outcome, whereas one study also assessed differences in viral suppression. 27 These intervention evaluations showed mixed results, with two studies suggesting a positive impact on retention 23,27 and one of these also on viral suppression, 27 and the other three showing no significant effects on retention. 5,7,26
Placebo trial intervention
The last clinic-based intervention was a placebo pill trial, through which participants were prescribed pills with an inert substance mimicking the HAART regimen, to allow them to practice taking HAART and identify possible barriers to adherence. 28 This intervention did not show evidence of effectiveness, as biomarkers (viral load and CD4 count readings) for youth who received one or more trials were not significantly different from those who did not a year postintervention. 28
mHealth intervention
The one individual-level intervention evaluated, the mHealth study, did not find significant differences in adherence between youth receiving reminder SMS (Short Message Service; text) messages and those who were not, over a 48-week period. 25 This was the case for both the one-way and two-way messaging intervention groups.
Community- or household-based interventions
Instead two household-based interventions provided evidence of better outcomes among young people who received the intervention: Bermudez et al. found higher odds of viral suppression at both 12 and 24 months among adolescents who participated in their savings-led economic empowerment intervention, compared with controls. 24 Fatti et al. found the receipt of a home-based health and support intervention to be associated with lower LTFU (higher retention) and mortality rates 5 years after the intervention. 29 Lastly, the study evaluating community-based adherence clubs found significantly lower LTFU after 1 year for adults in the intervention group, but not for the population of interest for this review, that is, youth 16–24 living with HIV. 4
Study quality and risk of bias assessment
Most of the studies included in this review were judged to be of moderate quality (Tables 4 and 5); three studies achieved a “good” rating (one of which was an RCT) and one received a “low” rating. For the two RCTs it would not have been possible to prevent knowledge of allocation to the intervention recipients or implementers, given the nature of the interventions. 24,25 Quality concerns among the nonrandomized studies included lack of clear or adequate information on intervention and control group selection criteria, 4,5,28 the consistency of the intervention's application to all participants, 7,23,26 and how missing data were addressed in the analyses. 4,23,26,28
Methodological Quality and Risk of Bias Assessment for Randomized Controlled Trials
Methodological Quality and Risk of Bias Assessment for Nonrandomized Studies
Other concerns for specific studies were short follow-up time, 26 small sample size and not controlling for potential confounding factors, 28 insufficient detail on the nature of the intervention, 7 and changing composition of the intervention and control groups throughout the duration of the study. 5,23 Several studies also indicate high risk of selection bias inherent in the allocation of participants to the intervention versus control groups; 4,27 –29 examples of selection bias include exclusion from the intervention group based on the participant's health status, access to the intervention service, or a maximum cutoff number for the intervention.
Discussion
This review highlights several positive developments in studies focusing on adolescent and youth ART adherence and retention in care interventions post 2016. First, there appears to have been a shift in geographical focus since the publication of previous reviews, 14,15 from HICs to lower-income countries most affected by generalized HIV epidemics; 9 of the 10 studies identified in this review were in fact conducted in LMICs, and 8 in sub-Saharan Africa.
Second, while it is difficult to confidently make direct comparisons between study quality assessments of different reviews (due to different foci and an element of subjectivity inherent in assessments made by different groups of individuals), it appears there has been a quality improvement in RCTs conducted in recent years with adolescents and youth (noting that all RCTs in the review of studies by MacPherson et al. before 2014 were graded as low).
Third, there has been a clear increase in sample sizes and follow-up periods: intervention group sizes for most of the studies included in this review were over 200, whereas intervention group sizes for the large majority of studies in previous reviews ranged between 10 and 50 participants; 14,15 with the exception of one study, all studies identified in this review had follow-up periods of 12 months or more, whereas many studies included in previous reviews with youth had follow-up periods below 6 months. 14,15
Studies included in this review provide further evidence for previously tested approaches with youth and adolescents, and extend the evidence base to new approaches with this population group. Below, we discuss the implications of findings for each type of intervention study included in this review, in relation to the broader empirical literature.
