
Abstract
The southern United States accounted for 52% of new HIV diagnoses in 2015. Visits to primary care providers (PCPs) offer opportunities for routine HIV screening. However, of at-risk persons in the United States who visited a health care provider within the previous year, >75% were not offered a test for HIV. Perceptions of patient population risk by PCPs could offer insight into these missed opportunities, and inform development of HIV testing interventions for PCPs to increase routine screening. During April–October 2017, we conducted online surveys regarding PCP's perceptions of patient HIV risk in six areas of the South with high-HIV prevalence. Surveys queried HIV-related knowledge, beliefs, attitudes, and practices. Free-text responses to the question “Are there any unique or special risk factors relating to HIV infection in your patient population?” were analyzed using NVivo for applied thematic analysis. Of 526 respondents, the mean age was 47 years with 65% white, 13% Asian/other, 13% black, 6% Hispanic/Latino; 71% female; 93% straight/heterosexual; and 35% offered HIV screening correctly based on standard of care. Main themes revealed were as follows: (1) provider perceptions of patient risk factors (e.g., “injection drug use is rampant”), (2) provider perceptions of patient barriers to access and care (e.g., “concern for parental notification and cost for treatment”), and (3) provider misconceptions of HIV risk and patient stigmatization (e.g., “I have a low-risk population”). Our findings suggest that PCPs in the South may warrant education regarding local HIV prevalence and routine HIV screening and prevention practices.
Introduction
In 2015, the South (Based on US Census definitions, the southern states include AL, AR, DE, DC, FL, GA, KY, LA, MD, MS, NC, OK, SC, TN, TX, VA, and WV) represented 38% of the US population, but had the highest burden of HIV incidence and prevalence in the country. 1 This region accounted for 51% of annual HIV infections, 46% of all persons living with HIV infection, and an estimated 51% of all undiagnosed HIV infections. 1
Moreover, racial/ethnic minorities, gay, bisexual, and other men who have sex with men (collectively referred to as MSM) and women are disproportionately diagnosed with HIV infection in this region. 1,2 Among persons living with HIV infection in the South, 32% were African American/black (hereafter referred to as black) MSM, 16% were Hispanic/Latino MSM, and 19% were black heterosexuals. 1 Among all women living with HIV in the South, black women accounted for 71% women living with diagnosed HIV infection. 1
Health professionals, particularly primary care providers (PCPs), are at the forefront to implement HIV prevention, treatment, and care services. However, recent data show that of at-risk persons in the United States who visited a health care provider within the previous year, >75% were not offered a test for HIV. 2 In another study, among persons who visited a PCP in the past 12 months, 58% reported not being offered an HIV test and 31% had never been tested for HIV. 3 Provider-initiated HIV testing is often limited due to factors such as HIV stigma, lack of provider knowledge of national HIV screening recommendations, and potential value judgments regarding HIV risk among one's patient population. 4 –6
Data regarding provider knowledge of HIV statistics and knowledge of behavioral, social, and structural factors that place patients at risk of HIV are limited. This information is essential to ensure that providers are well equipped to help as part of national HIV prevention efforts, which may include increasing the distribution of prevention resources [e.g., condoms, postexposure prophylaxis (PEP), and pre-exposure prophylaxis (PrEP)] and increasing access to HIV testing and to linkage to care among HIV-positive patients. Research regarding provider perceptions and activities could also offer insight into missed opportunities to curtail the HIV epidemic in the South. Therefore, we examined PCP perceptions of patient population risk for HIV infection to strengthen research strategies, and inform the development of provider-level HIV awareness and testing interventions.
