
Abstract
As COVID-19 vaccinations became available in early 2021, we collected data from a US national sample of 496 people living with HIV (PLWH) to assess COVID-19 vaccination uptake and attitudes. The study was cross-sectional, and data were collected using an online survey between March and May 2021. At the time, 64% of the participants received at least one dose of a COVID-19 vaccine. Vaccine uptake was associated with older age and more years living with HIV, higher educational attainment, less vaccine hesitancy, and higher perceived COVID-19 vulnerability. Rates of vaccination uptake were highest among sexual and gender minority (SGM) cisgender men and transgender participants as well as those more likely to report undetectable viral load. Among the 166 unvaccinated, intention to receive the vaccine was related to older age and years living with HIV as well as lower vaccine hesitancy. Among the unvaccinated, SGM individuals demonstrated higher intent than non-SGM individuals. Findings indicate relatively high levels of vaccination in PLWH, although uptake and intent are not monolithic in the population. Patterns of vaccination are consistent with the health behavior literature in so much as those with higher levels of perceived heath vulnerability due to age as well as higher levels of proactivity about their HIV health are more likely to be vaccinated or intend to be vaccinated. Ongoing vigilance is required to vaccinate the US population, particularly those with underlying conditions such as HIV, as is the need to tailor health messaging to the highly diverse population of PLWH, with particular emphasis on the intersection of HIV and SGM status.
Introduction
Inequitable deadly pandemics, such as HIV and COVID-19, have magnified the deep-seated disparities evident in American society. 1,2 For the past four decades, the HIV epidemic has disproportionality affected marginalized populations, namely sexual and gender minority (SGM) men as well as Black and Hispanic/Latinx populations. 3,4 These epidemiological patterns are largely analogous in the COVID-19 pandemic where people of color are placed at higher risk for SARS-CoV-2 infection, hospitalization, and death. 5 Specifically, 34% of all COVID-19 deaths in April 2020 were Black/African American, although they only comprise 13% of the US population. 6,7 Recent studies have also documented that SGM men and lesbian, gay, bisexual, transgender, questioning/queer, and other SGM (LGBTQ+) people of color are placed at higher risk for SARS-CoV-2 infection than other subpopulations. 8,9 These vast disparities affecting marginalized communities resulting from systemic inequities within the United States are notably highlighted in worldwide outbreaks. 10 –12
At the onset of the COVID-19 pandemic, researchers and officials at the US Centers for Disease Control and Prevention (CDC) were concerned that people living with HIV (PLWH) might have an increased risk for severe illness if they contracted SARS-CoV-2 due to the high prevalence of comorbidities. 13 A study in New York City found that while PLWH were not overrepresented in COVID-19 cases compared with the general population, they had more adverse health outcomes due to COVID-19. 14 Although historically PLWH may have more exposure to public health messaging, the experiences of PLWH are not monolithic.
As COVID-19 has disproportionately affected structurally marginalized communities, in particular Black and Brown people and LGBTQ+ populations, 3,9,15 it is imperative to understand whether there are differences among these groups regarding overall COVID-19 vulnerability and vaccination uptake and intent among PLWH. While increasing access to the COVID-19 vaccine is critical to inoculation efforts, there is widespread vaccine hesitancy among adults in the United States, 16 particularly among Black, and Hispanic/Latinx individuals. 16,17
Presently, there is limited information on COVID-19 vaccination attitudes and hesitation among PLWH in the United States. 17 –19 Results from a French study found that 28.7% of participants found that hesitancy to be vaccinated for COVID-19, and those who reported history of antibodies, were significantly less likely to have received the vaccine. 18 In a study of PLWH in Miami, Black non-Latinx PLWH, compared with non-Black Latinx participants, were less likely to believe that vaccine information is reliable and trustworthy and that vaccines are effective in preventing COVID-19 disease. 19 Given the amount of misinformation and disinformation that has been spread around the COVID-19 vaccine 20 –22 and the potential adverse impact of COVID-19 on PLWH, it is important to understand the overall picture of COVID-19 vaccination uptake and intent among this population.
As COVID-19 vaccinations became available in the United States in early 2021, we collected data from a diverse national sample of PLWH to (1) describe rates of COVID-19 vaccination intent and uptake and (2) determine demographic, COVID-19-, and HIV-related factors associated with COVID-19 vaccine intent and uptake.