Youth friendly clinics and services
This review shows an increase in the number of adolescent- or youth-friendly clinic intervention evaluations, as had been advocated by previous review articles. 13,15 These interventions likely draw from WHO recommendations that adolescent-friendly services be accessible, acceptable, equitable, appropriate, and effective, 30 by aiming to improve the physical space and social environment. 27,31 However, despite high hopes, studies evaluating youth-friendly approaches in this review show mixed results.
When considering this finding, it is of course important to take into account the heterogeneity in youth-friendly models across studies and the methodological limitations of studies, both described above. It is possible that certain components or services may be more strongly associated with better outcomes than others, and that this may differ in different contexts. In fact, a recent cross-sectional study, conducted across multiple (12) clinics in the United States, found retention in HIV care among youth to be associated with some youth-friendly components of care, such as clinic waiting areas intentionally designed for youth, evening hours, and providers with training in adolescent health, but not with others, such as clinic location or accessibility. 32 However, we were not able to identify clear commonalities in the models adopted among studies in this review that showed effectiveness, or differences between those that did and did not.
It is also worth noting that, while most of the facility-level studies included in this review were conducted at public clinics, they were either based at one clinic or groups of clinics participating in existing interventions or networks; it is therefore unclear whether these could be considered representative of youth accessing health services nationally or even in the study area.
Evidently, further research and consideration are required to better understand why youth friendly approaches may work in some cases and not in others. Well-designed and reported implementation science methodologies could be employed to identify which aspects or components of specific youth friendly interventions may be working or not working well, and why. 33,34 Moreover, implementation research could compare the effectiveness and cost-effectiveness of different youth-friendly clinic models. It could be particularly useful to disaggregate and assess specific characteristics of interventions, for example, individual intervention components, intervention timing and dose, implementers, target population, and outcomes. 33 This research could be informed by qualitative studies conducted with health providers and young people that explore perceived facilitators and barriers to care, to strengthen health service implementation and uptake. 34 –36
Placebo trial intervention
The placebo pill intervention did not show positive impact with adolescents and youth in the United States. 28 These types of trials applied to ART among young adults are in their early stage, and it should be noted that the quality of the study by Ingerski et al. was assessed as low in this review, in part because of the small sample size. Nevertheless, it is unclear whether there would be value in further investigating this type of intervention in LMICs most affected by the HIV epidemic, where coexisting social and economic factors may present greater obstacles to adherence 5 than knowledge and discipline linked to pill taking.
mHealth intervention
The only study in this review evaluating an mHealth intervention did not provide evidence of effectiveness. 25 Although this was the first known study to report effects of a mobile phone text message reminder intervention on ART adherence among adolescents and young adults, previous studies testing similar interventions with HIV-positive adults in Africa and India have shown mixed results. 37 –40
While enthusiasm for interventions that take advantage of increasingly accessible mobile technology is understandable, this clearly needs to be tempered with more reasonable expectations as to what text messages alone can achieve. 25 The content of the intervention reported in the study by Linnemayr et al. (standardized messages that asked whether the participant felt well or unwell) was very limited and may not have been sufficient to have significant impact. We also need to consider that text messages alone may not be particularly effective for adolescents in some of today's societies, given increasing volumes of messaging, and also lower cellphone network coverage in rural and remote areas within Africa.
Future mobile technology interventions should explore additional functionality, such as adherence feedback, or integration into broader m-Health approaches. 14,25 For example, a recent US study with 91 young men who have sex with men showed the preliminary success of an intervention utilizing multiple social media (including Facebook, texting, and GPS-based mobile social and sexual networking) in increasing retention in HIV care and viral load suppression. 41 Further testing of similar initiatives with larger samples among general adolescent and youth populations in LMICs would be very useful.
