
Abstract
Pre-exposure prophylaxis (PrEP) is an effective biomedical strategy for HIV prevention. This umbrella review is aimed at providing a comprehensive summary of the current status of each stage of the PrEP care cascade. A systematic literature search was conducted in PubMed, Embase, and Cochrane. Additionally, a Measurement Tool to Assess Systematic Reviews 2 (AMSTAR-2) tool and Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) checklist were used to evaluate their methodological and reporting quality, respectively. A total of 30 systematic reviews met the inclusion criteria. According to the results of methodological quality assessment, 3 reviews were rated as low, while 27 as critically low. Furthermore, the results of the reporting quality evaluation revealed a mean score of 23.03 for the included reviews. Across all the reviews, awareness of PrEP was generally moderate in all populations, and the acceptability was even higher compared with awareness. Unfortunately, the PrEP uptake among different groups was even less optimal, although the adherence was almost above moderate, and several barriers that hindered the utilization of PrEP were identified, and the most common are as follows: cost, stigma, lack of knowledge, mistrust, low risk perception, and more. Although PrEP has proven to be an effective prevention method to date, the promotion of PrEP failed to achieve the anticipated outcome. To reinforce the generalization of and use of PrEP, and effectively control HIV transmission, it is urgent to identify the underlying causes of low uptake rates so that efficient interventions can be implemented.
Introduction
Pre-Exposure Prophylaxis (PrEP) is a specific antiretroviral medication prescribed to individuals who have not contracted HIV before engaging in behaviors that make them susceptible to HIV infection to prevent HIV. 1
During the COVID-19 pandemic, disruptions to HIV services and a slower public health response to HIV led to increased infections, 650,000 people died because of HIV-related diseases, and 1,500,000 people were newly infected with HIV in 2021. 2 Furthermore, by the end of 2020, the “90-90-90 target” (90% infected people will be diagnosed, 90% of those diagnosed with HIV will receive ART, and 90% of those who receive ART will have the virus suppressed) issued by UNAIDS in 2014 3 was not achieved. There are several high-risk behaviors and situations for easy HIV acquisition, 4 for instance, engaging in unprotected anal or vaginal sex; having already infected with other sexually transmitted diseases, such as Syphilis, HSV, Chlamydia, gonorrhea, bacterial vaginosis; inappropriate use of alcohol and drugs in a context of sexual activity; sharing contaminated needles, syringes, and other injecting equipment when injecting drugs, all pose significant risks. Exactly, men who have sex with men (MSM), sex workers, people who inject drugs (PWID), serodiscordant couples are more likely to engage in these mentioned behaviors. 2
Above vulnerable populations around the world are disproportionately burdened by HIV. Specifically, cisgender women who engage in sex work, and/or use drugs have considerably higher HIV prevalence than their peers. 5 In numerous countries, MSM account for the majority of incident HIV cases, as observed in the United States. 6 Most HIV infections are heterosexual, with marital transmission being the prevailing scenario, this is particularly evident as more than 90% HIV-positive women are married and in a monogamous relationship. 7
According to the US Centers for Disease Control and Prevention, in recent years, the government had made a significant progress in the program of implementing PrEP among susceptible populations, with only 3% of 1.2 million people who were recommended for PrEP taking PrEP in 2015, but it increased to 25% by 2020. 8 But, after all, PrEP is used with a high degree of autonomy, and global PrEP use remains limited on the whole. By the end of 2020, only 920,000 people worldwide had initiated oral PrEP, 9 for example. To better measure progress in the implementation of PrEP programs, Nunn et al. 10 proposed the model “pre-exposure prophylaxis care cascade” to assess multiple steps related to PrEP acceptability, uptake, and adherence. The model indicates that each stage of the cascade must involve the patient, the HCP, and other key stakeholders in the system. 11 It is similar to the HIV treatment cascade, particularly in the identification of high-risk groups and the successive phases of treatment initiation and adherence. 12 Accordingly, the PrEP Cascade is a heuristic framework for familiarizing each step or stage of PrEP care and implementation, from identifying population susceptible to AIDS to individuals retained in PrEP care. 13
Although this cascade may vary slightly in specific steps across different studies, 5,11,14 there is a common goal of identifying gaps between HIV care to target future interventions. 15
Since PrEP has become the most effective means of targeting HIV, the number of studies on PrEP among different populations has increased dramatically in the last decade, as has the number of systematic reviews and meta-analysis. Many of the reviews are aimed at a particular population or stage of the PrEP care cascade or a particular region, and often present inconsistent conclusions. But no studies have documented and summarized the results of relevant reviews and assessed their quality. Therefore, it is necessary to comprehensively evaluate the various stages of PrEP among different populations, and make an overall assessment of their qualities based on the comprehensive evidence grading criteria. An umbrella review is an overarching systematic review conducted for decision makers as the number of existing systematic reviews increases. 16,17
Given the importance of PrEP care to the AIDS high-risk groups, this overview of systematic reviews was designed with a significant emphasis on comprehending the present status of the PrEP care cascade and barriers or facilitators associated with the implementation of PrEP among diverse populations, and provide empirical evidence for future research and practice in this field. The ultimate objective is to enhance the effectiveness of PrEP care and contribute to the overall prevention and management of HIV/AIDS.