Methods
Study design
The study was cross-sectional in design, and data were collected using an online survey between March and May 2021. The purpose of this study was to understand COVID-19 vaccination uptake of PLWH in the United States. The inclusion criteria for this study required that participants (1) be 18 years old or older, (2) have received an HIV diagnosis before enrolling in the study, and (3) live in the United States or the US territories. The Rutgers University Institutional Review Board approved the study protocol (2021000063).
Procedures
Recruitment materials were distributed via three different channels: (1) professional and other community listservs (e.g., American Public Health Association, ACT UP, Gay and Lesbian Medical Association), (2) institutional social media accounts (e.g., Facebook, LinkedIn, Twitter), and (3) HIV service organization listservs (e.g., Ryan White Part A Grantees List and AIDS Education Training Center). The survey was distributed using Qualtrics and available in English only. Interested individuals first completed an online screening questionnaire to determine their eligibility. If eligible, participants provided online consent before completing the survey. At the end of the survey, participants were given the option to enter into a raffle to win one of two $60 gift cards. The survey was self-administered and took ∼10 min to complete. The sample for this study comprised 496 participants who met the inclusion criteria.
Measures
Participant demographic information included in the analyses was self-reported.
Age
Participants were asked to report their age in years. Participants 90 years old or older were recorded as 90.
Race and ethnicity
All participants were asked about their racial and ethnic identity. Participants could select from the following groups: Asian, Black or African American, Hispanic or Latinx, Native American or Alaska Native, Pacific Islander, White, or different identity with the option to specify. For analytic purposes, the responses were then collapsed into the following four categories: Black/African American non-Hispanic, Latinx/Hispanic, White non-Hispanic, and Other non-Hispanic racial and ethnic groups.
Education
Participants indicated highest level of education completed, which, for analytic purposes, were recoded into the following three categories: high school or GED or less, some college or associate degree, and bachelor's degree or more.
Employment
Employment status was as full-time employment, part-time employment, or unemployment.
Nation of birth
Participants were asked if they were born in the United States (yes/no).
Gender and sexual identity
Participants were asked to report their gender identity using the following categories: cisgender male, cisgender female, non-binary/genderqueer/gender non-conforming, transgender man, transgender woman, or different identity with the option to specify. For sexual identity, participants were asked to choose from the following categories: asexual, gay or lesbian, queer, heterosexual or straight, bisexual, or different identity with the option to specify. For analytic purposes, the sexual orientation and gender identity variables were collapsed into a single variable: sexual minority cisgender man, nonsexual minority cisgender man, sexual minority cisgender woman, nonsexual minority cisgender woman, and transgenders of all sexual orientations.
COVID-19 vaccine intent
Participants were asked about their intent to receive any of the COVID-19 vaccines using a single question (“How likely are you to take the COVID-19 vaccination when it becomes available to you?”) using a 5-point Likert scale. Very likely and likely were collapsed into one category and unlikely and very unlikely were collapsed into another. Unsure responses remained as recorded.
COVID-19 vaccine uptake
Participants were asked if they had received at least one dose of the COVID-19 vaccine and were able to select either yes, no, or unsure. For the purposes of these analyses, respondents who selected unsure were coded as missing. We note that participants who received the Janssen vaccine only required one dose. In our sample, this was only nine of those vaccinated.
Perceived COVID-19 vulnerability
Participants were asked about their perceived vulnerability to COVID-19 via two items: “Has a friend or family member been diagnosed with COVID-19?” and “Has a friend or family member died due to COVID-19?” Responses were collected dichotomously (yes/no).
Vaccine hesitancy
All participants were asked to complete the Vaccine Hesitancy Scale (Shapiro et al.). 23
HIV health indicators
Number of years since HIV diagnosis
All participants were asked to report the year that they received their HIV diagnosis.
Opportunistic infection diagnosis
Participants were provided a list of opportunistic infections classified as AIDS defining 24 and asked to identify ones they had experienced.
CD4 count
Participants were asked to report on their last CD4 count from the options: less than 200, 201 to 500, more than 500, and unknown.
HIV viral load
Participants were asked to report on their last viral load (polymerase chain reaction) from the options: undetectable, less than 500 but not undetectable, 500 to 5000, more than 5000, and unknown.
