
Abstract
Significant advances in our understanding and treatment of HIV have led to improvements in the medical management of the illness, as HIV infection has evolved from an acute to a chronic illness. Increasing our understanding of the medical and/or psychosocial comorbidities, which can interact to determine “clinical complexity” and impact HIV management, will further strengthen this process. Retention in care is a critical step of the HIV Treatment Cascade, which facilitates effective management of these comorbidities and their impact on HIV medical management. This study sought to build on literature regarding medical and/or psychosocial comorbidity that impacts retention in care, and it often leads to clinically complex presentations, by gaining the perspectives of people living with HIV (PLHIV), and medical and allied health clinicians in the field in Sydney, Australia. A total of 16 clinicians (medical doctors, nurses, clinical psychologists, and social workers) and 14 clients participated in a series of focus groups; they were asked to comment on the perceived barriers to retention and the potential solutions to overcome these. The results indicated a significant degree of overlap between clinician and client perspectives, and they identified “service-specific factors,” “logistic/practical factors,” “medical/physical factors,” and “psychosocial factors” as potential barriers to retention. Results are reviewed in the context of similarities and differences in perspectives between clinicians and PLHIV, and limitations regarding the generalizability of findings are discussed. The broader context of comorbidity and clinical complexity is also examined.
Introduction
Advances in the development, tolerability, and accessibility of antiretroviral therapy have significantly improved physical health outcomes for people living with HIV (PLHIV) and have increased lifespan. An aging population of PLHIV can be associated with increased comorbidities, which may interact to increase the burden of illness. 1 These medical and psychosocial comorbidities often contribute to complex clinical presentations, and they are increasingly the focus of clinical interventions within HIV services. 2
The HIV Treatment Cascade (Cascade) outlines the phases of HIV management and treatment from diagnosis through to viral suppression. 3 –5 Maintaining consistent viral suppression over the lifespan requires regular monitoring and effective management of relevant comorbid presentations that may impact illness progression; it requires that PLHIV remain retained in care. A recent systematic review suggested a number of factors that impact retention in developed countries, both medical/physical and psychosocial as well as system-specific factors. 6 What is clear in the retention literature, as well as research focusing on chronic disease and HIV more specifically, is that very rarely does one single factor impact health management. Rather, an often complex combination of factors, or comorbidity, influences individuals and, ultimately, health systems. The presence of comorbidity is often associated with poorer health outcomes, including poor quality of life (QoL) and morbidity. 7 In addition, complex presentations characterized by comorbidity impact service delivery and can stretch resources, as the identification of complex clients and integrated intervention solutions remain difficult to implement and require significant resources. In this way, deepening our understanding of the factors involved will assist in targeting personnel and financial allocations accordingly.
In translating research to clinical practice, an exploration of the perspectives of PLHIV and clinicians working in the field, in addition to existing literature, is imperative to ensure a well-rounded evaluation. Further, given the relevance of psychosocial as well as medical factors that impact HIV management, the views of allied health as well as medical practitioners in HIV are relevant and are consistent with a biopsychosocial model of health care. 8 The client perspective has also long been considered central to optimal service delivery. 9 Within many local health districts in Australia, community partnerships and direct client involvement in delivering effective and sustainable health care are considered essential. 10
To build on previous literature on this subject, this study sought to gain the perspectives of PLHIV and clinicians working in this field regarding the factors that might impact retention in care and effective management of HIV, viewed through the lens of comorbidity and complexity. Given the literature suggesting the complex interaction of comorbidities in PLHIV, this study seeks to explore the relationships between such factors.
Methods
Participants
Clinicians from The Albion Centre (Albion), the largest publicly funded interdisciplinary HIV clinical treatment center in Australia, were invited to participate. To avoid any direct pressure for staff to participate, a general email to medical doctors, clinical psychologists, social workers, and nurses was sent that detailed the study and invited interested parties to contact the research team. It was emphasized that participation was voluntary. Three clinician focus groups comprising 16 participants were conducted over a 3-week period during 2018, each comprising a mix of disciplines. Two medical doctors, six nurses, six clinical psychologists, and two social workers participated. Each group lasted between 45 and 60 min, and was audio taped with participants' consent for the purpose of transcription only.