Methods
This systematic review of systematic reviews and meta-analyses followed the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guidelines. 18 We registered the protocol in PROSPERO (ID: CRD42023421747) prospectively.
Search strategy
A literature search was conducted in three prominent databases, including PubMed, Embase, and Cochrane Library in January 2023 and updated on April 11, 2023. To ensure a comprehensive coverage of relevant studies, a combination of keywords and medical subject heading (MESH) terms related to our subjects were used to search the literatures: HIV, acquired immunodeficiency syndrome, PrEP, pre-exposure prophylaxis, and other similar terms. To search more accurately and comprehensively, we adjusted the search strings to suit different databases. Detailed search terms of each database were listed in Supplementary Table S1.
Inclusion and exclusion criteria
Studies that met the following criteria were included: (1) systematic reviews utilizing meta-analysis, qualitative systematic review, or a combination of both; (2) at least one outcome related to the PrEP care continuum of patient-or-provider level was reported; (3) discussion of barriers or facilitators associated with PrEP implementation; (4) full text could be found; and (5) published in English. We exclude literatures if they were original articles and protocols instead of systematic reviews or meta-analyses, if they did not include any outcomes along the PrEP care cascade, or if they were conference abstracts and presentations.
Study screening and data extraction
All references identified through the search process were imported into ENDNOTE. By scanning the titles and abstracts, the literatures that did not meet the standards were screened and removed by two reviewers (G.J. and J.D.), independently. Then they assessed the full texts to exclude ineligible articles after removing duplicates. In cases where there were disagreements between the two independent reviewers, resolution was achieved through the discussion with the rest of the team members. 19
The other two reviewers (H.S. and H.G.) extracted information of included studies into Microsoft Excel Software following a predefined format. Extracted data items were as follows: (1) first author, (2) the year of publication, (3) the number of original studies included, (4) total sample size, (5) total number of events, (6) the study-specific sample sizes (only for systematic reviews with a meta-analysis), (7) the study-specific numbers of events (only for systematic reviews with a meta-analysis), (8) study type, (9) population studied, (10) country, (11) the tool for quality/bias assessment, (12) the rationale for not performing a meta-analysis (only for systematic reviews without a meta-analysis), (13) 95% confidence intervals (CI; only for systematic reviews with a meta-analysis), and (14) key findings. A third author (G.Y.) resolved the discrepancies in the data extraction. 20
Assessment of quality and epidemiological credibility
The methodological quality and reporting quality of all included studies were accessed using Assessment of Multiple Systematic Review (AMSTAR-2) 21 and PRISMA 2020 checklist, 18 respectively. AMSTAR, published in 2007, is a practical tool for assessing the quality of systematic reviews. 22 However, some researchers have pointed out some problems with it in the use of AMSTAR. 23 As a result, the research team collaborated with experts from various fields, revamped AMSTAR and officially published the second edition of AMSTAR-2 in September 2017. 21 The AMSTAR-2 tool consists of 16 items, 24 although each step of the systematic evaluation is important, 7 of which were selected by the research team as critical items affecting the production of systematic reviews and the validity of their results: items 2 (research protocols), 4 (literature search strategies), 7 (list of excluded studies and reasons), 9 (bias assessment methods), 11 (statistical analysis methods), 13 (the impact of bias risk), and 15 (publication bias), 25 and the remaining 9 items are noncritical items.
The AMSTAR-2 also advises on methods for grading the credibility of results: (1) “high”: if there is none or only one noncritical deficient, (2) “moderate”: if there is more than one noncritical area deficient, (3) “low”: there are deficiencies in one critical area and/or nonimportant areas, (4) “critically low”: there are deficiencies in more than one critical area and/or nonimportant area. 26
PRISMA checklist was developed using an evidence-based approach whenever possible, with the overall goal of helping to ensure clarity and transparency in the reporting of systematic reviews. 27 It contains 27 entries (42 subentries) in 7 sections: Title, Abstract, Introduction, Methods, Results, Discussion, and Other information. Each item was rated as “Yes” (a score of 1), “Partial Yes” (a score of 0.5), or “No” (a score of 0) based on whether it is fulfilled. 28
GRADE is a transparent framework designed to provide a clear set of criteria across different domains to assess the level of evidence and make recommendations for clinical practice. 29 It was used to classify the quality of evidence for the secondary outcome indicators included in this umbrella review. In total, there are eight factors that may affect the quality of GRADE evidence, 30 of which three are upgrade factors, including large magnitude of effect, plausible confounding, and dose-response gradient. 31 The remaining five are downgrade factors, including: study limitations, inconsistency of results, indirectness of evidence, imprecision, and reporting bias. Because 9/10 included studies were observational and predetermined to be “low-level” evidence, only upgrade factors were evaluated; 32 the one remaining meta-analysis contained randomized controlled studies (RCTs) with high starting quality, evaluating both upgrade factors and downgrade factors. If the magnitude and intensity of any one of the three factors meet the criteria, the evidence may be raised by one level to intermediate (such as relative risk >2) or by two levels to high.