Household- or community-based interventions
Two studies in this review provide evidence of potential effectiveness of community interventions with adolescents and youth, including home-based health care and broader economic empowerment initiatives such as savings mechanisms and financial management education. 24,29 The study results from Fatti et al. extend findings of previous studies showing positive effects of community support interventions on retention among adults and children, 42,43 and a recent RCT showing improvements in viral suppression and mortality among children (6–15 years) whose caregivers received structured support from community health workers. 44
The study by Bermudez et al., instead, is the first known evaluation of an economic empowerment intervention aimed at improving HIV treatment adherence among adolescents (a previous pilot study showed promise but tested a combination of motivational interviewing and financial incentives and worked with a very small sample of 11 adolescents 45 ).
However, the importance of economic support is not surprising, as transportation costs and food insecurity have been identified as the greatest challenges to adolescent treatment and care in sub-Saharan Africa. 46 Recent cross-sectional analyses with over 1000 ART-initiated adolescents in South Africa's Eastern Cape province found SDG-related provisions—such as access to basic necessities, food security, government cash transfers, and household employment—to be associated with reduced mortality risk [indicated by lack of viral suppression and/or symptomatic untreated tuberculosis (TB)]; moreover results showed a strongly graded reduction in risk in the presence of multiple provisions. 47 In addition, there is prior evidence pointing to the usefulness of economic strengthening initiatives with HIV-positive adults in LMICs; for example, an agricultural and microfinance intervention in Kenya was found to improve viral suppression, CD4 counts, and food security. 48
The promising findings of family-based and economic empowerment initiatives reinforce the need to move beyond the health facility or possibly even health sector, to further investigate broader and multi-faceted interventions that address social and economic barriers to treatment adherence. While it is important to better align clinic facilities to the needs of adolescents and youth, a number of studies now indicate that this may have limited impact on long-term retention post-ART initiation without also addressing socioeconomic, family, and community factors. 5 Suggested potential foci include developing and testing interventions that encourage family disclosure and support, strengthen adolescents' social networks, reduce stigma, and provide community-based services, including transport. 5,16
Nonetheless, positive findings of community- and family-based initiatives should be considered with caution, since the evidence base with youth and adolescents is still small: this review only identified one study for these types of interventions and each was the first of its kind to be tested within this population group. Further evaluations are clearly needed both to determine the effectiveness of these interventions and the various mechanisms through which this may occur. For example, a home-based intervention offering multiple services could positively impact HIV treatment retention through one or more factors, including referrals and clinic linkages, better health care, better mental health, and self-management skills. 29,49
From a research and programmatic perspective, it would be important to be able to disaggregate and separately test individual components of multi-component interventions, to determine which aspects of these programs are (more or less) effective. This was reported as a challenge by previous authors when reviewing interventions. 14
Lastly, the study evaluating community-based adherence clubs found a reduction in LTFU for adults (in line with previous studies with HIV-positive adults 42 ) but not for youth 16–24. 4 This finding highlights the fact that interventions with positive impact for adult populations may not always work for adolescents and youth, a group with particular difficulties and needs. It reinforces the need to develop interventions and conduct rigorous evaluation studies specifically with adolescents and youth in mind, preferably soliciting their feedback on intervention design and barriers to retention 23 through qualitative or mixed methods research. 36
Concluding thoughts
Despite a notable increase in the relative number and quality of studies published over the past two and a half years, the current pace of intervention research with young people living with HIV remains highly disproportionate to their needs. 17 The overall number of studies for each type of intervention is still small, quality across studies is inconsistent, and—even for interventions with more available evidence—findings are inconclusive. In particular, this and previous reviews highlight the very small number of studies conducted specifically with the 10–19 (adolescent) age group, despite this being the potentially most vulnerable age group in need of effective support and adherence interventions. 2,3
We clearly need more, more representative and higher quality studies focused on youth and, more specifically, adolescents 10–19, or that disaggregate findings for these particular age groups. Moreover, there may be good reason to disaggregate even further based on subgroups identified by previous studies as potentially high risk for LTFU and poor biomedical outcomes, for example, older (15- to 19-year-old) adolescents 23 and adolescents transitioning from pediatric to adult care. 16 These particular groups of young people can fall through the cracks of existing systems and may require specific programming and transition protocols. 16
A greater focus on specific groups of youth speaks in part to the concept of “differentiated care,” which has gained traction in the recent HIV treatment adherence debate. 50 Certainly, focusing a greater proportion of health worker time and other health resources on more at-risk patients can potentially lead to higher retention among these critical groups, as well as efficiency gains and lower health worker needs. 13,50 However, possible long-term effects on adherence across various groups, as well as gains at facility level, are issues that require further investigation.
