
Abstract
Although there is ongoing debate over the need for substantial increases in pre-exposure prophylaxis (PrEP) use when antiretroviral treatment confers the dual benefits of reducing HIV-related morbidity and mortality and the risk of HIV transmission, no studies to date have quantified the potential added benefits of PrEP use and changes in its efficiency in the context of high treatment engagement across multiple US subpopulations. We used a previously published agent-based model to simulate HIV transmission in a dynamic network of Black/African American and White men who have sex with men (MSM) in Atlanta, Georgia (2015–2024) to understand how reductions in HIV incidence attributable to varying levels of PrEP use change when United Nations Joint Programme on HIV/AIDS (UNAIDS) “90-90-90” goals for HIV treatment are achieved and maintained. Even at achievement of “90-90-90” goals, 75% PrEP coverage further reduced incidence by 67.9% and 74.2% to 1.53 [simulation interval (SI): 1.39–1.70] and 0.355 (SI: 0.316–0.391) per 100 person-years for Black/African American and White MSM, respectively, compared with the same scenario with no PrEP use. Increasing PrEP coverage from 15% to 75% under “90-90-90” goals only increased the number of person-years of PrEP use per infection averted by 8.1% and 10.5% to 26.7 (SI: 25.6–28.0) and 73.3 (SI: 70.6–75.7) among Black/African American MSM and White MSM, respectively. Even with high treatment engagement, substantial expansion of PrEP use contributes to meaningful decreases in HIV incidence among MSM with minimal changes in efficiency.
Introduction
As the United States has set its sight on ending its HIV epidemic by 2030 (Refs. 1,2 ), no singular approach can eliminate wide-scale HIV transmission. However, strategies that combine pre-exposure prophylaxis (PrEP) and antiretroviral therapy (ART) as treatment as prevention (TasP) may hold promise toward meeting these ambitious goals. 3,4 The question remains as to how best to make use of these strategies in tandem, 5,6 and how this combination approach must be adjusted to suit unique qualities of distinct micro-epidemics within the United States. 6,7 Although there are many studies that use mathematical models to investigate the potential impacts expanding access to each of these prevention options independently, there are a few that investigate their combined effects, and none that explicitly compare their combined impact and efficiency on the dynamics of various domestic micro-epidemics. 8 –11
Moreover, there is ongoing debate over the need for combination approaches, specifically surrounding the value of broadly promoting PrEP use among HIV-negative individuals when the full benefits of high treatment engagement and TasP have yet to be fully realized. As PrEP has gained momentum, there has been caution of overuse of the high-cost intervention in low-risk populations, particularly from a health economics perspective. 11 Many wish to instead prioritize ART scale-up to reach global TasP targets, 12 advocating for the efficient, dual benefit it provides: improving health outcomes for those currently living with HIV while also being an effective prevention method. 4,13,14 However, a TasP-based approach may not be able to fully end the HIV epidemic in certain subpopulations. In particular, given the high burden of the HIV epidemic among Black/African American men who have sex with men (MSM) in the United States, high HIV prevalence may continue to sustain a high incidence rate even under circumstances of high treatment engagement, thus necessitating additional prevention options. 15
Notably, Black/African American MSM and other non-White MSM are disproportionately affected by the HIV epidemic in the United States. 16,17 Despite Black/African American MSM being no more likely to engage in condomless anal intercourse than White MSM, 18 there are substantial racial disparities in incidence and prevalence. 19 There are also inequities in access to and use of ART and PrEP that contribute to the widening of these disparities. 16,20 –22 Vulnerable populations experiencing high background prevalence and high incidence rates, such as Black/African American MSM in the United States, 23 provide a unique set of challenges that likely require combination strategies involving high treatment engagement to maximize the benefits of TasP, in addition to some level of PrEP use.
To this end, we leveraged an agent-based network model to investigate the added impact of PrEP expansion and changes in efficiency in the potential future with high levels of treatment engagement among Black/African American and White MSM, using the setting of Atlanta, Georgia as an illustrative case study.
Methods
Model setting
We used a previously published adaptation of the TITAN model, an agent-based network model, to simulate HIV transmission among White and Black/African American MSM in Atlanta, Georgia. 24 Agent-based modeling is a simulation method that executes micro-level interactions between individual entities, called agents, to generate population-level trends, such as HIV incidence. 25
All details regarding model structure and processes, parameter values, and model calibration can be found in a previously published supplementary appendix. 24 In brief, our model was primarily parameterized with estimates from the published literature of two studies conducted among White and Black/African American MSM in Atlanta, 23,26 with estimates drawn from others where necessary (Table 1). All parameters were race specific unless otherwise noted. Each iteration of the model simulated HIV transmission in discrete time-steps, each representing one calendar month for 10 years, and included population formation, network formation, and HIV transmission under varying levels of intervention engagement (see “Model Scenarios”).