Finally, the quality of evidence was graded according to the total score: ≥0: high-level evidence; −1: intermediate level of evidence; −2: low level of evidence; or less than or equal to −3: very low level of evidence. The assessment of quality and epidemiological credibility was carried out by the first author, with any uncertainty discussed with the other team members in conferences.
Synthesis of results
Despite the emergence of this framework (HIV care continuum) for PrEP implementation, gaps remain in the studies on the application of all steps of the PrEP care continuum to systematic reviews and meta-analyses such as those included in this umbrella review. 33 We searched all systematic reviews and meta-analyses on PrEP and found that there was no way to encompass all of the steps proposed by Nunn et al. into this review, so relevant adjustments were made as appropriate. Now, we conducted an umbrella review of published systematic reviews and meta-analyses of public PrEP awareness, PrEP acceptability, PrEP uptake, PrEP prescribing, PrEP adherence, and barriers and facilitators. During the full-text reading, the findings were reviewed and coded using inductive and deductive content analysis, which was led by the first author. More specifically, after the full-text review of the extracted literatures, the first and senior authors collaboratively identified overlapping themes in the literature and created coding definitions. The two reviewers independently coded the data included in the study according to the themes that had been set. The coding of outcomes for the PrEP cascade is shown in Table 1 below.
Pre-Exposure Prophylaxis Care Continuum Outcomes of This Umbrella Review
PrEP, pre-exposure prophylaxis.
Results
Search results
A total of 656 articles were identified in the initial search, 536 of which were reserved after duplicates were removed. Through the process of screening the titles and abstracts, 53 remained. During full-text review, we ruled out literatures that were not eligible for our criteria; in other words, 30 relevant studies were included in this umbrella review in the end (Fig. 1). For transparency, the specific documents that were excluded during the full-text review, along with the reasons for their exclusion, were provided in the Supplementary Table S2.
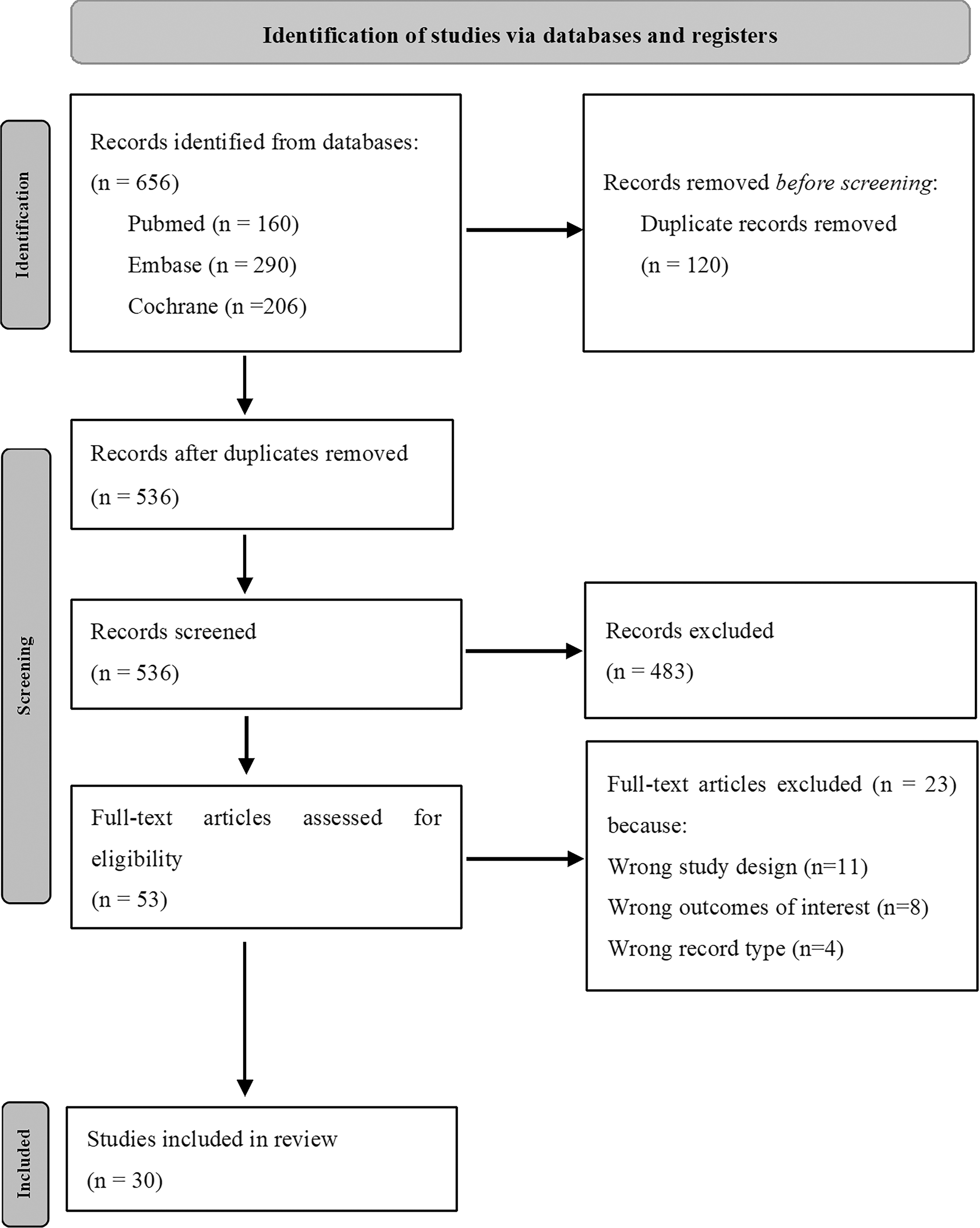
The selection process of studies included in this review.