Concurrently, four client focus groups were also conducted. Posters were displayed around Albion detailing the study and providing contact details for clients who wished to participate. Participation was voluntary, and the emphasis was on assisting Albion to monitor and improve service delivery, rather than to provide feedback to care providers. Confidentiality was stressed, and consent was obtained to audio tape the discussions for the purposes of transcription only. Fourteen clients agreed to participate in four groups. All participants (clinicians and clients) were provided with light refreshments during the process, and clients were additionally offered an AUD$20 groceries card in gratitude for their time and participation.
Focus group questions and data analysis
Two broad questions were asked of all participants, with additional clarification questions as needed. The two key questions were: What are the key factors that can get in the way of PLHIV attending their regular medical appointments, as recommended by their HIV specialist? Can you suggest any strategies that services could employ to improve these rates?
When indicated by the discussion, follow-up questions that were relevant to the specific role of complexity/comorbidity were asked. Examples include:
Do you think we are seeing an increasing number of comorbid presentations? [Clinicians]
Is there a particular profile of comorbid presentations that is more problematic for retention? [Clinicians]
Are there particular medical or psychosocial factors that might impact a person's ability to attend their appointments? [Clients]
Clients were reminded of the importance of confidentiality and were asked to draw on either their own past or current experience or the experience of others, but were asked not to disclose any identifying information if discussing others' experiences. One author (S.M.B.) facilitated each group, transcribed, and reviewed the results.
Analyses broadly followed the protocol for thematic analyses outlined by Braun and Clark. 11 The flexibility of this approach allowed for the data to determine the course of the thematic analysis, and it served as a basis to examine the similarities and differences between the areas discussed. Broad themes were identified, and NVivo v11 software assisted in the organization of these areas of interest.
Clinician and client focus groups were coded separately, with coding occurring on completion of all focus groups. A systematic coding procedure was developed, consistent with the protocol described by Braun and Clark 11 that involved the development of a clinician and client “codebook” by one author (S.M.B.), which was then discussed and reviewed by a second author (T.R.O.N.-J.). This codebook contained the broad themes identified, a definition, inclusion and exclusion criteria, and an example from the transcripts.
Two authors (S.M.B. and T.R.O.N.-J.) then independently coded the transcripts, according to the respective codebooks; the codes were discussed, with any discrepancies discussed until a consensus was reached. The codebooks were modified, as needed, as a result of these discussions.
Results
The focus group discussions targeted two broad areas: perceived barriers to retention and possible solutions to address these issues.
Clinician focus groups (n = 16) comprised 38% clinical psychologists, 38% nurses, 12% medical doctors, and 12% social workers. All were employed at Albion. A summary of client demographics (n = 14) can be found in Table 1. During focus group discussions, n = four clients were able to reflect on their previous personal experience of difficulty in attending appointments, and the reasons for this.
Summary of Demographic Characteristics of Client Participants
TAFE, Technical and Further Education.
Barriers to retention
The thematic analysis regarding barriers to retention identified four key categories: service-specific factors, logistic/practical factors, medical/physical factors, and psychosocial factors. These are outlined in Table 2.
Potential Barriers to Retention Identified by Clinicians and Clients Through the Thematic Analysis
Service-specific factors
Clients identified some service-specific barriers to retention, including previous (negative) experiences with a service and staff attitude.
“…and previous experiences, so if they've had experiences with clinicians not being favourable for them – they have very lasting effects in terms of whether a person will return to a service”
In addition, clients noted that the lack of flexibility of the service (e.g., ability to change appointment time), clinic processes, and staff attitude can serve as a barrier to retention.
“…providing enough options for the relevant Doctor who is overseeing the care to fit in – not necessarily ‘fit in’ but to find a working time that matches and respects that person's work schedule or life”
Clinicians also suggested that current support (e.g., IT) systems do not identify those who are accessing care elsewhere, and therefore a proportion who might be considered “lost to follow-up” might, in fact, be seeing another medical specialist.
“There are many different places that people can go, though, so I would say that if they can't come here they can go a few blocks that way, or a block that way, or a block that way…so what we might consider as “dropped out of care” might actually not be…”
Logistic/practical factors
Clients identified the location of services as a potential barrier to attending clinical appointments, especially for those who reside outside the inner city or in rural and remote locations. This was also considered important in the context of anonymity, and there was some overlap here with psychosocial factors such as stigma. Thus, clients living in rural or remote locations who lacked transportation to facilities where they felt anonymous appeared to be the most strongly impacted.