Analytic plan
We undertook descriptive analyses of participant demographic characteristics as well as COVID-19 vaccine uptake and COVID-19 vaccine intent. We then conducted bivariable analyses of the demographic characteristics by COVID-19 vaccine uptake and COVID-19 vaccine intent. Based on the bivariable analyses, we conducted binary logistic regression analyses for COVID-19 vaccine uptake as well as ordinal logistic regression analyses for COVID-19 vaccine intent. Participants who responded unsure for vaccine uptake were excluded from the analyses. All analyses were conducted using SPSS 26 (IBM). Participant ZIP codes were matched to state data using the postal (zip) code R 0.3.1 package in R 4.1.0 and mapped using QGIS version 3.14.15 (Open Source Geospatial Foundation).
Results
Survey participants (n = 496) were average age of 50.08 years [standard deviation (SD) = 0.61; range, 19–78 years] at the time of the survey and were diverse in terms of race and ethnicity and other demographic factors (Table 1 and Fig. 1). Gay cisgender men made up the largest proportion of participants (n = 226, 45.6%), followed by heterosexual cisgender women (n = 101, 20.4%).
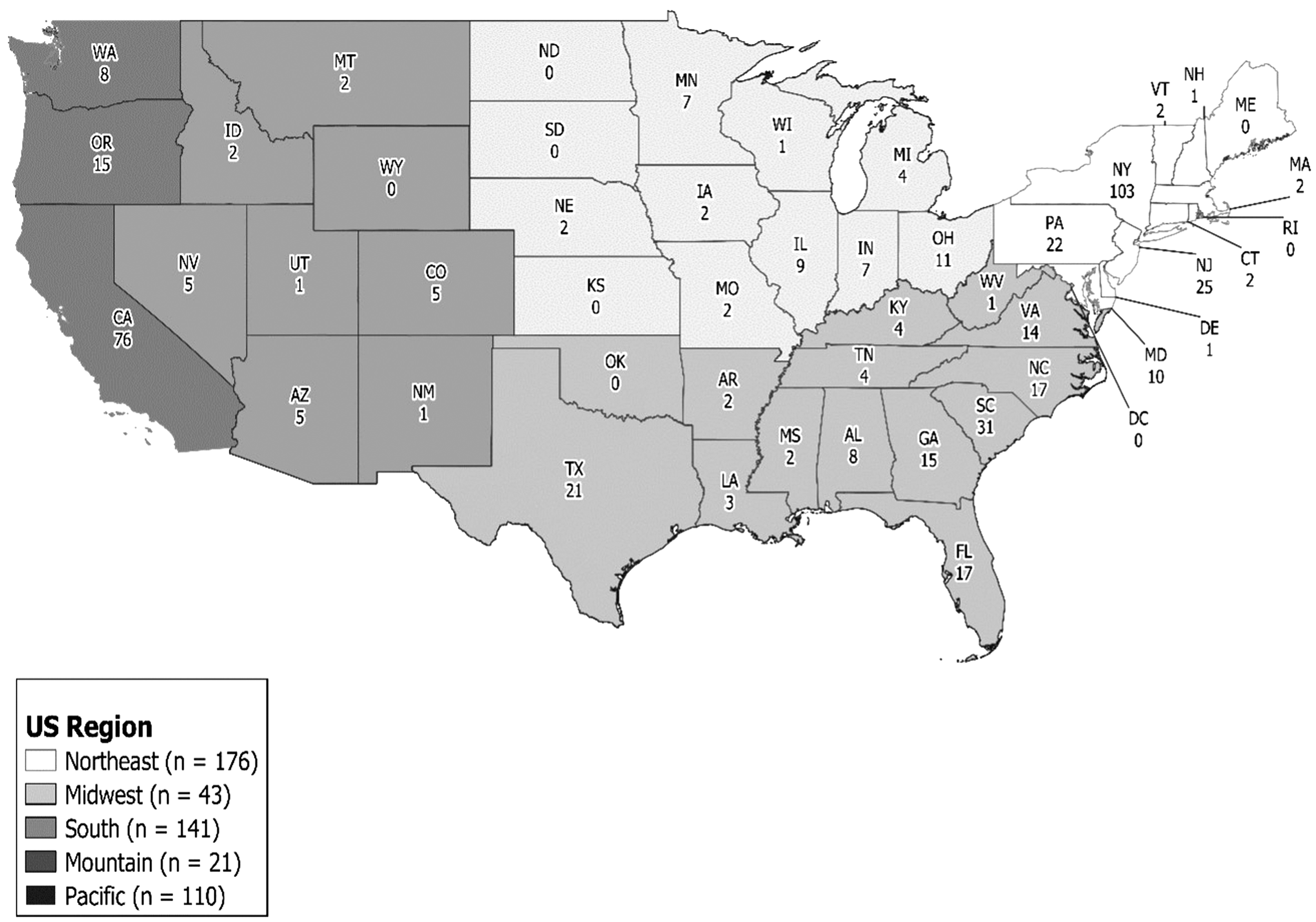
Number of participants, by region and state, in a nationwide survey of COVID-19 vaccine hesitancy among PLWH (n = 496), United States, 2020. Pacific region includes three participants who resided in noncontiguous states and territories: Alaska (n = 2), Hawaii (n = 1).