Characteristics of included studies
Table 2 summarizes the main characteristics of the final 30 reviews included in this overview, which consisted of 20 systematic reviews (SRs), 9 systematic reviews with meta-analyses, and 1 meta-analysis. All the eligible studies were published after 2012, with ∼1/3 reviews reported on PrEP in the United States, and quite a few reviews summarized global data related to PrEP. The reviews encompassed diverse study populations—MSM, 14,34 –42 transgender women/men, 36,42 –44 PWID, 12,45,46 and health care providers (HCPs). 11,47 Regarding the assessment of quality and risk of bias in individual studies, two SRs and one SR with meta-analysis were conducted based on the Mixed Methods Appraisal Tool. Additionally, one used the Cochrane Collaboration's tool, another one used a modified Critical Appraisal Skills Programme (CASP) Qualitative Checklist and Joanna Briggs Institute Checklist, and one used a quality assessment tool. One review utilized the Effective Public Health Practice Project (EPHPP) tool and CASP tool, one used the PREFS checklist, and another used the GRADE rating scheme.
Characteristics of the Included Systematic Reviews/Meta-Analyses
CASP, Critical Appraisal Skills Programme; CI, confidence interval; DCE, discrete choice experiment; EPHPP, Effective Public Health Practice Project; FSW, female sex workers; HCP, health care provider; MMAT, Mixed Method Appraisal Tool; MSM, men who have sex with men; MTC, medication-taking coverage; NHLBI, National Heart, Lung, and Blood Institute; NR, not reported; NS, not specified; OR, odds ratio; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; PWID, people who inject drugs; PWUD, people who use drugs; RCT, randomized controlled study; RDBPCTs, Randomised Double Blind Placebo Controlled Trials; STI, sexually transmitted infection; WWID, women who inject drugs.
Two reviews used an adapted Newcastle–Ottawa Quality Assessment Scale, one used an adapted version of an existing tool, and one review employed three assessment tools (NHLBI, 2019; the EPHPP, 2019; the Critical Appraisal Skill Program, 2019 qualitative checklist). Furthermore, one review used the Jadad scale and one employed the National Heart, Lung, and Blood Institute (NHLBI) study quality assessment tool. The rest of the reviews did not conduct any assessment.
Reporting, methodological quality, and epidemiology credibility
In this umbrella review, the PRISMA checklist was used to evaluate the reporting quality of literatures, the results showed that the scores of each review included in this overview ranged from 13.5 to 32.5. Based on the results, only four items (Q1, Q3, Q4, and Q6) in the PRISMA statement were adhered by all studies. All of the reviews had some deficiencies in the quality of reporting; this is mainly due to the fact that no review provided the register name and registration number in abstract (Q2) and explained any amendments made to the protocols (Q24c), although eight reviews registered a formal protocol before the literature search. One-third of the reviews had a score below 20, which had serious defects, with reporting gaps mainly in search strategy, synthesis methods, effect measures, reporting bias assessment, certainty assessment, results of individual studies, and synthesizing results. Outputs of reporting quality are displayed in the Supplementary Table S3. 48