Methods
Data collection
The K-BAP Provider Survey (Knowledge, Beliefs, Attitudes, and Practices of Providers in At-Risk Jurisdictions about HIV Risk, HIV Diagnosis, and Antiretroviral Drug Interventions) was a web-based survey to examine HIV knowledge and practices among PCPs in the southeastern United States. Study locations were determined using national HIV surveillance data available in 20157; the six metropolitan statistical areas (MSAs) in the southern United States with the highest HIV burden (based on prevalence in the national HIV surveillance report) were selected for study recruitment: Baton Rouge, LA MSA, New Orleans-Metairie, LA MSA, Baltimore-Columbia-Towson, MD MSA, Washington, DC MSA, Atlanta-Sandy Spring-Marietta, GA MSA, and Miami, FL MSA (these MSAs will be referred to throughout the rest of the article by their respective central cities: Baton Rouge, New Orleans, Baltimore, Washington DC, Atlanta, and Miami).
PCPs, including physicians, nurse practitioners, or physician assistants in primary care specialties (e.g., internal medicine, pediatrics, obstetrics, and gynecology), who practiced in these areas based on a national database listing, were invited to participate in the study through a mailed invitation. Following online consent to participate in the study, the PCPs were emailed a survey link and asked to complete the baseline survey through a web-based platform. Baseline data were collected during April 2017–August 2017. PCPs were mailed $20 cash as compensation for their time after completion of the survey (postsurvey payment). This study was approved by the Chesapeake Internal Review Board and the National Center for HIV, Viral Hepatitis, STD, and TB Prevention's project determination process.
Data analysis
Qualitative analysis
Free-text responses to the question “Are there any unique or special risk factors relating to HIV infection in your patient population?” were imported into NVivo 11 Pro and analyzed using applied thematic analysis. 8 Two qualitative analysts (K.D. and A.G.) first read all 526 responses and developed a preliminary codebook. After discussion, the codebook was finalized. Each of the analysts then independently coded the first 100 responses. Once the first round of coding was complete, the analysts compared codes through discussion until an intercoder reliability of 0.80 was reached. The first author (K.D.) then coded the remaining 426 responses. Main themes are summarized below.
Geographic information system analysis
HIV prevalence data, at the ZIP code scale, for five of the six MSAs in the study area were downloaded from the AIDS Vu site (
Results
Demographics
Of 4,595 with mailed surveys, 820 respondents were eligible, and 526 participants wrote in free-text responses used for this analysis. The 526 PCPs self-identified as white (65%), Asian/other (13%), black (13%), or Hispanic (6%). Mean age was 47 years, 71% were female, and 93% identified as straight/heterosexual. Over 42% of responses were obtained from PCPs in the Baltimore or Washington DC MSAs, 25% were from Baton Rouge or New Orleans, 22% from Atlanta, and 11% from Miami. Physicians were playing the most common clinical role (43%), followed by nurses (37%) and physician assistants (21%). The most commonly reported medical specialty was family medicine (23%), followed by internal medicine (21%). Infectious disease specialists were the least common (2%), and 19% reported practicing a medical specialty not listed (i.e., “Other”). Nearly 38% of PCPs reported practicing in a hospital-based environment, closely followed by private practice (33%). Thirty-five percent of PCPs offered HIV screening correctly based on standard of care (i.e., routine, opt-out testing). 9 Results are listed in Table 1.
Demographics of Primary Care Providers in Six Metropolitan Statistical Areas in the United States (n = 526)
Qualitative themes
Provider perceptions of patient risk factors
Providers addressed several examples of behavior and risk factors among their patient population that may have increased risk for HIV acquisition and transmission (n = 202). Examples included the following: risk of perinatal HIV transmission, late presentation for HIV, risk among vulnerable populations, alcohol and drug use, comorbidities, disclosure of risk behaviors to PCPs and HIV status to partners, and general sexual risk behaviors.
Perinatal transmission of HIV from mother to child during pregnancy and breastfeeding was a common concern among providers. One PCP mentioned that she worked in pediatrics, so, “the majority of our HIV patients were infected by their mothers” (Family Medicine, 40, black, female, Atlanta). Another provider revealed that young women in her practice are sometimes diagnosed with HIV while pregnant: “In Maryland, women represent 35–36% of all HIV-infected individuals. This is especially true in our pregnancy component among adolescent or young women who are often diagnosed in pregnancy” (Other specialty, 52, black, female, DC & Baltimore). However, another provider said that despite being exposed to HIV, most of the babies in her practice do not acquire HIV: “…most of our HIV exposed babies end up negative because of prophylaxis” (Other specialty, 29, white, female, DC & Baltimore).