Summary of Key Model Parameters
MSM, men who have sex with men.
Model processes
Population formation
The model began by initializing a virtual population of 17,440 agents (61.1% White, 38.9% Black/African American) who represented the estimated composition of all MSM aged 18–39 years in Atlanta, Georgia. 27 The agent population was dynamic and in steady state, where agents left the population at death or by aging out at 40 years. This age range was determined based on the underlying data 23,26 used to parameterize the TITAN model (see previously published supplementary appendix). 24 Agent attributes were assigned through stochastic processes to achieve the desired distributions (Table 1), with new, incoming agents drawn from these same set of distributions.
Sexual network formation
After population formation, the model created partnerships between agents to build a sexual network. All agents were assumed to participate in sexual behavior and were assigned a target number of annual sexual partners from negative binomial distributions. Using this target partner number, agents were tied together by using a partnering algorithm that reflected observed assortative mixing by race in the study setting. As the model progressed through monthly time steps, these ties formed and dissolved, generating a dynamic sexual network. Additional descriptions of these processes are included in the previously published supplementary appendix. 24
HIV transmission
The per-act probabilities of HIV transmission for condomless insertive and receptive anal intercourse were based on estimates from existing literature. An agent's probability of HIV acquisition was dependent on their assigned target number of sex acts per partner per month, the state of infection for the partner living with HIV infection (acute stage of infection, using ART, achievement of viral suppression), and any additional use of prevention interventions (condoms and PrEP). Types of partnerships were made variable through the averaging of partnered agents' target numbers of sex acts, creating partnership dynamics. 35
Intervention implementation
After seroconversion, agents moved through the HIV care continuum: diagnostic testing, engagement in ART, and achievement of viral suppression. An agent could test an unlimited number of times each year, but the model was constructed such that a set proportion of agents were required to test at least once per year and have the potential for diagnosis. Agents who initiated ART were assigned an adherence classification that would influence their probabilities of onward transmission and progression to AIDS. Agents engaged in ART were subject to a monthly probability of discontinuation and were not immediately replaced by new agents on discontinuation. Agents that discontinued ART had the potential to re-engage in ART with the same probability as those newly diagnosed at any time point.