The quality of three reviews was assessed as low, and the remainder was judged as critically low using the AMSTAR-2. For the seven critical items of AMSTAR-2, none of the reviews met all the conditions, which is why there is a lack of high-level and mid-level credibility studies, and we found that few reviews (n = 2) provided a list of excluded studies and the exclusion reasons for exclusion. As mentioned earlier, only a small number of reviews developed a preliminary study protocol before conducting the systematic review did not satisfy the item 2. Even though 10 systematic reviews performed meta-analysis, few reviews evaluated the impact of individual study risk of bias on the results of meta-analysis. Further detail on the results of methodological quality assessment is shown in Fig. 2. 49
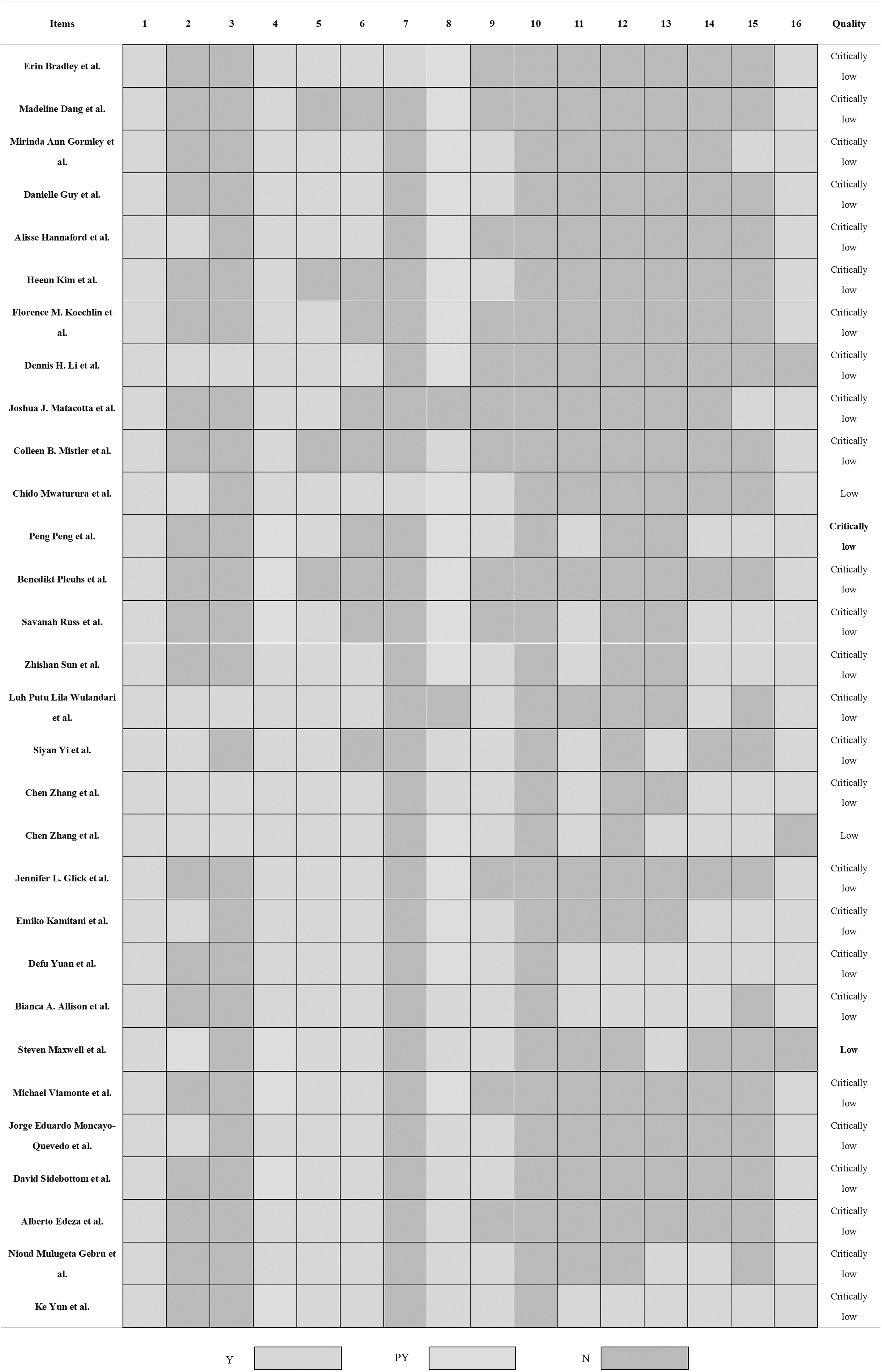
Results of the AMSTAR-2 assessments.
There are 10 systematic reviews and meta-analyses involving 92 factors that influence different stages of the cascade of PrEP. In terms of GRADE, ∼29.7% were rated high, 26.7% were rated medium, and 43.6% were rated low. Seven of 10 systematic reviews and meta-analyses explored 76 factors related to acceptability to take PrEP, the most frequent of which were age, education, condom use, and sexual partners. Six reviews investigated the association between age and willingness, four of which were rated medium in quality of evidence and two were rated low. Of the five reviews that evaluated the association between education and PrEP acceptability, two were rated as high quality, one was rated as medium quality, and the remaining two were rated as low quality. But when it came to exploring whether condom use was associated with acceptance, the quality ratings of the same five reviews changed, with four of them being intermediate quality and only one being low quality. We assessed four reviews exploring sexual partners and acceptability on a quality scale, with one being high level, two intermediate, and one low level. Besides, three reviews have examined various factors related to adherence.
All three analyzed whether age affected adherence, and one was found to have high-quality evidence, while the other two were of low. In addition, one review reported not only predisposing factors for acceptance but also for awareness. Among the influences reported in the review, age and transactional sex had moderate effects on awareness, while having conversations about HIV prevention had a high impact on awareness. The results of the quality of evidence for the meta-analyses included in this study are presented in Table 3.
The Results of the Quality of Evidence for the Meta-Analyses
MTC, medication-taking coverage; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.