Sociodemographic Characteristics of Participants in a Nationwide Survey of COVID-19 Vaccine Hesitancy Among People Living with HIV (n = 496), United States, 2021
OI, opportunistic infection; SD, standard deviation.
COVID-19 vaccine uptake and intent
Of the 496 participants, 310 (62.5%) reported that a friend or family member was diagnosed with COVID-19 and 158 (31.9%) participants had a friend or family member who died due to COVID-19. A large proportion of participants received at least one dose of a COVID-19 vaccine (n = 319, 64.3%). Of these, 149 (46.7%) participants received the Pfizer/BioNTech, 144 (45.1%) participants received the Moderna, 13 (4.1%) participants received AstraZeneca, 9 (2.8%) participants received the Johnson & Johnson, and 4 (1.3%) were unsure. Of those who had not received a COVID-19 vaccine at the time of the survey, 110 (66.3%) stated that they intended to receive the vaccine when it becomes available to them.
Vaccine uptake was associated with age, education, sexual orientation and gender identity, vaccine hesitancy, COVID-19 vulnerability, number of years since HIV diagnosis, and viral load (Table 2). Participants who had received at least one dose of any of the COVID-19 vaccines were older on average than those who had not received a dose. Participants who received at least one dose of a vaccine had less vaccine hesitancy and had been living with HIV for a longer period of time than those who had not received a dose. Participants who had a family member or friend who was diagnosed with or who died due to COVID-19 also were more likely to have received at least one dose of the COVID-19 vaccine. Finally, participants who reported an undetectable viral load indicated higher rates of vaccine uptake (68.6% vs. 55.6%; χ 2 = 5.52; df = 1; p = 0.02). Lower vaccination rates were noted among SGM versus non-SGM individuals (p < 0.001).
COVID-19 Vaccine Intent and At Least One Vaccine Dose Received Among People Living with HIV in a Nationwide Survey, by Sociodemographic Characteristics, United States, 2021
The total sample for receiving at least one dose of a COVID-19 vaccine was 485 because missing (n = 1) and unsure (n = 10) were treated as missing. SD, standard deviation.
We then examined those factors to explain COVID-19 vaccine uptake intent (defined as yes, no, and may be) among those who had yet to receive a dose of vaccination (n = 166; Table 2). Those who intended to receive the COVID-19 vaccine were older than others in the sample. We found that participants who did not intend to receive a COVID-19 vaccine reported higher levels of vaccine hesitancy [mean (M) = 2.99, SD = 0.69] compared with the uncertain (M = 2.46, SD = 0.46) and intended (M = 1.93, SD = 0.65) groups. Also, those who intended to receive the COVID-19 vaccine had a higher average number of years since their diagnosis of HIV than the may be and no groups. Finally, variability was noted across sexual and gender identity groups with more than 70% of both SGM men and transgender participants, regardless of sexual identity, indicating vaccine uptake, with lower rates reported by non-SGM participants and SGM women (p < 0.001). Among the unvaccinated, similar patterns are reported for intent (p < 0.01).
Multi-variable modeling in the form of binary logistic regression analyses was utilized to explain vaccine uptake (Table 3) and ordinal logistic regression models to examine vaccine intent (Table 4). The model for vaccine uptake was significant (χ 2 = 49.03; df = 15; p ≤ 0.001; classification fit = 67.5%). When controlling for all other factors, participants who held a bachelor's degree or more education had 1.79 [95% confidence interval (CI) 1.02–3.14, p < 0.05] times higher odds of receiving at least one dose of a COVID-19 vaccine compared with participants with a high school degree, GED, trade school degree, or less education.
Binary Logistic Regression Models Examining COVID-19 Vaccine Access Among Participants in a Nationwide Survey of People Living with HIV, United States, 2021
The total sample for multi-variable logistic regression was 462 due to missing data.