All HIV-uninfected agents who were in an ongoing relationship with an agent living with diagnosed HIV infection or had two or more ongoing concurrent relationships and engaged in condomless anal intercourse had equal probability of engaging in PrEP. Agents were initialized with either optimal or suboptimal PrEP adherence that impacted the effect of the intervention. Agents engaged in PrEP had a monthly probability of discontinuation and would be immediately replaced with new agents on PrEP to maintain the desired population coverage set in each scenario.
Model scenarios
The main analysis compared HIV incidence across different treatment engagement scenarios and variable PrEP coverage levels within each of the treatment scenarios. The baseline treatment scenario maintained current (2015) estimates of treatment engagement for each race group (Fig. 1). 23 The model was calibrated to reproduce race-specific estimates of HIV incidence (2010–2014), 23 as previously discussed (Fig. 2). 24

Race-stratified estimates of current levels of HIV treatment engagement among Black/African American and White MSM in Atlanta
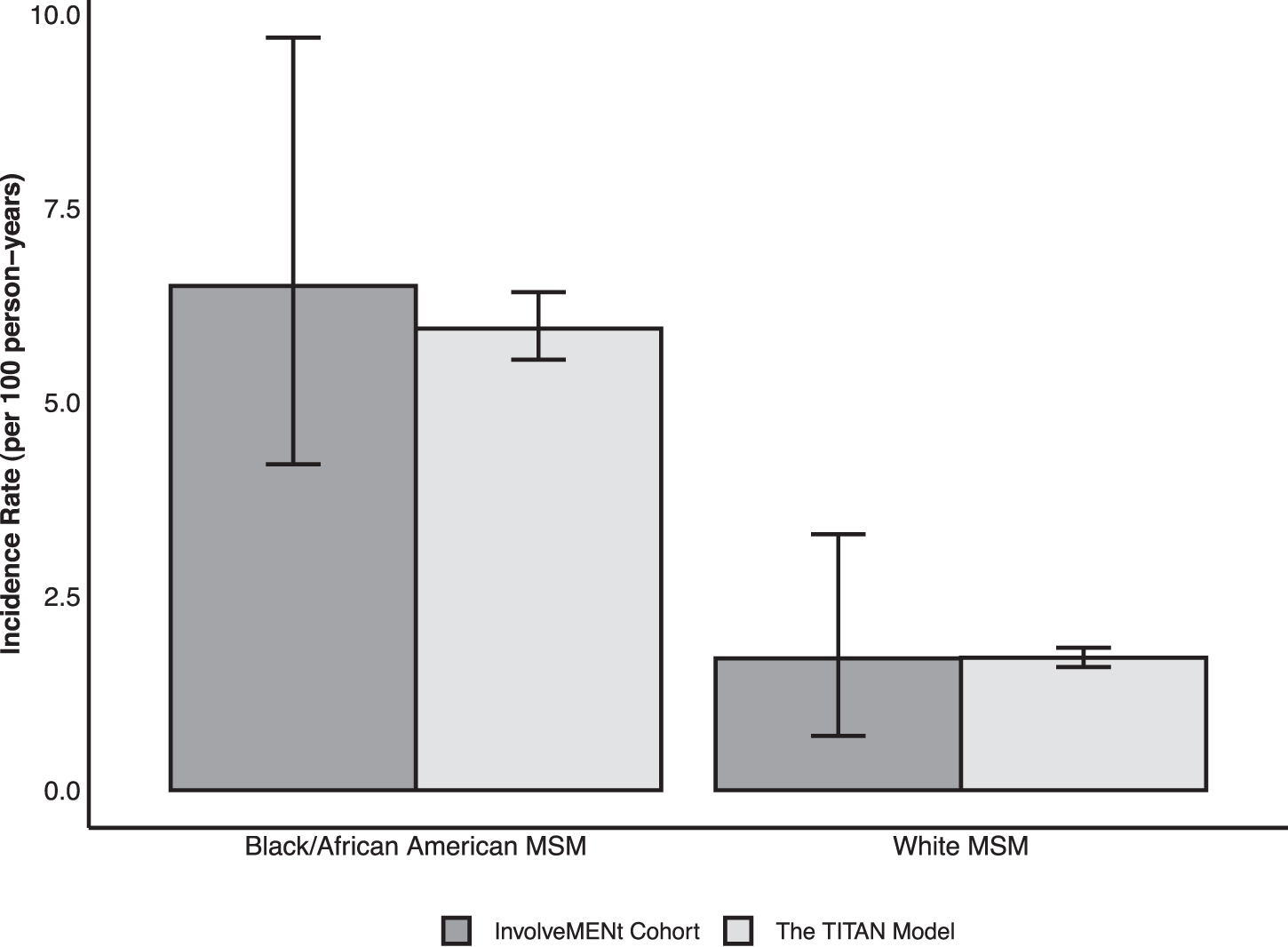
Comparison of observed HIV incidence among young Black/African American and White gay, bisexual, and other MSM aged 18–39 years old residing in the Atlanta–Sandy Springs–Roswell MSA who participated in the InvolveMENt study with 1000 simulations of the baseline scenario from this analysis using the TITAN model. Note: The error bars represent the 95% confidence interval for data from the InvolveMENt cohort and the 95% simulation interval from the TITAN model output. ART, antiretroviral therapy; MSA, metropolitan statistical area; MSM, men who have sex with men.
Subsequent treatment scenarios increased treatment levels to United Nations Joint Programme on HIV/AIDS (UNAIDS) “90-90-90” and eventual “95-95-95” goals in both racial subgroups to represent levels of treatment engagement that could result from prioritizing expanding ART. 12 These scenarios resulted in 72.9% and 85.7% of all agents with HIV infection achieving viral suppression, respectively (Fig. 1).
Within each of the treatment scenarios, we modeled PrEP coverage from 15% to 90% of all eligible MSM, in 15% increments. PrEP coverage levels were held equal across both race groups. Adherence to PrEP differed between race groups to reflect observed racial disparities in the study setting. A sensitivity analysis investigated the effect of parameterizing the proportion of Black/African American MSM with optimal adherence to PrEP to be the same as White MSM.