Some providers mentioned that patients would present to their office/clinic with late-stage HIV or AIDS when newly diagnosed as HIV positive: “Advanced stage AIDS is most common in my practice,” an Atlanta-based provider stated, “My priorities are limiting exposure of HIV to partners and compliance with ART (antiretroviral therapy)” (Other specialty, 56, white, male, Atlanta).
PCPs felt that vulnerable populations such as individuals with disabilities, those with a history of incarceration, and people who were homeless were at risk of HIV. Two PCPs said that they worked with patient populations with disabilities (i.e., developmental disabilities), and that their patients were “at high risk to be abused sexually (and exposed to HIV), because they cannot defend themselves” (Pediatrics, 57, white, female, DC & Baltimore). Another provider indicated that he/she treated “many formerly incarcerated patients and many underserved patients” (Other specialty, 44, white, gender missing, Miami). Another concern for PCPs was “homeless shelter exposure” (Other specialty, 32, white, female, Atlanta), noting that urban locations can “contain a lot of homeless and disadvantaged patients” (Other, 63, white, male, Atlanta).
Alcohol and drug use among patients was a concern of several providers, with one stating that “Drug use is a big thing around here” (Family medicine, 48, black, female, Atlanta), and that “IV drug use (heroin use) is significant in our area” (Family medicine, 39, white, female, DC & Baltimore). Another PCP argued that among her patient population, drug use was the most common mode of HIV transmission: “Unique, no. Drugs are the main cause of HIV, sex with people who are IVDU a second major cause, other sexual causes seem to be less of a risk for the pts. Still, an issue, just less of one” (Family medicine, 71, white, female, DC & Baltimore).
Disclosure of risk behaviors and HIV status to PCPs was an additional concern. Providers stated that youth sometimes had a difficult time disclosing MSM status and sexual activity to health care providers, and that patients were apprehensive in discussing HIV status with them, as one PCP stated, “Patients here do not openly admit they have HIV until we ask about medication history” (Family medicine, 32, Hispanic, female, Miami). Others perceived that HIV transmission may be affected by lack of HIV status disclosure to sex partners: “Yes, persons who are already infected with the virus, constantly have unprotected sexual intercourse without informing their partners” (Family medicine, age unknown, black, female, DC & Baltimore).
Providers also mentioned sexual risk behaviors such as condomless sex, multiple sexual partners, and infidelity as factors potentially affecting HIV transmission in their patient population. “Multiple sexual partners,” one PCP stated, “I really need to do a better job about asking more definitively how many partners in the past 12mos” (Family medicine, 29, white, female, Atlanta). A few PCPs mentioned sexual abuse among immigrants [i.e., “high refugee population from Central America—many victims of trafficking or sexual abuse” (Pediatrics, 32, white, female, DC & Baltimore)], as well as in the military [i.e., “military sexual trauma history” (Other, 44, Asian/other, female, DC & Baltimore)]. Another provider stated that sexual networks played a role in HIV transmission in his patient population in Atlanta, and offered direction for future interventions:
Extensive, active sexual networks in this county, especially among young black males, probably with large social media components with alarming and accelerating rates of new HIV with severe presentations of acute HIV seroconversion, more rapid progression to AIDS. Massive public health education and interventions needed in the community and has to actually get to the people involved and be raw and honest and impactful. (Infectious diseases, 45, white, male, Atlanta)
Provider perceptions of patient barriers to access and care
Lack of resources
Forty-three providers gave examples of how patient resources were lacking, ultimately hampering PCPs' ability to provide HIV care and treatment. Health insurance coverage and access to transportation were common concerns. One provider stated, “There is a disproportionally high prevalence of HIV in the uninsured and Medicaid populations. Cost of ongoing healthcare and cost of medicines is a constant battle for them, sometimes even transportation to clinic is something they can't afford” (Emergency medicine, 35, white, male, New Orleans & Baton Rouge).