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
p Values in bold < 0.05.
Ordinal Logistic Regression Models Examining COVID-19 Vaccine Intent Among Participants in a Nationwide Survey of People Living with HIV, United States, 2021
The total sample for the unadjusted sexual orientation and gender identity model and the multi-variable ordinal logistic regression were 174 due to missing data.
p Values in bold < 0.05.
Furthermore, the adjusted ordinal logistic regression model for vaccine intent was significant (χ 2 = 61.78; df = 7; p < 0.001) and assumption of parallel lines was not violated (χ 2 = 7.28; df = 7; p = 0.400). Specifically, higher levels of COVID-19 vaccine hesitancy were significantly associated with lower vaccine uptake intent. A one unit increase in vaccine hesitancy score was associated with a 0.18 (95% CI 0.10–0.32) lower odds of either not planning or being uncertain about receiving the vaccine holding all other factors constant.
Discussion
This study contributes to the extremely limited knowledge available on the impacts of COVID-19 in the lives of PLWH, specifically as it relates vaccine intent and uptake in this population. The majority of this sample (64%) reported receiving at least one dose of a vaccine, which was significantly higher than the national average at the time of data collection (March–May 2021). 25 Despite this relative success, patterns were not monolithic with results demonstrating vaccine hesitancy and low uptake among some subgroups. In particular, this study found that participants who had been living with HIV a longer period of time were more likely to have received at least one dose of the vaccine, as were those that reported an undetectable viral load. These findings align closely with a recent study of Black Americans living with HIV. 17
We also note that Black participants in this sample constitute the group least likely to be vaccinated. These findings should be considered in light of studies that have demonstrated the relation between race and residential segregation for individuals infected with HIV 26,27 and COVID-1928 in the United States, with people of color tending to live in less economically advantaged neighborhood. These patterns, in turn, affect outcomes, where higher rates of mortality due to HIV 29,30 and COVID-19 infections 31,32 are linked to poverty. In effect, these patterns replicate in COVID-19.
Moreover, such racial disparities are observed in HIV vaccine and treatment trials. 33 Taken together, these findings suggest that successfully managing COVID-19 and HIV is predicated largely on continued access to trusted health care providers and trusted sources of health information, which likely affects decision-making around vaccine uptake as well as treatments for both HIV and COVID-19. Importantly, access to care is lower for people of color living in poverty. 34
Indeed, the COVID-19 pandemic has set back the federal and state “Ending the Epidemic” plans by disrupting the HIV prevention and care continuum, particularly for those at the margins of society. 35,36 Increasing and maintaining access to HIV-related care and services for underserved populations are urgently needed as the pandemic continues to surge, as engagement in care may engender trust in COVID-19 health information and recommendations and thus serve as an effective avenue for encouraging COVID-19 vaccination uptake.
Recent studies on the broader US population have observed lower COVID-19 vaccine acceptance among younger adults. 37,38 This finding also emerged among our sample of PLWH. Older individuals likely feel placed at higher risk for severe COVID-19 complications, suggesting that public health messaging around the importance of vaccination must evolve to reach younger populations, many of whom have largely expressed significantly less concern about contracting COVID-19. 39 Promoting preventative health measures among young groups can be difficult as other research has shown low rates of preventive health care utilization and the need for health promotion among this demographic. 40
Engaging young PLWH in consistent medical care and promoting the benefits of U = U [i.e., antiviral therapy (ART)] adherence leading to an undetectable viral load) and other preventative health measures, such as the COVID-19 vaccine, are of paramount importance. However, we also note that that our study finding may be linked to date of data collection, when the vaccine was largely available to the older population. Still, as time has progressed, younger adults continue to be less likely to receive COVID-19 vaccination than their older peers, 65 years and older. 41
In our study and across other studies of US-based populations, lower educational attainment was also associated with lower vaccine intent and acceptance. 37,38 Although educational attainment can be a useful proxy for ascertaining potential access to and acceptance of trustworthy sources of health information, it is important to address the extent to which misinformation and disinformation have powerfully shaped the response to the pandemic, including at the federal, state, and societal levels. 22,42 In a recent study of COVID-19-related trust, health information sources, and social relationship/health service disruption among PLWH in Georgia (United States), the authors found high rates of inaccurate information about COVID-19 among participants, as well as low levels of trust in CDC and government sources of health information. 43
Similarly, in a study of COVID-19 mistrust among Black PLWH, nearly all participants endorsed some type of COVID-19 mistrust idea, and more than half endorsed mistrust beliefs related to the COVID-19 vaccine and treatment, as well as greater COVID-19-related mistrust was associated with increased vaccine and treatment hesitancy, suggesting an urgent need to address misinformation. 17 Although our study suggests that many subgroups of PLWH have been vaccinated or intend to obtain the vaccine, our findings also call for tailored efforts to address misinformation about PLWH.