Outcome measures
The primary comparison outcome measures were the overall and race-specific incidence rates over the simulation period (2015–2024). The prevalence was also calculated at the beginning and end of each simulation. The absolute and percent reductions in incidence rates attributable to the addition of PrEP use for each group were calculated relative to the scenario with comparable treatment and the absence of any PrEP implementation (0% PrEP coverage). Lastly, race-specific values of the number of person-years on PrEP per infection averted were calculated as an efficiency measure. A total of 1000 iterations were conducted for each scenario, and all estimates are reported as mean values with 95% simulation intervals (SIs).
Results
Assuming current patterns of treatment engagement were maintained for 10 years with no PrEP implementation, the model predicted an overall incidence rate of 2.79 (SI: 2.64–2.95) per 100 person-years, initial prevalence of 29.4% (SI: 28.6–30.0%), and final prevalence of 46.8% (SI: 45.7–47.8%). The model predicted incidence rates of 5.95 (SI: 5.55–6.42) and 1.71 (SI: 1.59–1.84) infections per 100 person-years for Black/African American MSM and White MSM, respectively. The model showed initial prevalence of 53.3% (SI: 51.4–54.7%) and 14.2% (SI: 13.5–14.8%) for Black/African American MSM and White MSM, respectively. The model predicted a final prevalence of 76.9% (SI: 75.4–78.6%) among Black/African American MSM and 27.6% (SI: 26.4–28.9%) among White MSM.
Impact of immediate increases in HIV treatment engagement
Figure 3 displays the overall and race-specific incidence rates for the three treatment scenarios in the absence of PrEP implementation. When treatment levels are raised to “90-90-90,” incidence rates are reduced to 4.78 (SI: 4.37–5.08) among Black/African American MSM and 1.38 (SI: 1.28–1.49) among White MSM. When treatment levels are raised to “95-95-95,” incidence rates are further reduced to 4.44 (SI: 4.15–4.80) among Black/African American MSM and 1.27 (SI: 1.18–1.38) among White MSM. No scenarios produced a decrease in the prevalence at the end of the simulation compared with the initial prevalence.

Projected overall
Additional benefits of PrEP implementation