Lastly, while beyond the scope of this review, it is important to consider the replicability and potential sustainability of interventions, as well as their effectiveness. Many of the studies included in the 2015 review of MacPherson et al. comprised resource-intensive approaches such as individual counseling, education, and therapy. As argued by the review authors, these interventions may not be generalizable or sufficient to overcome the structural and systemic obstacles facing adolescents. 15 This may be all the more the case in LMICs in sub-Saharan Africa with generalized epidemics. The recent increase in studies conducted in LMICs in Africa is encouraging. However, it is important to consider whether these initiatives could be feasibly scaled up in the absence of large amounts of external donor funding or technical support and implemented within the (health worker and other) constraints of existing national health and social systems. 49
In this respect, operations research and cost-effectiveness analyses would be particularly useful to prioritize resources and monitor impact within the health system, 23,51 and determine the cost and feasibility of scaling up interventions beyond the health system (e.g., community-based interventions). Only one study included in this review, 29 conducted in South Africa, assessed costs and benefits (expressed as patient-loss averted) of the community-based support intervention tested, and found it to be cost effective. As argued by previous authors, 15 the public health benefits of expanding ART access to adolescents through universal treatment can only materialize when cost-effective and sustainable service delivery interventions are widely implemented.
UNAIDS treatment targets aim to eliminate new HIV infections by the year 2020; these targets include 90% of all people living with HIV knowing their HIV status, 90% of all people with diagnosed HIV infection receiving sustained ART, and 90% of all people receiving ART having suppressed viral loads. 12 While some progress has been made globally, we are still very far from achieving these goals among adolescents and youth, particularly in those parts of the world where most affected young people reside, such as sub-Saharan Africa. 2
This highlights the pressing need for interventions and service models among these specific population groups that are effective in increasing HIV testing and timely treatment uptake, as well as retention and treatment adherence to ensure viral suppression. To achieve these global public health goals, interventions and services will not only need to be effective, but also acceptable and accessible to young people, financially and operationally viable for scale-up, and sustainable in the medium to long term.
Footnotes
Acknowledgments
The study was supported by UNICEF Eastern and Southern Africa Office (UNICEF-ESARO), the Nuffield Foundation under [CPF/41513], the European Research Council (ERC) under the European Union's Seventh Framework Program [FP7/2007–2013/ERC Grant Agreement No. 313421], the ERC under the European Union's Horizon 2020 research and innovation program (Grant Agreement No. 737476), the Philip Leverhulme Trust [PLP-2014-095], and the University of Oxford's ESRC Impact Acceleration Account (IAA). Additional support is provided by Janssen Pharmaceutica N.V., part of the Janssen Pharmaceutical Companies of Johnson & Johnson, the Economic and Social Research Council [IAA-MT13-003]. John Fell Fund [161/033 and 103/757], and the International AIDS Society through the CIPHER grant (155-Hod and 2018/625-TOS). An additional award is being cofunded by the Medical Research Council (MRC) and the Department of Health Social Care (DHSC) through its National Institutes of Health Research (NIHR) [MR/R022372/1]. The funders have had no influence over the review design, search strategy, proposed analysis, interpretation, or publication of data.
Author Disclosure Statement
No competing financial interests exist.