“… And the anonymity they, kind of – you know, if they go into the city they can likely come across a service and not stand out. Yeah, I think there are a lot of different layers when it comes to stigma and discrimination”
“…it depends on the access to services as well, and how close they are…”
There was a high degree of overlap between clients and clinicians, with both groups noting that requiring clients to attend appointments too frequently can serve as a barrier, as can having a service that does not offer holistic care. Some also noted that limited availability of appointments with a preferred medical specialist can also serve as a barrier.
“…and then I asked the doctor or he said to me “come back in 6 months time” – not the 3-month usual period, which is a far more nagging time.”
In addition, clients noted that employment restrictions (i.e., not being able to get time away from work to attend appointments) and weather (i.e., clients not wishing to travel in inclement weather conditions) can serve as barriers.
“For some people it might be the location and needing to travel to appointments. Or it could be the [bad] weather and people don't feel like coming out”
“Maybe some people…they might not take the steps to allow the time and logistics to work out and get to their appointments. They'll think ‘work is more important, I'll go to work’”
Medical/physical factors
Both clients and clinicians acknowledged the impact of an aging population of PLHIV on attendance to appointments, citing age, frailty, and mobility as potential barriers.
“Well I suppose as the population's getting older – so frailty is one of the things, and yeah, potentially getting transport to a service…”
In addition, both groups noted feeling well and feeling unwell/being asymptomatic as potential barriers; both options potentially limit clients from attending appointments, although for different reasons.
“It's like if you're experiencing symptoms, you're more likely to go to the doctor because it's bothering them, it's causing them pain. But if it's not, if it's not causing any distress – yeah, I can postpone that, I don't have to go to the doctor today. The more you start feeling something, then you want to get rid of that”
In addition, forgetting appointments, and changing priorities in the context of the changing nature of HIV (i.e., if HIV is well managed, not prioritizing attending appointments), were identified as potential barriers.
“Sometimes when treatment has stabilized and results are ok and you're getting the same results each time, therefore it doesn't become a priority – because it's managed. I might wait until there are other reasons to go to the doctor. I know that's not ideal, but it's the truth”
Clinicians also cited cognitive impairment as a potential reason that clients may not attend appointments, with some noting the potential for clinicians to misattribute the symptoms of cognitive impairment with personality traits or mental health symptoms.
“I see with my caseload now how many clients I follow up with quite regularly and 25–30 of them are living with HAND, and I feel like they're more impacted by HAND than people realise – the symptoms that they're showing in terms of confusion and things are put down to who they are, or their personalities, or their mental health diagnosis, but it's actually an impairment…and about how well we, how flexible we are in reaching out to make sure they're supported enough to come back each time because a lot of them just miss appointments because of confusion”
Psychosocial factors
Clinicians identified a number of social/welfare factors as potential barriers to retention (e.g., unstable housing or finances, and transient clients). A number of clinicians also suggested that “locus of control” might have an impact, noting that those clients with an external locus of control (i.e., believing they have little control over their life and attributing successes or failures to external factors) were more likely to fail to attend regular appointments.
“Well, your interpersonal personality disorders can affect a person's ability to negotiate and navigate any kind of relationship, including a professional one. And that touches a little on locus of control, and the way you see how empowered you are as well. A lot of people might feel very disempowered”
There was a significant overlap between client and clinician perspectives, with both groups citing stigma, substance use, mental health concerns, social isolation, and financial stress as potential barriers to retention.
“Thinking of some clients from particular backgrounds…whose families might not know they're gay, let alone HIV positive…You know, sometimes, they just go underground, and we have trouble getting in contact with them”
“You know, if you're recently diagnosed and you are on your own, and you don't have friends. That sense of isolation, and that can impact on your mental health, your depression, all that.”
“Sometimes it's because they're disempowered. Mental health is a big factor, those who are depressed…‘why bother’. Those who are anxious, it's very frightening so they might engage in other avoidance behaviours”
Beliefs and attributions were also important barriers, including burnout/exhaustion with the illness. This was particularly relevant for those who had been living with HIV for many years.