PrEP continuum of care
PrEP awareness
In total, eight SRs and five SRs with meta-analyses examined PrEP awareness among various populations. Among these, the awareness of MSM and PWID was frequently discussed. The three systematic reviews and meta-analyses 14,38,39 reported the pooled prevalence of awareness in MSM, one of which based on global data reported a pooled estimate of 50%, whereas awareness rate of PrEP in low- and middle-income countries was lower, accounting for 29.7%. 39 Besides, reviews reported >1–66% knowledge 5,12,45 46 among PWID. One review specifically focused on women who inject drugs (WWID) and reported a relatively narrow range of 4–36.5% awareness. Yet the other two ranges (>1–57% and 7–66%) were much wider. Also, the PrEP awareness was associated with many factors, for example, WWID who participated in transactional sex, had prior knowledge about HIV prevention 45 and PWID with a college education, and had received a sexually transmissible infection test, 12 were more likely to be aware of PrEP. In addition, there was evidence 12,45 to prove that women's knowledge of PrEP was superior to men.
Two reviews discussed PrEP awareness in HCPs; the pooled proportion of awareness was calculated in a meta-analysis (68%, 95% CI: 55–80%). 47 It was also observed that the PrEP knowledge had risen steadily between 2009 and 2015. 11
PrEP acceptability
There were also 13 reviews 1,5,11,12,14,37 –39,45 –47,50 –52 that delineated willingness to use PrEP and variables related to PrEP acceptability. Women or PWID were involved in five of them, and the range of data varied widely (23–100%). 1,5,12 45 Besides, three reviews highlighted that WWID appeared more interesting in PrEP compared with men who inject drugs. 5,12,45 Furthermore, four meta-analyses evaluated acceptability among MSM, and the pooled prevalence all >50%. 14,37 –39 Regarding HCPs, the willingness to prescribe to people was 60–92% according to two reviews. 11,50 In short, the overall acceptability was moderate. In addition, a stronger interest in PrEP was linked to people who were younger, had higher income, perceived high HIV risk, had condomless sex recently, had received HIV testing, had access to learned PrEP previously, received higher education, insurance coverage, and high effectiveness of PrEP based on nine reviews. 1,5,12,14,34,45,50,51,53
PrEP uptake
In fact, literatures on the use of PrEP were not extensive. As a result, six reviews 5,12,14,40,46,54 discussed the use of PrEP, and one meta-analysis 11 calculated pooled proportion of health care professionals who had prescribed PrEP. The findings indicated that the rates of PrEP uptake were dissatisfactory. A systematic review 54 that summarized the results of the PrEP care cascade for patients in emergency departments reported the percentage of patients initiating PrEP therapy, ranged from 1.2% to 2.2%. Likewise, the use of PrEP among PWID minimal, ranged from nonexistent to 3%. 12 While outcomes from two meta-analyses showed that the PrEP uptake among Black MSM and HCPs ever prescribed PrEP was slightly higher, 15.5% (95% CI: 12.8–18.2%) 14 and 24% (95% CI: 17–32%) 11 respectively, also a review 40 investigated a prevalence of PrEP use among MSM, reporting a range of 9–12% in 2015.
PrEP adherence
All nine reviews included compliance with PrEP and factors relevant to poor adherence. Four of these reviews provided specific pooled estimates or numerical ranges, adherence to PrEP ranged from 5.6% to 52.3% among WWID, 45 and the pooled percentage of adherence in adolescents and young adults was 64% (95% CI: 57–71%). 38 In studies focusing on MSM, adherence rates were found to be over 70%. 42 Another review examining adherence in female and younger subjects reported an overall pooled medication-taking coverage of 59.9% (95% CI: 43.1–74.6%). 55 It is important to note that definitions and ratios of PrEP adherence varied across different reviews. In the systematic review assessing the states on PrEP continuum among cisgender women, 5 the adherence was defined as taking the medicine as prescribed, and reported fluctuated rates with the passage of time in both South Africa (70–85%) and Benin (finally declined to 43.3%). Nevertheless, the adherence was characterized as taking four or more pills every week according to another review, 40 in addition, it is recorded that the adherence (drug levels) after 24 weeks (20–84%) and 48 weeks (34–80%) are nearly the same.
The poor adherence mainly rooted in stigma, medical mistrust, low-risk perception, dosing regimens, and concerns about side effects. 14,46 Likewise, the PrEP adherence was also concerned with substance use such as drugs, alcohol, stimulants, etc. 42 It was also recorded that age was similarly a factor that influences adherence. 55
The overall descriptive data of included studies are shown in Figs. 3 and 4.

A descriptive forest plot of included meta-analyses by PrEP Awareness, PrEP Willingness, PrEP Uptake, PrEP Adherence and different populations. Pooled prevalence among different populations. MSM, men who have sex with men; PrEP, pre-exposure prophylaxis; WWID, women who inject drugs.