Figure 4 displays the absolute changes in overall and race-specific incidence rates attributable to the addition of varying levels of PrEP use within a given treatment scenario. Increases in PrEP coverage resulted in reductions in incidence in all scenarios. At the highest levels of treatment engagement (“95-95-95”), increasing PrEP uptake among all eligible MSM to 30% reduced the incidence rate among all MSM by an additional 0.65 (SI: 0.57–0.75) cases per 100 person-years, among Black/African American MSM by an additional 1.39 (SI: 1.17–1.60), and among White MSM by an additional 0.43 (SI: 0.35–0.49). These reductions corresponded to percent reductions of 31.3%, 31.2%, and 33.7%, respectively, as compared with the “95-95-95” treatment scenario with 0% PrEP engagement.
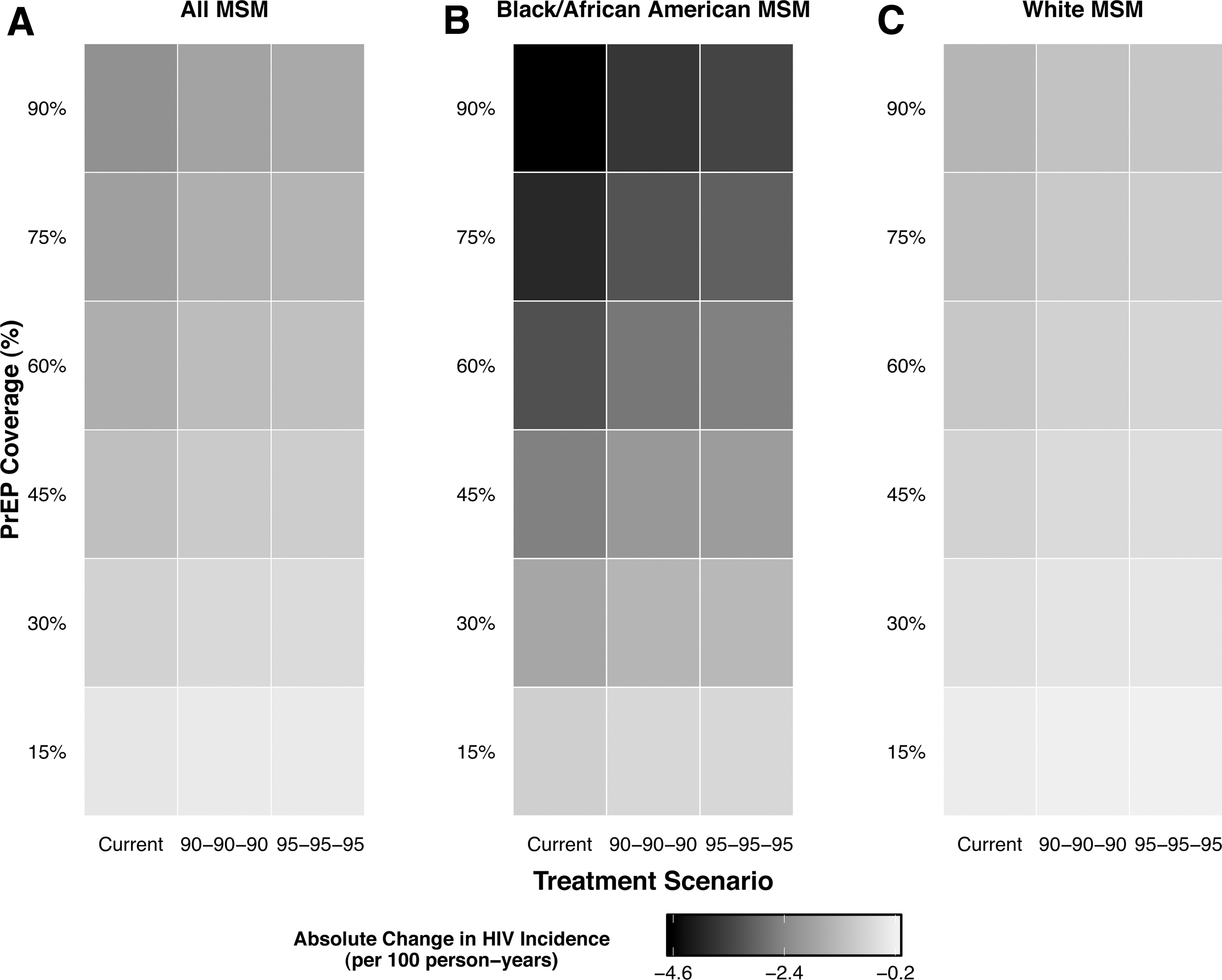
Overall
Remaining at “95-95-95,” an increase of PrEP uptake to an idealistic 75% of all eligible MSM reduced the incidence rate among all MSM by an additional 1.47 (SI: 1.43–1.50) cases per 100 person-years (70.0% reduction as compared with “95-95-95” with 0% PrEP engagement), among Black/African American MSM by an additional 3.04 (SI: 2.92–3.17, 68.3% reduction), and among White MSM by an additional 0.94 (SI: 0.89–0.98, 74.3% reduction). The marginal change in incidence due to increasing PrEP engagement lessened as treatment levels increased, but consistently increased as the proportion of MSM using PrEP expanded within each treatment scenario.
Changes in efficiency of PrEP
Figure 5 displays the race-specific values for the number of person-years on PrEP per infection averted across all scenarios. The number of person-years on PrEP per infection averted was substantially lower among Black/African American MSM than White MSM across all levels of varying intervention engagement. The number of person-years on PrEP per infection averted increased as levels of treatment engagement increased and as PrEP coverage was expanded for both Black/African American MSM and White MSM. The minimum number of person-years on PrEP per infection averted for both groups was under current levels of treatment engagement with 15% PrEP coverage: 21.5 (SI: 14.7–31.3) among Black/African American MSM and 51.9 (SI: 38.8–76.5) among White MSM. The maximum number of person-years on PrEP per infection averted for both groups was reached under “95-95-95” treatment goals with 90% PrEP coverage: 29.6 (SI: 28.5–30.7) among Black/African American MSM and 83.1 (SI: 80.6–85.46) among White MSM.