“…from a personal perspective, I guess – it can sometimes just get exhausting. It's like a constant reminder ‘I have this chronic condition that is being treated’ – I don't need constant reminders”
Clinicians also noted that beliefs in alternative medicine can serve as a barrier to accessing medical care.
“I think a lot of beliefs and adjustment issues. People who maybe don't want to go down the conventional medicine track – they might have other views about medicines and health and want to take alternative medicines, or maybe don't want to believe it or face issues yet”
Both clinicians and clients identified cultural/identity factors (including ethnicity, “belonging” to a particular cohort, and sexual/gender orientation) as potential barriers to retention in care.
“I think that it's also the fact that if they're culturally and linguistically diverse and from a migrant community. You can be from a culturally and linguistically diverse background but be Australian born and perfectly comfortable accessing services, but if you're a relatively new migrant, you know, there's more instances of social isolation, not being familiar with health services, and perhaps even a bit of mistrust”
“Culturally people have a different view of their health as well…not just because you value what you get in Australia that you wouldn't get in your country of origin. But you might not deal with those issues, especially when it's sexual, sex related”
Comorbidity and complexity
A strong theme that emerged from the discussions was that of comorbidity and how this contributes to often complex clinical presentations. Clients noted that there is often an interaction of multiple factors, rather than one variable in isolation, which can lead to feeling overwhelmed and this often impacts effective HIV management, including retention in care.
“…so it can be mental health issues, and it can be, like, a whole lot of other conditions they're dealing with and maybe sometimes I think social stuff is happening [too] and sometimes people can just become overwhelmed”
When asked whether clinicians believed that they were dealing with increased numbers of comorbid factors, they reflected on the changing nature of comorbidities in the context of HIV illness, rather than the number of presentations. They also specifically noted that comorbidity often results in complex clinical presentations that can be difficult for clinicians and services to effectively manage and support.
“The HIV population has changed. Once upon a time your comorbidities would have been high lipids and cholesterol and cardiac problems, and medication and disease progression – whereas now we can control that so people are getting older…so I don't know if it's more [comorbidities], I think it's different comorbidities…certainly in the way of HIV, if it's purely a medication adherence or a medical issue, it's a thing of the past. 80% of the population are a once a day regime which is long-lasting and robust, so if we look at this as purely being about medication – it's not an issue, it has to be everything else that goes with it”
“It's not just one thing, but the combination of factors which get in the way…complexity…”
Clinicians also noted the shift from focusing on biomedical aspects of HIV alone, to incorporating a recognition of other relevant factors, particularly the interaction of psychosocial factors such as mental illness, shame, isolation, and substance use.
“it's not purely medical but then flagging of anything else, mental health reasons, drug and alcohol reasons, additional comorbidities”
“I guess the biggest comorbidity that we see that interferes with engagement in care is crystal [methamphetamine], and that has increased dramatically in the time I've been here”
“…talking about that overlaying complexities, I think that the shame drives isolation, the isolation drives depression, and the isolation is that lack of connectedness, so it all kind of ties together”
Others also noted that comorbidity associated with aging was perhaps not as relevant to retention as we might expect.
“I don't know if the ageing comorbidities, I don't know if they do, unless it actually impacts on mobility, like physical impairment. I don't know, because I think the ones who are getting older and have ageing comorbidities were either engaged or not before…I don't know if we are losing that many through the ageing comorbidities”
Some clinicians also highlighted the need for individualized schedules of visits for clients, depending on the assessment of needs and the comorbid factors with which they present.
“The simple ones, once they're suppressed and they don't have too many other issues, then once every 6 months. But the ones that have comorbidities or other issues…then 4-monthly”
Potential solutions to improve retention
In addition to barriers to retention, the thematic analysis identified three key categories of potential solutions to improve retention: service-specific factors, logistic/practical factors, and psychosocial factors. These are also represented in Table 3.
Potential Solutions Identified by Clients and Clinicians to Improve Retention Rates
PBS, pharmaceutical benefit scheme; QoL, quality of life.
Service-specific factors
Clinicians identified a number of service-specific factors that could be enhanced to improve retention rates, such as care planning, improving the physical environment to meet the needs of all client groups, and improving interdisciplinary care, communication, and referrals.