Drawing upon strategies employed in the HIV epidemic, the Popular Opinion Leader (POL) approach may be an effective method of engendering trust and confidence in public health COVID-19 messaging. 44 In Wisconsin, researchers are recruiting POLs who are social media influencers, predominantly Black and Latinx, who will be closely engaged with their communities and who will share trusted sources of health information. 44 Given the need for trusted social media and community leaders across various sociodemographic groups, the POL approach is a promising strategy to begin dismantling government and public health mistrust.
Disparities in vaccine uptake and intent by gender and sexual orientation also were documented in this study. Uptake was highest among sexual minority cisgender men, as well transgender participants, and intent was also highest among these groups compared with SGM women and non-SGM individuals. This may be due in part to interactions with health care, especially poorer communication with non-SGM, as was found in a study of PLWH men who have sex with women. 45 Heterosexual men living with HIV may have less access to health resources, as a large proportion of HIV services are oriented toward sexual minority men, 46 and thus, straight men may not tap into the same networks that provide trusted information about COVID-19.
Other studies have also found that cisgender women are less likely than people of other genders to obtain the vaccine, citing concerns about safety and efficacy. 47 Cisgender women may be concerned about the potential effects of the COVID-19 vaccine on fertility and reproductive health, 48 although these concerns, while widespread, are not supported by scientific evidence. 49 Messaging and vaccine outreach efforts must directly address how vaccine concerns may be gendered in unique ways.
Finally, although the study presented here did not detect any differences in vaccine intent and uptake by race and ethnicity, perhaps due to smaller cell sizes for groups of color, the broader literature points to structural racism as a driver of lower vaccine uptake among minoritized communities, and White supremacy-driven disinformation as a key factor explaining vaccine hesitancy and low uptake among groups of largely conservative, White Americans. 22,50 –52 Both types of mistrust require innovative strategies that do not apply blanket responses to vaccine hesitancy. For PLWH of various sociodemographic backgrounds, it is essential that communication of health information signals a genuine understanding of various communities' concerns and acts in partnership to address the hesitancies.
Limitations
The data reported in these analyses are time-bound. Given the ever-evolving nature of the COVID-19 pandemic, these findings must be nested within the time frame that the data were collected, specifically in spring 2021. This was a at a time when individuals with underlying conditions were fully eligible, namely Phase 1c, although those older than 75 years, those living in long-term care facilities, and those who were health care personnel and/or essential workers would have been eligible in the first two phases. 53 As with any self-reported data, the finding are subjected to social desirability. Still, the consistency of the data within our survey provides us with higher levels of confidence, as we also undertook procedures to prevent the infiltration of bots. 54
Additionally, small cell sizes also require the collapsing of race and ethnicity data. However, more than 50% of the respondents did not identify as White, and thus, we achieved a relatively diverse sample. Of course, the data are dependent on accurate representation of PLWH. Given our targeted recruitment and the responses to HIV-related questions, we also have a high level of certainty in the constitution of the sample. Although cross-sectional data are always subjected to spuriousness, the findings align with the extant literature on health behaviors across sectors of PLWH. Finally, the study was limited that it was only available in English, although the survey had an elementary school reading level.
The findings of our investigation reveal the extent to which existing structural inequities have become reinforced, sustained, and amplified by the inadequate and negligent government and societal response to the COVID-19 pandemic. Vaccine outreach efforts must take special care to reach out to subgroups for whom vaccine uptake has lagged, including young PLWH, sexual minority women and nonsexual minority men living with HIV, and those who are less engaged in HIV care. To do so successfully, public health and medicine must address the particular ways misinformation might affect PLWH. Finally, ensuring uninterrupted access to HIV care, as well as increasing access for underserved populations, is a key strategy to not only facilitate progression along the HIV prevention and care continua but also provide access to trusted sources of health information that encourages vaccine uptake.
Ethical Approval
The study protocol was approved by the Institutional Review Board of Rutgers University.
Consent
Informed consent was obtained from all participants.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding provided for this study.