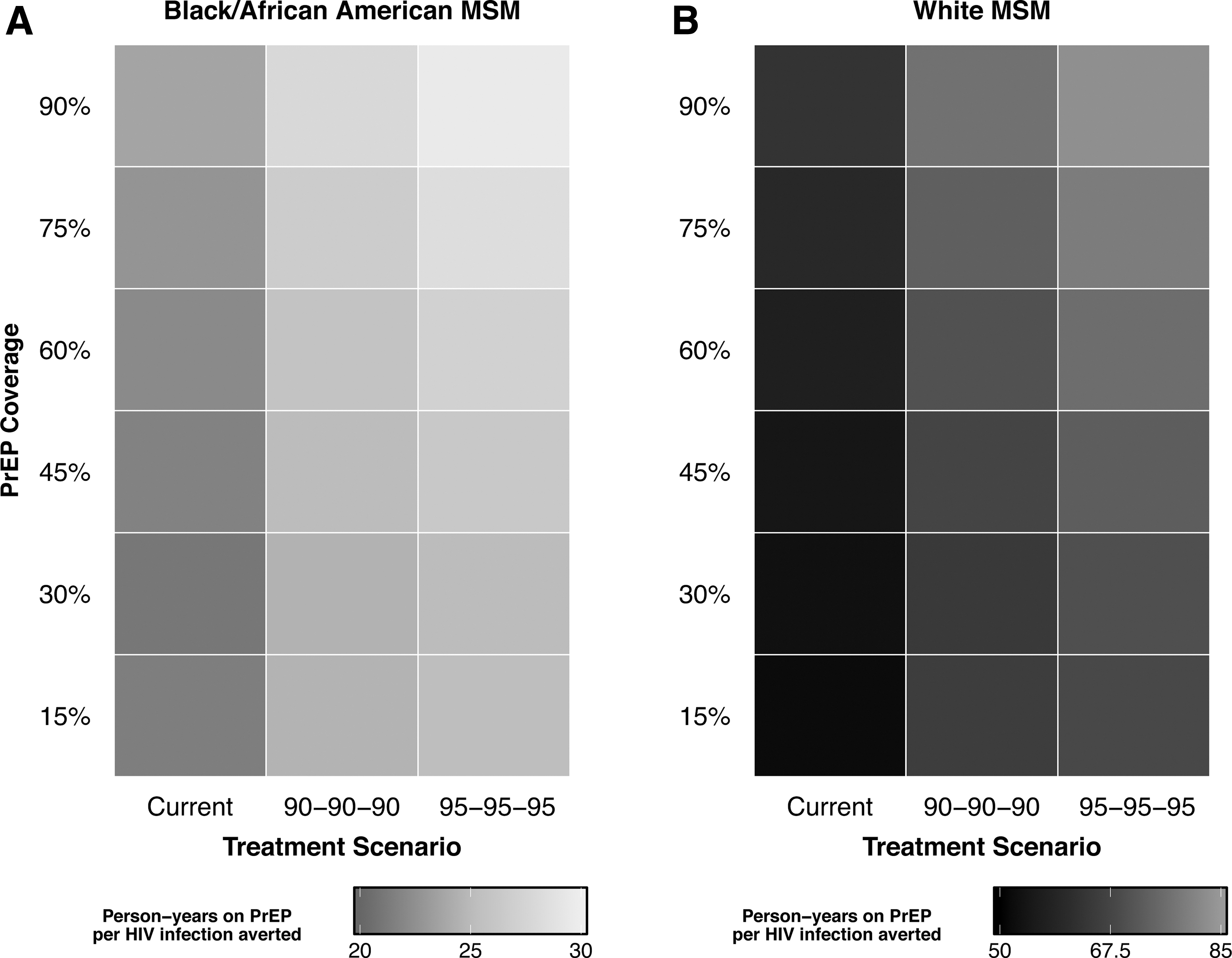
Person-years of PrEP use per HIV infection averted among Black/African American
Sensitivity analysis
Figure 6 displays a comparison of race-specific incidence rates when differences in PrEP adherence are left as observed or eliminated. The results were sensitive to eliminating the racial differences in PrEP adherence, where reductions in incidence rate among Black/African American MSM attributable to eliminating disparities in PrEP adherence increased as PrEP engagement expanded.