“…[making sure we are] working with the client and working out what the schedule might look like and negotiating that with them. And I'm sure that we do that to a certain degree, but I'm not sure how far ahead we actually discuss those future appointments coming up, particularly if they're going to be someone complex. So sort of like a structured follow-up…asking them when it's best for them, when can they get in…”
Clients also identified supporting clinical services to improve cultural sensitivity and improving clinic processes and the ways in which staff communicate (e.g., booking appointments, and ensuring an empathic, vs. directive, mode of engagement).
“Not only in the language used, the cultural sensitivity, the rapport and deportment of the doctor…I mean – some Anglo [i.e. Caucasian] doctor in an Anglo way dealing with a non-Anglo person will not fit…because there's a very different loading, a very different cultural approach to health”
There was a degree of overlap between clinicians and clients within this category, with both groups highlighting the importance of excellent communication between disciplines, streamlined service delivery, and ensuring individualized schedules of visits (moving away from overly broad metrics of retention against which to compare attendance), “…for those complex clients…you do have a number of clinicians that are involved and are invested in ensuring the client is engaged in the service…a group of people that are responsible or working together to try and solve or resolve the issues to get people back in”
Both clinicians and clients identified a strong theme of having a client-centered approach to therapeutic relationships, which spans all aspects of contact with the service from initial contact with reception staff to clinical consultations. Clinicians also highlighted the importance of allowing sufficient time with clients. Clients, in particular, spoke about feeling comfortable within the service as they were not judged and felt respected. This points to a subtle difference between what services do, to how they deliver interventions.
“…they come here again and again, everyone is so nice to them, and don't make them feel any different”
“…you know, that you don't give up on them even in the darkest hours and when they can behave inappropriately…”
“…and even some of the patients who see me, and they're being managed by another doctor but that person doesn't have the time to explain what the test results mean…so they bring the results in and say ‘let's talk about this, and clarify this for me’…so we have that flexibility to listen to their problems”
Other potential solutions, identified by clinicians, included the importance of prevention/early intervention for difficulties (e.g., developing a screening tool), and improving IT/recall management systems to ensure alerts are in place for those who miss appointments or have not attended for a while.
“…and that's why I think a screening tool…to identify the right group, a flowchart of follow up, an alert system, and using the technologies to actually help us”
Clients also identified advances in and accessibility of medications, and trust in the medical system as factors that can improve retention.
“…It puts our trust in the medication as well, so you don't need to come back every 3 months just in case the medication doesn't work – so that trust in these biomedical interventions is crucial…”
Both clients and clinicians noted that the anonymity of a service could also serve to improve retention, particularly when there were concerns regarding stigma and/or discrimination. This appeared to be especially important for services that were known within the community to be designated HIV/Sexual Health services, compared with those nestled within a larger hospital or community health center where the reason for the visit would be largely unknown.
“…stigma of location…that a certain location has a reputation for why you go there…high visibility…for example, you could be going to [a local hospital in Sydney] for anything”
Logistic/practical factors
Clients and clinicians identified few logistic/practical factors that could improve retention, including improved assertive follow-up processes (e.g., extra reminders or phone calls when appointments are missed).
“Having an sms the day before and on the day – sometimes I get the sms the day before and I just forget it…but if I got a message on the morning, after I've had a chance to rest, I might remember better”
Psychosocial factors
Clients and clinicians identified a number of areas for growth in this domain. Both groups noted the role of community and peer-support workers to facilitate clients' capacity to navigate appointments within the service. Clinicians further identified the importance of structured case management, through the provision of planning, facilitation, and advocacy for clients, and some suggested that the clients may, in fact, be more engaged with a greater number of comorbidities.
“I don't know if there's evidence to support that, but it would be interesting to see, especially for the clients – the complex clients – it would be interesting to see if there are more points of connection to the service, if that would help them to be engaged more, than having just one point of connection”
Clients also noted the importance of shifting the focus from illness to improving QoL.
“…it's not necessarily that they want to hear that. What they want to hear is the new things, the new outcomes about information about HIV and quality of life and the things that they can do, you know…”
Discussion
This study sought to synthesize the perspectives of clinicians and PLHIV regarding potential barriers to retention in care in Sydney, Australia. These results sit within a broader framework that highlights that HIV retention is associated with many factors. However, the present findings bring new insights with respect to the specific role of comorbidity in impacting retention in care.