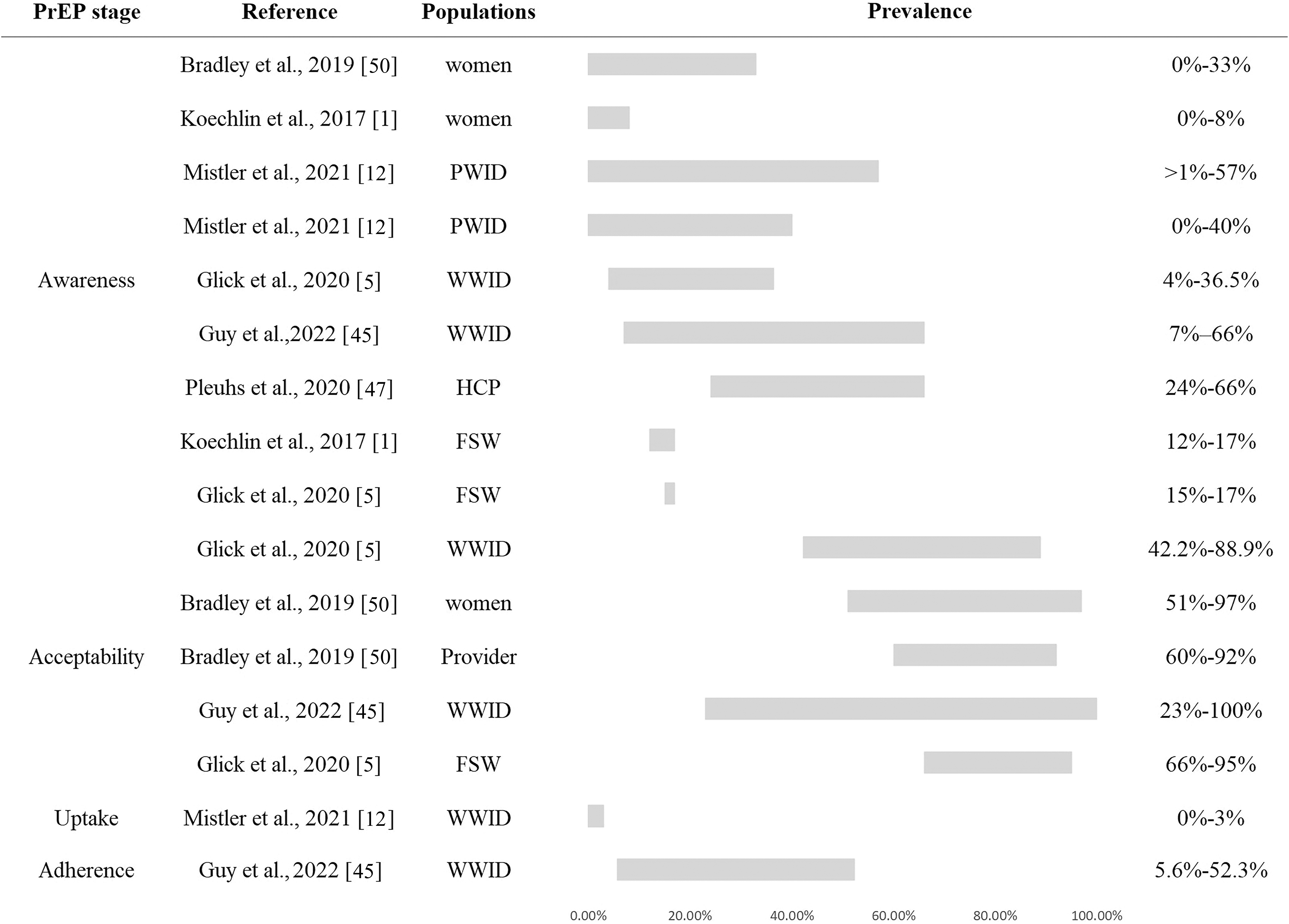
A descriptive bar chart of included systematic reviews by PrEP Awareness, PrEP Acceptability, PrEP Uptake, PrEP Adherence and different populations. The range of prevalence among different populations. FSW, female sex workers; HCP, health care provider; PrEP, pre-exposure prophylaxis; PWID, people who inject drugs.
Barriers or facilitators
To some extent, the effectiveness of PrEP depends on whether people actually take the medication. But there were plenty of factors that influenced the implementation of PrEP. Understanding how to better promote the use of PrEP for HIV prevention among HIV-susceptible populations who wish to utilize it is a critical step toward ending the epidemic and promoting health equity. 56 Overall, 15 reviews 1,11,35 –37,41,43 –45,47,50,52,53,57,58 examined factors that either promote or hinder PrEP uptake. Five of them adopted a prespecified methodology to identify and classify contributory factors. Similarly, we categorized contributory factors according to the populations included in the study.
Women
Three reviews 1,50,58 on influencing factors of PrEP in women underscored the significance of cost and stigma as formidable barriers. Women indicated that they were reluctant to take out-of-pocket money to pay for PrEP, and harbored feelings of discomfort when broaching topics concerning PrEP or HIV. At the individual level, partners' anticipated reaction emerged as another critical factor in the women experiencing intimate partner violenc 58 ; they worried about partners' reactions if they expressed a desire for PrEP. Moreover, a myriad of impediments, including adherence challenges, low-risk perception, mistrust, negative experience, side effect, 50 dearth of comprehensive information, concerns about effectiveness were identified. 1
For facilitators, the number of reviews was somewhat limited. Although partners' attitudes may hinder female real thoughts, partner and peer support could encourage women to initiate PrEP, particularly when peers possessed knowledge about PrEP. 1,50 Furthermore, the significance of daily use and adequate knowledge transcended their classification as mere barriers, also functioning as facilitators based on the study. 50 Moreover, familiarity with pills, fear of HIV/desire HIV prevention, trusted information sources and recommendations, risk reduction, and adherence strategies were identified as instrumental in fostering PrEP uptake.