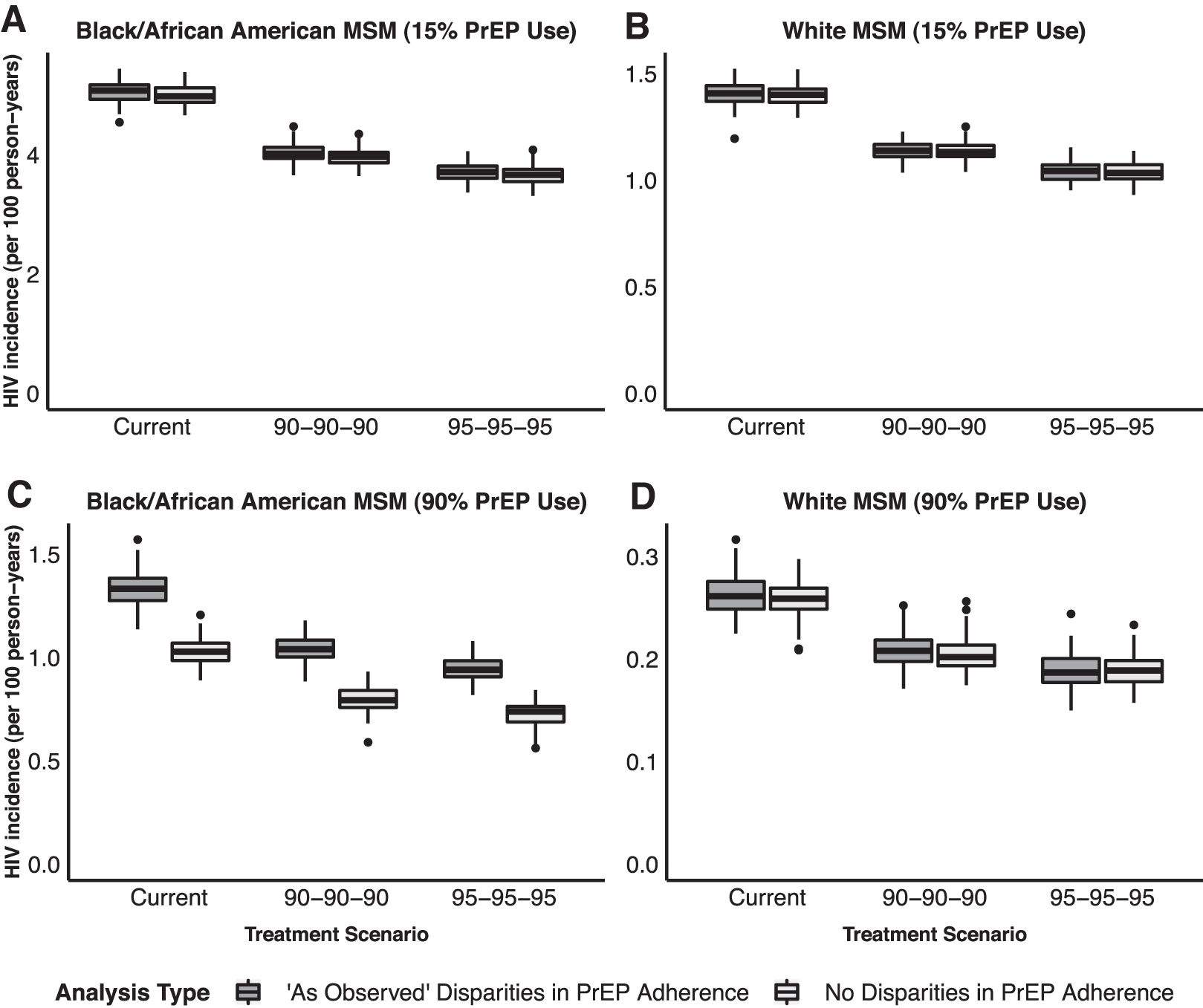
Race-specific HIV incidence among Black/African American and White MSM in Atlanta across scenarios of varied levels of treatment engagement among agents living with HIV infection and levels of PrEP use among HIV-uninfected agents.
Discussion
Although there are numerous simulation studies that examine the potential effects of combination HIV prevention and treatment options, 8 –11 we believe that this is the first study to explicitly measure the added impact of PrEP use and changes in efficiency in the context of high treatment engagement across racial subgroups in the United States.