Both clinicians and clients identified many possible factors that can interact to impact retention rates. Largely similar messages from both clients and clinicians regarding a range of barriers to retention, as well as potential solutions to overcome these, were identified. The results of this study also complement existing literature on this topic, suggesting that comorbidity and the clinical complexity that often ensues should be an explicit focus of future research.
Service-related factors were identified by both clients and clinicians as potential barriers to retention, with both groups noting the importance of holistic care to address all needs of the client beyond medical alone. Other more practical factors that have been identified in the literature, such as appointment availability, 12 were also acknowledged.
The medical factors identified by clinicians and clients in this study account for the changing characteristics of an aging population of PLHIV, although it was unclear whether age-related comorbidities impact retention. The role of cognitive impairment was raised, with some suggesting that missed appointments may be explained by memory concerns related to cognitive decline. Interestingly, both groups also acknowledged that both ends of the “wellness” spectrum might be at risk of dropping out of care, which has also been identified in previous studies (e.g., McMahon et al. 13 ); because they are asymptomatic (and therefore do not prioritize their HIV care), or because they feel unwell and are therefore unable to attend appointments. This finding is consistent with the chronic disease literature. In a review of systematic reviews on the antecedents of poor adherence, Kardas et al. noted that an illness that lacks symptoms, or where clinical improvements are evident, can lead to decreased motivation to adhere to medication. 14 In the context of HIV, this might extend to appointment adherence.
Psychosocial factors were possibly the most important cluster identified in this study. Clinicians noted that an external locus of control could impact retention, whereas clients identified apathy as a possible barrier. Some authors have also suggested similar factors, such as feeling hopeless about treatment, 15 or “not bothering”. 16 Both groups noted stigma, mental health concerns, substance use, and isolation as significant barriers to retention, suggesting that these are important factors to address, and these are again consistent with the literature on this topic (e.g., McMahon et al., 13 Tobias et al., 16 Lourenço et al., 17 and Nosyk et al. 18 ). A recent systematic review and meta-analysis on this topic highlighted the important role of mental illness, most commonly depression, in retention and stressed the importance of effective support and interventions to maximize engagement. 19 Isolation, in particular, is gaining significant traction within the chronic illness literature, with an increasing awareness of its impact on physical health outcomes, 20 well-being, and QoL. 21 In this study, burnout and exhaustion from the illness, medication, and accessing regular care likely contribute to mental health concerns, including depression and isolation.
Potential solutions were identified by both groups, which could be useful for future service planning. Early detection of difficulties was highlighted by many participants to facilitate a proactive approach for providing appropriate support, rather than waiting for difficulties to arise. A screening tool was suggested as one possibility to identify risk factors. Likewise, increasing recognition of the impact of medical and/or psychosocial comorbidity formed the foundation for multiple suggestions of enhancing the interdisciplinary care model, streamlined service delivery, and assertive follow-up processes. Other, more practical, suggestions included improving appointment booking systems and IT support systems to facilitate alerts when clients did not attend for some time. A related issue is the sharing of attendance information between clinics, so it is possible to know whether a client is attending to their HIV needs elsewhere. Interestingly, the strides made in mobile technology to support retention were not raised here, although these are well documented elsewhere. 22
Client and clinician groups argued that no single (or group of) factor(s) was consistently considered to negatively impact retention; rather, the consensus seemed to be that often a combination of factors is present (comorbidity), and that these factors appear to interact to potentially worsen a person's capacity to effectively manage their HIV infection, including retention. The results of this study suggest that a combination of medical and psychosocial factors, as well as service-specific variables (including staff empathy/communication and logistics), all intersect to impact retention. Despite advances in the medical treatment of HIV, mortality rates remain higher than the general population, even in those whose treatment is considered “successful”, 23 highlighting the importance of recognizing the role of other factors at play. In resource-limited countries, commencing second- or third-line treatments is often associated with poor adherence and, therefore, also contributes to mortality. 24 Common comorbid presentations associated with HIV mortality, such as Hepatitis C, 25 smoking 26 in resource-rich countries, and tuberculosis in resource-limited countries, 27 were not identified in this study, but they remain important in the context of thorough examination of all relevant comorbid factors related to HIV management.