Insurance also impacted treatment for HIV, as one provider mentioned, “We have a high population of uninsured patients that come to us for STD testing. We are often the first ones to diagnose their HIV. When they don't have insurance, it's hard to find a place to send them for further management/treatment” (Other specialty, 28, white, female, Atlanta). Access to appropriate specialists and transportation to care was also a concern among PCPs: “There is a real lack of appropriate HIV care in my county with very few providers. People are traveling long distances for appropriate care” (Internal medicine, 63, white, male, Miami). Another PCP similarly noted that there was “poor public health and transportation infrastructure in GA” (Infectious diseases, 36, Asian/other, female, Atlanta).
Poverty and low socioeconomic status (SES) served as an additional perceived barrier to care according to providers, as did lack of education. One provider explained that illiteracy was an issue in her community, stating, “Many patients do not read/write” (Infectious diseases, 62, white, female, Atlanta). Lack of materials in languages other than English was an additional barrier to care, as a provider mentioned, “A lot of my patients are Hispanic and do not know the risks and health effects of contracting HIV. If I had some education materials in Spanish in my office, that would help with increasing public awareness because it is often something that is not talked about” (Family medicine, 30, white, female, Atlanta).
Psychosocial challenges
Twenty-one PCPs stated that providing care was complicated by communication challenges with patients, patient compliance and adherence with ART, mental illness, and HIV testing behaviors. Reaching and communicating with patients was more difficult in certain patient populations such as college students and adolescents, undocumented immigrants, those with low SES, those with a history of drug use, and homeless populations. PCPs expressed that providing continuous care was sometimes made more difficult by care setting (i.e., in a clinic setting), preventing PCPs from establishing relationships with patients: “All of our patients are attending college and are here for a limited time,” a provider stated, “No long term care for most of our patients” (Other specialty, 63, white, female, DC & Baltimore). One PCP expressed the difficulties of following up and treating patients with HIV who were homeless, and how mental health and substance use can affect adherence with ART:
I work with homeless individuals so identifying and treating these patients can be difficult and frustrating. These patients are often lost to follow up, non-adherent to medication and experience frequent interruptions in treatment due to lack of insurance, lack of transportation, lost or stolen medication, lack of access to care, and poor health literacy. Mental illness and drug addiction also impact adherence to follow up and ART. (Family medicine, 37, white, female, DC & Baltimore)
Complicating mental health illnesses such as depression, PTSD, and psychiatric disorders made care and treatment more difficult, particularly when coupled with substance use, as illustrated by one provider, “Substance abuse and psychiatric disorders limit compliance with therapy” (Emergency medicine, 42, white, male, Atlanta). Testing behaviors further complicated getting patients into care. Difficult to reach populations such as undocumented individuals, individuals who would be considered “baby boomers,” pregnant women who opt-out of HIV testing, and minors were some examples of populations which PCPs saw as difficult to get tested for HIV.
Fear and stigma
Thirteen providers reported that delivering HIV care and treatment was hindered by confidentiality concerns among patients and cultural stigma of HIV within their communities. Confidentiality concerns among youth and young adults in particular were significant for patients, according to PCPs. Fear of parents discovering sexual activity status, sexual identity, tests performed, test results, and treatment were all barriers among youth. One provider revealed,
I find it hard to convince parents/patients to consent to a blood draw if they are denying sexual activity. It's an easier sell for urine screening for gc (gonorrhea) and chlamydia. In general, pediatric patients are fearful of shots and needles. I would like to make it standard for say at 16 and over to have to get this done. Maybe I just need to change the expectation and maybe combine it with a cholesterol screening at the 16 year visit. (Pediatrics, 46, black, female, New Orleans & Baton Rouge)
Here, the provider shows two different barriers involving fear: fear of parental notification of sexual activity and fear of needles for testing. She also offers a solution to lower barriers to testing by making it routine. Other PCPs expressed similar views about confidentiality as a barrier to testing for youth, as another provider expressed, “Underage population whose parents have access to their billing and medical records and will be able to see what tests were performed. This may hinder them getting tested” (Pediatrics, 36, Asian/other, female, DC & Baltimore). Providers also indicated that confidentiality was a concern among college-age patients as well: “College student population, so there is a concern for parental notification or treatment and cost for treatment” (Family medicine, 37, white, female, DC & Baltimore).