Expanding treatment to “95-95-95” will be insufficient to reduce incidence rates by 90% within 10 years as outlined in the Ending the Epidemic Initiative. 1,2 Although expanding treatment to “95-95-95” levels results in a proportionally consistent reduction in incidence rates of 25% across White, Black/African American, and all MSM, this is an insufficient change for Black/African American MSM given the disparities of the current epidemic. These ideal treatment patterns reduce the incidence rate among White MSM to less than 2 cases per 100 person-years, but the incidence rate among Black/African American MSM remains well above 4 cases per 100 person-years. In comparison, an incidence rate of 1 case per 1000 years has been previously defined as a temporal milestone toward achieving HIV control. 36
Increases in PrEP coverage resulted in substantial additional reductions in incidence rates that remained proportional across White, Black/African American, and all MSM. However, larger absolute changes in incidence rates among Black/African American MSM were observed due to higher baseline incidence rates. Although the maximum incidence reduction of 87% among all MSM approached the 90% reduction goal, it required very high levels of treatment engagement (95-95-95) and PrEP use (90% of eligible MSM) and resulted in incidence rates that remained above the aforementioned HIV control milestone. These findings align with prior work that has demonstrated the need for targeted, context-specific combination implementation strategies to meet overarching national targets. 37
Importantly, our measure of PrEP efficiency (i.e., the number of person-years on PrEP to avert one infection) showed very little variation across coverage levels, particularly among Black/African American MSM. This finding suggests that PrEP has continued benefits, particularly among Black/African American MSM, even in circumstances of high treatment engagement. Given the high burden of the HIV epidemic among Black/African American MSM in the Southeast United States, 17,38 our results demonstrate that there is likely no strict upper bound for PrEP efficiency under high treatment levels in subpopulations where background prevalence is high enough to sustain a high incidence rate. These findings are, therefore, likely not limited solely to Black/African American MSM in the Southeast United States, but are relevant to other US subpopulations with high background prevalence, such as Hispanic MSM or smaller geographic US subpopulations. 16
These results support dramatic scale-up of PrEP use among Black/African American MSM and subpopulations with comparable disease burden, even in settings with extremely successful treatment engagement. Although there is high willingness among Black/African American MSM to use PrEP, 39 there are numerous structural 38,40 and social 41,42 barriers that prevent PrEP access and engagement. 43 We will be unable to realize the potential impact of PrEP without novel strategies that address both the structural and social barriers that impede PrEP access and uptake among Black/African American MSM. Although these levels of PrEP engagement may be unnecessary for all MSM in the United States or for prolonged periods, our results further support claims that scaling up PrEP among Black/African American MSM will be both efficient and necessary to achieve reductions in incidence rates in line with the national agenda. 1,2,9
Limitations
Although this research fills important gaps in the literature about the added impact of PrEP in the context of high levels of treatment, there are limitations. First, although data from studies involving MSM in Atlanta were used to parameterize the majority of the inputs, a limited number were derived from national level estimates. Although this has the potential to limit the representativeness of the model, 44 we are confident that, if present, the magnitude of this bias is minimal, due to the success of our model calibration. Second, this study was specific to the MSM subpopulation of Atlanta, Georgia, an illustrative, although discrete, context variable from other subpopulations experiencing high incidence. Third, our model assumes immediate implementation and maintenance of increased treatment engagement and PrEP coverage, whereas a gradual scale-up would be required for practical implementation. Fourth, there are multiple other intervention strategies not considered in our analysis employed as a part of combination strategies, including condom use campaigns, 8 campaigns to reduce numbers of sexual partners, 45 and other behavioral strategies. Although including these strategies was outside the scope of the current analysis, they likely play a substantial role in optimizing the interactions of PrEP coverage and ART engagement. Fifth, including cost-effectiveness analyses was beyond the scope of this analysis. However, we acknowledge that the cost of PrEP plays a substantial role in informing optimal combination strategies. 11 Future models should investigate the cost-effectiveness of PrEP expansion in settings that are also in need of increased treatment levels to better understand the practicality of expanding PrEP engagement. Finally, this analysis did not include scenarios designed to address and narrow racial disparities through equitable PrEP expansion nor equitable treatment engagement. As previously shown, increasing PrEP coverage without addressing racial disparities in incidence and prevalence may exacerbate the existing disparities. 16,22 In the future, we recommend extending the analysis to include scenarios that make use of metrics such as the PrEP-to-need ratio (the number of PrEP users divided by new HIV diagnoses), to more appropriately represent and address the variable states of subepidemics. 46
Even in the context of a highly successful HIV care continuum, the scale-up of PrEP coverage will be an efficient and necessary component in lowering incidence rates, particularly among Black/African American MSM in the United States. Notably, equitable PrEP expansion is needed, even in the context of high treatment levels, to appropriately address racial disparities in HIV incidence among MSM.
Footnotes
Acknowledgments
The authors would like to acknowledge the Brown University Centre for Computing and Visualization for providing access to the high-performance computing services utilized in this research. The authors would also like to thank Sam Bessey, MS, Maximilian R.F. King, ScM, and Jesse L. Yedinak, MPA for their research assistance.
Authors' Contributions
All authors have contributed substantially to the article, drafted and/or revised the work, approved of the final version, and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
The authors have no competing interests, financial or otherwise, to declare.
Funding Information
This work was supported by the National Institute on Drug Abuse (B.D.L.M, DP2DA040236) and the National Institute of Mental Health (W.C.G., F31MH121112 and R25MH083620).