Comorbid combinations identified in this study included the interplay between psychosocial variables, with some noting that medical and aging factors are perhaps less pertinent for retention rates. This highlights increasing recognition of the impact of psychosocial comorbidity, such as mental illness, substance use, shame, and isolation, and the fact that HIV can no longer be considered from a biomedical perspective alone. The changing nature of HIV was also reflected upon, in the context of a shifting emphasis of comorbid presentations from the medical to the psychosocial. There is certainly a precedent for this in the chronic illness literature (e.g., chronic pain 28 ), which accounts for and incorporates the psychosocial with the medical antecedents. Indeed, the results from this study identified relatively few physical (compared with service or psychosocial) factors that were perceived to impact retention.
Clinical presentations characterized by such a combination of comorbidities have been widely discussed in the literature and can be considered as “clinical complexity”: the interaction of medical and/or psychosocial comorbidity that can compound to impact treatment, health-related outcomes, and overall QoL. 29 –31 Some authors 29 have found that increasing the number of diagnosed comorbid conditions actually increased the odds of optimal retention in care; as one clinician suggested in this study, comorbidity might, in fact, mean more points of connection to a service. Others, however, have suggested that comorbid conditions increase fatigue and reduce retention rates. 30 Another study 32 noted that more than 25% of clients considered complex by their primary physician presented with a combination of psychosocial and behavioral factors that were influencing the complexity rating more than the medical diagnoses.
Consequently, clinical complexity should not be considered from the biomedical perspective alone, 31 and should include the possible range of other psychosocial and behavioral determinants. A deeper understanding of these comorbidities that contribute to clinical complexity, and in turn to a person's capacity to effectively manage their health, including remaining retained in care, is necessary to adapt service delivery to accommodate and support their needs.
Organizations, therefore, need to account for the potential role of medical and/or psychosocial comorbidity that can mitigate how service-specific and logistic/practical factors, as well as clinical interventions, are received by clients, all of which may ultimately impact retention. A schematic representation of the possible relationships between these variables, and their interactions, identified in this study is depicted in Fig. 1 and accounts for the complex interplay of these factors. Future studies could seek to quantify this model.
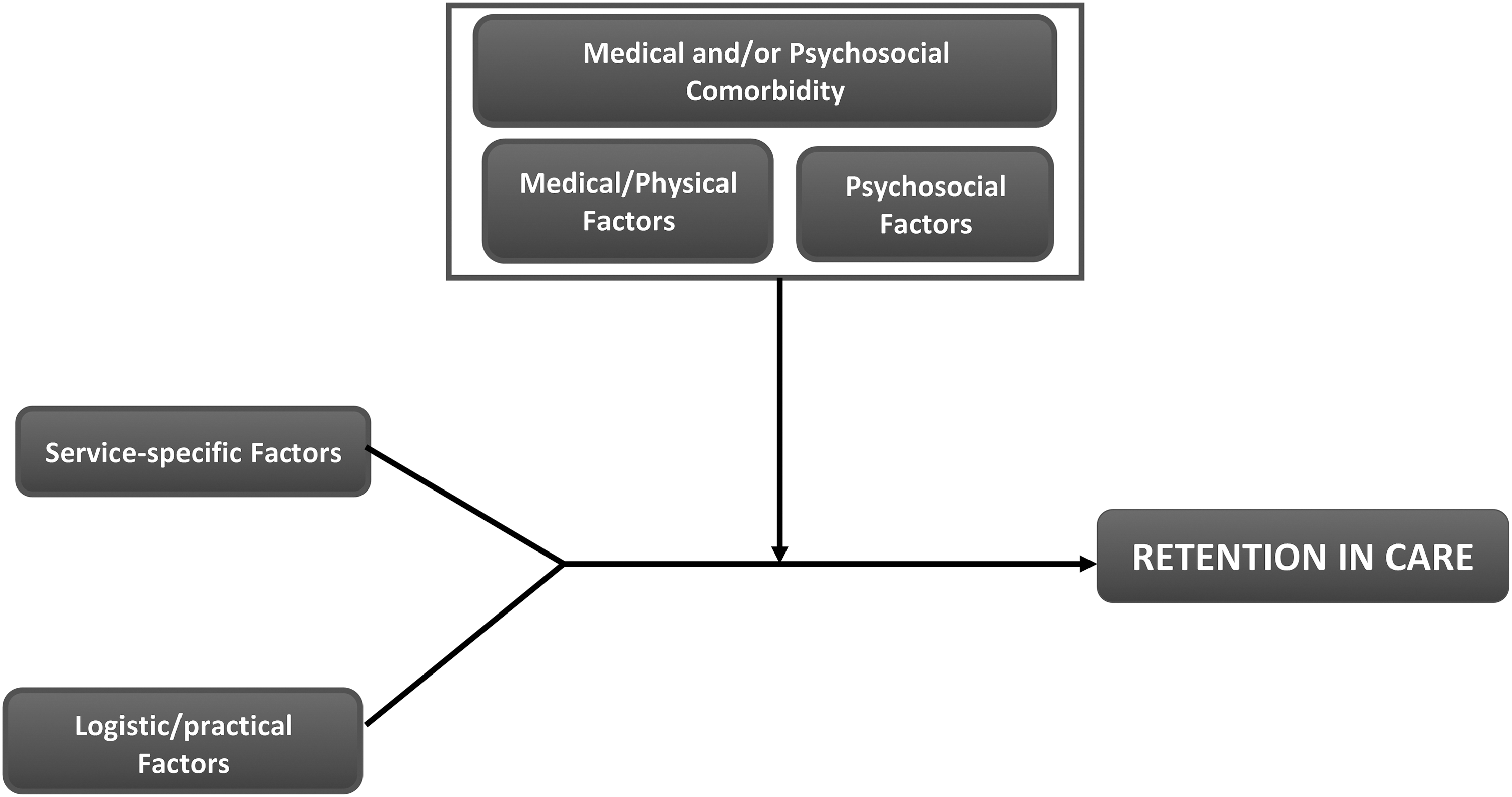
A schematic representation of the proposed relationship between the barriers to retention identified by clients and clinicians through the thematic analysis.