Cultural stigma further complicated treatment and prevention options. One PCP described how prescribing PrEP can be difficult when a patient is covered by a parent's insurance policy. Prescribing PrEP to these patients may mean that they would have to discuss their sexual orientation with their parents, which can further be complicated by cultural norms:
Several of our patients are from Muslim countries which makes it very difficult to get them treatment without their parents finding out. Many of our patients are on their parent's insurance and they would have to come out to their parents in order to get the Truvada through their prescription drug plan. (Unknown specialty, 57, white, female, DC & Baltimore)
Providers discussed community stigma among certain racial groups and locations: “Many in the African-American community do not wish to speak about it” (Emergency medicine, 37, white, male, New Orleans & Baton Rouge), as one provider stated. Attitudes within communities in certain locations (i.e., the southern United States) also played a role in HIV prevention: “Louisiana is generally a conservative community with reluctance to openly discuss about sexually transmitted diseases” (Internal medicine, 55, Asian/other, male, New Orleans & Baton Rouge).
Low-risk perception
Nine providers commented that patients sometimes had incorrect perceptions of their risk of acquiring HIV. PCPs stated that patients with low-risk perception were youth, heterosexuals, whites, and blacks. Providers mentioned youth as having a “sense of denial” regarding HIV risk, believing that they would not acquire HIV: “I see youth, who often feel invincible and otherwise are naive, uninformed, and victimized by others” (Pediatrics, 60, white, male, Miami), as one provider stated.
Providers also believed that some patients had a “misconception [that HIV] cannot be contracted from heterosexual relationships” (Internal medicine, 43, black, female, DC & Baltimore), and that heterosexuals can sometimes “feel that they are not at risk for contracting HIV” (Family medicine, 44, white, female, Atlanta). Another PCP stated that some middle-to-upper-class white patients did not feel that they were at risk of HIV. Low-risk perception among young black gay men was a concern for one provider: “Our young African American male gay population seems very unconcerned about HIV and have multiple partners. Transmission rates among this sub group is very high” (Other specialty, 46, white, female, DC & Baltimore).
Provider misconceptions of HIV risk and patient stigmatization
While the majority of providers displayed accurate HIV-related perceptions within their patient population regarding HIV prevalence, incidence, and populations at risk, some providers held misconceptions and used stigmatizing language regarding patients (n = 14). Despite practicing in areas where HIV prevalence was high, a number of providers failed to acknowledge that their patient population was at risk of HIV. Providers stated that “we care for a very low risk population in general” (Specialty missing, 67, white, female, DC & Baltimore), “I have a low risk population” (Pediatrics, 50, white, female, Atlanta), and “I don't deal with this population” (Pediatrics, 36, white, female, DC & Baltimore). Another provider acknowledged that HIV prevalence in her area of practice was high, but stated that the risk of HIV among her patients was low: “I live in a high prevalence city for HIV but care for the higher income and lower risk patients within this community” (Internal medicine, 43, white, female, New Orleans & Baton Rouge).
Other examples of misconceptions were that elderly patients were not at risk (i.e., “No, my patient population is older adults in senior nursing facilities and nursing homes” (Family medicine, 32, Hispanic, female, Miami)), and that HIV was “not very prevalent in [their] suburban community” (Family medicine, 55, Asian/other, male, DC & Baltimore). A couple of responses carried a stigmatizing tone regarding patient sexual behavior, stating that patients had “promiscuous behavior” (Family medicine, 47, white, male, New Orleans & Baton Rouge), and that patient populations were “large uneducated population engaging in promiscuous sexual practices and large IV drug population” (Internal medicine, 40, Asian/other, male, New Orleans & Baton Rouge).
Geographic information system results/analysis
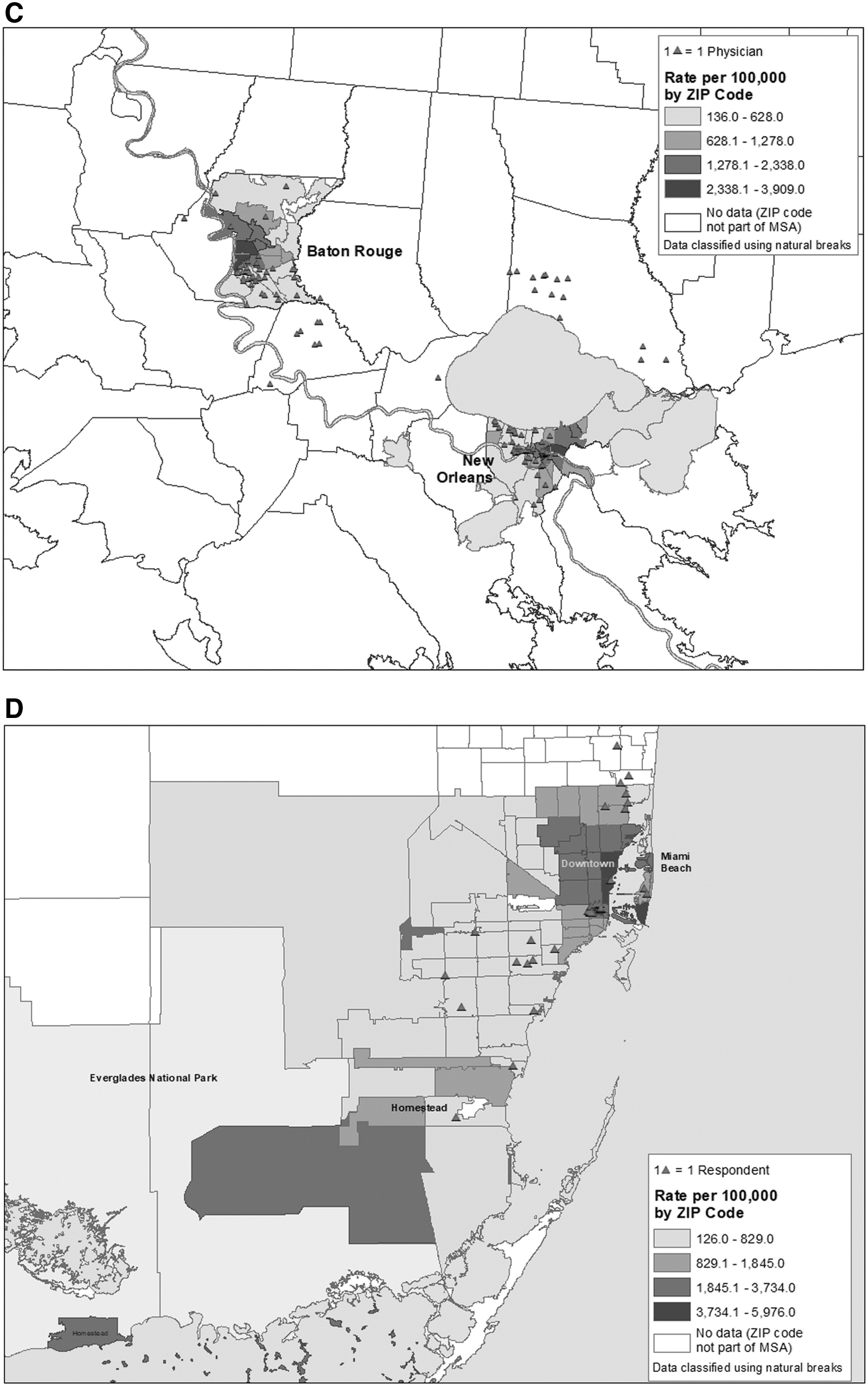
The geocoded locations of PCP respondents were overlaid onto HIV prevalence data, both at the ZIP code level (for all MSAs except Baltimore) (Fig. 1A–D); 505 of the 526 PCP respondents (96%) were able to be accurately geocoded. We examined the general distribution of PCPs relative to HIV prevalence. The maps used here are choropleth maps, where darker shades indicate higher disease prevalence; each triangle indicates the location of one PCP respondent, and they are plotted randomly within each ZIP code.