Limitations of this study include the fact that clinicians and clients were recruited from only one site. However, most of the clients involved in this study described experiences with several other services in the Sydney region. The present sample of PLHIV was relatively racially homogenous (predominantly Caucasian), and this, therefore, limits the generalizability of the findings. Research in this area has noted the disparity of retention rates between ethnic groups 33,34 ; therefore, future research should aim at accessing a more racially heterogeneous sample. This is particularly relevant in this study's findings with respect to the importance of cultural sensitivity in supporting retention, and how its absence can impede the same. Racial and ethnic disparities can impede retention by neglecting to recognize difficulties in language comprehension, and confusion in navigating a new health care system that can characterize interactions between culturally and linguistically diverse populations and service providers. 35 In planning service delivery, organizations should account for all populations represented in their client base to ensure retention, among other elements of the Cascade, and should ensure they are optimized.
A second limitation, inherent in research regarding retention in care, is the difficulty in sampling the target group of interest—those who do not attend appointments as they should. This study obtained the perspectives of clients who were generally well engaged and willing to participate, although they were able to draw on either previous experience of struggling to attend or the (anonymous) experience of others. The generalizability of the present findings are, therefore, limited. Focus groups in this study also contained fewer participants than the ideal, because focus group attendance was arranged according to participant flexibility and availability. Ideally, future research should aim at sampling clients whose pattern of retention is sub-optimal.
Future research in this field should also consider further exploration of the barriers identified both here and in the broader literature, and whether comorbidity patterns can be identified. Further, investigating the nature of the relationships between such variables is of paramount importance, to design and implement effective interventions.
Conclusions
This study complements existing research regarding comorbidity and retention in care, to provide the specific perspectives of PLHIV and the clinicians who support them. Early identification of and intervention for such medical and/or psychosocial comorbidity would be important to enhance the gains already made in the management of HIV as a chronic illness. Although the HIV sector in Australia is certainly moving in the direction of interdisciplinary medical and allied health coordinated care for PLHIV, there is more to be done to target our interventions to those most in need.
Footnotes
Acknowledgments
The authors would like to acknowledge the clinicians and clients who volunteered to participate in this research. Participants volunteered their time and were provided with light refreshments and/or a modest grocery voucher in gratitude for their participation, funded by the University of Technology Sydney.
Author Disclosure Statement
The lead author is a 2019 recipient of the NSW Health Education and Training Institute (HETI) Mental Health Research Award. The Albion Centre is an NSW health entity, and the WHO Collaborating Center for capacity building on HIV and STI care, treatment, and support.