In the Atlanta MSA, the highest rates of HIV prevalence are in the central area of the city of Atlanta, and there is a concentration of providers, however, in the areas of downtown and southwest Atlanta there are fewer PCP respondents located. In addition, several of these higher prevalence ZIP codes are not served by the MARTA rail system.
In the Baton Rouge MSA, the PCPs are concentrated in the ZIP codes with lower HIV prevalence; in the New Orleans MSA, the ZIP codes around the French Quarter have the highest rates of HIV prevalence, and there is also a concentration of PCPs in this area. However, the eastern portion of the city of New Orleans had no PCP respondents.
In the Washington, DC MSA, the eastern areas of the city have higher HIV prevalence rates, especially wards 5, 6, 7, and 8. These wards have a low number of PCP respondents. Only county-level data were available for the Baltimore MSA, thus very few conclusions about HIV prevalence and provider location can be drawn.
In the Miami MSA, the highest HIV prevalence rates are in ZIP codes in Homestead, downtown Miami (e.g., the neighborhoods of Biscayne, Bay Shore, and Buena Vista), and Miami Beach. Several of these ZIP codes have few PCP respondents; the Homestead ZIP codes (a large geographic area) only have two PCP respondents and there are only two respondents on Miami Beach.
Discussion
We explored perceptions of patients' HIV risk by PCPs in the southern United States. Qualitative analyses revealed three main themes: (1) provider perceptions of patient risk factors, (2) provider perceptions of patient barriers to access and care, and (3) provider misconceptions of HIV risk and patient stigmatization. Coupled with geographic information system (GIS) data on provider practice location and HIV prevalence, these perceptions by PCPs shed light on the HIV epidemic in the South and the factors that may be influencing it from a health care perspective.
Providers described several perceived patient behaviors and risk factors for HIV, including perinatal mother-to-child transmission of HIV infection. Although perinatal HIV infections in the United States decreased by 32% from 2011 to 2015, 65% of perinatal HIV diagnoses in the United States in 2016 were among black/African Americans; social challenges with access to prevention and care services have been described as barriers for women during and after pregnancy. 7,10 In addition, perinatal HIV exposure surveillance and reporting has been difficult due mostly to budget cuts; strengthening resources in this area requires strengthening accurate PHES and reporting processes, especially in areas most affected by perinatal HIV transmission. 10,11 The high number of responses related to mother-to-child transmission may also be due to the fact that 44.9% of K-BAP PCPs who responded specialized in either pediatrics, OB/GYN, or family practice (44.9%).
Late presentation in seeking medical care was also described by PCPs; some patients had advanced HIV/AIDS or were diagnosed with HIV for the first time upon presenting for medical care. Late diagnosis with HIV is associated with higher mortality; social and structural barriers play a role in late diagnoses and presentation for care. 12,13 In US areas where late HIV diagnoses have decreased, sustained HIV testing efforts by providers have been noted as a major factor in increased numbers tested for HIV, especially in areas where HIV testing is federally funded. 14,15
Members of vulnerable populations such as those who had been incarcerated or homeless were also a concern for PCPs. Members of vulnerable populations are more likely than others to have housing instability, which can have negative effects on HIV care and viral suppression. 16 Many providers also mentioned substance use, especially injection drug use with opioids. Opioid use in the United States is particularly concerning, as the rate of opioid-related deaths has increased by 200% since 2000, 17 and people who inject drugs represented 6% of all HIV diagnoses in the United States in 2016. 7
Disclosure of risk behaviors to providers and to sex partners was also a theme brought up by providers. It is important for providers to know about patient risk behaviors for HIV, so that they may offer appropriate care, but some patients may not disclose certain risk behaviors due to stigma concerns or failure by providers to probe patients. 18 Furthermore, studies have shown that concepts of HIV risk differ among health care providers and patients. 19 Ensuring that provider settings are safe and nonjudgmental may increase patient comfort with disclosure of same-sex sexual behaviors or sexual identity with providers; PCPs may warrant additional training to ensure that settings are perceived as nonjudgmental by patients as this correlates with increased uptake of HIV testing. 20
Testing for HIV is important as part of the HIV care continuum, as ∼40% of new HIV infections are transmitted by persons unaware of their HIV-positive status; 21 people who know their status can seek treatment and decrease ongoing, unintended transmission. In addition, perceived discrimination by providers can negatively affect health outcomes for HIV-positive persons, such as lower adherence to ART. 22
Many PCPs also discussed lack of resources, challenges with access to health insurance, psychosocial challenges, stigma, fear, and confidentiality concerns as some common barriers to retention in care for HIV-positive patients. Retention in care is associated with lower HIV viral load and improved outcomes for HIV-positive patients, 23 yet some data suggest that retention in care lags for HIV-positive patients in the southern United States. 24 Our GIS data reveal limited access to care for many patients located within Atlanta, Baton Rouge, New Orleans, Washington DC, and Miami MSAs (we are unable to draw concrete conclusions from Baltimore county-level data), and public transport systems may not service areas of care, further complicating testing and treatment options for patients. Improvements in reducing these barriers to care would be beneficial in combating the HIV epidemic in the southern United States.
Provider misconceptions and patient stigmatization also emerged as a major theme. Perceptions of having low-risk patient populations while working in geographic areas with high prevalence of HIV infection suggest that education regarding local HIV epidemiology may be warranted to ensure that PCPs are aware; this may help PCPs take every opportunity to provide HIV prevention and education during clinical visits with patients. Previous research has shown that providers may hold misconceptions about patients, including age-related stereotypes (i.e., older patients being sexually inactive), 25 which our data corroborate.
Some of our respondents also used stigmatizing language regarding patients. HIV-related stigma exhibited by health care workers in the South is prevalent, and provider characteristics such as race, religion, and clinic type may predict stigmatizing attitudes. 26 –28 Research has also shown that personal values held by providers may interfere with discussing sexual behaviors with their patients, 25 and patient anticipated stigma in health care settings has been correlated with lower adherence to ART. 29 This underscores that targeted educational and stigma reduction efforts with providers in the southern United States, like those who participated in this study, are warranted.
Our results are subject to some limitations. First, our data may be biased toward PCPs who had interest in HIV, and therefore responded to our survey invitation and the free-text response question. We do not know the perspectives of PCPs who were invited and declined to participate in the survey or provide free-text responses (89% of 4595 with mailed surveys). Prepaid incentives may be a more effective approach to receive surveys back from clinical providers. Second, our study sample also had a large population of female respondents (71%), and ∼43% of all respondents were located in the Baltimore and Washington DC MSAs, limiting the generalizability of our results.
Third, our data were based on zip-code level information on provider practice location. Address-level data would have afforded more detailed GIS results. Similarly, we did not have access to zip-code level data for the Baltimore MSA, which prevented us from drawing more specific conclusions. However, the large sample size of our qualitative data set (n = 526) allowed for greater exploration and certainty of qualitative themes. By combining qualitative data with GIS data, we were able to see a more complete picture of the landscape of perceptions of HIV risk by PCPs in the South.
Our findings suggest that PCPs in the South may warrant support for addressing social barriers to more effectively provide care. Education regarding local HIV prevalence and routine HIV screening and prevention practices to strengthen clinical-level HIV services in the South is also warranted. By strengthening PCPs as frontline HIV providers in the South, the region most affected by HIV, we may be able to increase access to prevention and care for patients as part of national and regional HIV prevention efforts and improved health equity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was provided by US Centers for Disease Control and Prevention contract # 200-2015-F-87651.