Health care providers
We identified five reviews 1,11,47 50 illuminated prevailing themes concerning barriers or facilitators related to providers across the 30 studies. HCPs concurred that cost of drugs, lack of PrEP education, providers' lack of time, 50 negative experiences with health care, stigmatization, side effects, drug resistance, and patients' ability to adhere 11,57 could reduce PrEP utilization. Otherwise, credible evidences, such as more efficacy data, and providers' ability to link patients to other HIV services, exhibited potential to engender heightened interest in PrEP. At the HIV specialists level, their collective belief that PrEP was better suited for general primary care setting, 1,57 lack of prescription knowledge, stigmatization and biases, 1 as well as the absence of established lack of PrEP care models 11 were significant barriers to PrEP prescription. Whereas the likelihood of prescribing PrEP increased if providers possessed PrEP training or sufficient knowledge, a firm belief in the high efficacy of PrEP, and a genuine desire to help more people at risk. 1,50
Men who have sex with men
The barriers and facilitators of MSM were measured in five reviews. 35 –37,41,57 Most reported stigma about HIV and gay men was the strong barrier, HIV-related stigma could lead to fear of PrEP, and effect to mental health directly. 36 Also, PrEP uptake was challenged by insufficient knowledge, and inconvenient location for those living in rural areas exacerbated this problem. 37 Homophobia, lack of access to LGBT-affirming care, difficulties integrating PrEP into daily routines, and the perception that PrEP promotes promiscuity, 41,57 challenges to adherence, 36 cultural barriers, financial concerns, as well as a personal preference for condoms 37 were reported as impeding implementation factors by the four studies. Nonetheless, willing to use PrEP was positively linked to greater recognition of HIV risk, favorable attitudes about PrEP, 57 online posts which revealed stimulus, 36 convenience of having sex without condom, as well as accessibility and location of the PrEP provider. 37
People who inject drugs
Research pertaining to barriers or facilitators for PrEP uptake in PWID remained relatively scarce. However, the available literatures shed light on key factors influencing PrEP utilization within this population. However, PWID regarded access to providers, homelessness, cost, daily medication requirement, continued condom use, and periodical HIV tests as barriers. 1,45 In the comprehensive review, 45 sexual assault, higher income, and inconsistent condom use were essential to increase the willingness to use PrEP.
Transgender population
Regrettably, the successful implementation of PrEP among transgender individuals was hindered by various factors. These included the lack of transgender-specific messaging, HIV stigma, concern about increased intimate partner violence, lack of awareness, lower income, lack of social support, mental health issues, and gender-affirming hormones. 36,43,44 A notable review conducted in the United States showed remarkable positive associations between gender affirmation and PrEP uptake. 43
Discussion
Umbrella reviews, situated at the apex of the evidence-based medicine hierarchy, represent one of the highest levels of integrated evidence available. 59 In addition to analyzing and synthesizing the results of systematic reviews and meta-analyses, the umbrella reviews evaluate the quality of the evidence more prudently, and objectively recommend them according to the evidence, so as to provide referential suggestions for clinical practice, medical decision making and orientation for further studies. 17 With the aim of expediting the achievement of the “90-90-90” target as soon as possible and better understand the global landscape of PrEP, this review endeavors to consolidate the current state of affairs along the entire PrEP continuum of care across diverse populations at risk.
This overview of systematic reviews and meta-analyses synthesized the results of 30 systematic reviews and meta-analyses and evaluated each state of PrEP care continuum among different populations. In all reviews published between 2016 and 2022, the cause of this phenomenon might be that the World Health Organization extended the PrEP use to encompass all people who were likely to infect HIV in 2015. 60 According to the results of the quality evaluation of this overview, the methodological and reporting quality of the included studies was poor, especially the methodological quality was critically low in most reviews, which is also inevitable in other umbrella reviews. 61 –63 We still conducted the present study because the field currently lacks a comprehensive summary of the cascade of PrEP care, and then we can alert the researchers based on the low quality of the results of this quality assessment; in future it should take more time to get a high-quality systematic review that provides strong evidence for clinical research.
However, precisely due to the lack of high-quality systematic reviews and meta-analyses, researchers need to further standardize the implementation of future studies, and it is also hoped that the original studies on PrEP will be of higher quality to provide high-quality literature for systematic reviews and to enhance the strength of evidence. In the process of future systematic evaluations, high-quality literature should be included as much as possible to enhance the evidence strength and to provide guidance for clinical workers. Systematic review practitioners are needed to be trained in methodology and reporting, and implementation is to be carried out in strict accordance with AMSTAR-2 and PRISMA.
Even though the GRADE results on quality of evidence showed that there was no very low level of evidence on affecting the implementation of PrEP, the proportion of low-grade evidence was still close to 50%, which suggests that the estimated effects of PrEP implementation factors are quite different from the true effects, and further research may alter the evaluation results. Moreover, for the same influencing factor, the quality of evidence varies from study to study. For example, in six reviews 34,37 –39,46,51 investigating the relationship between age and acceptability, the quality of evidence was graded as either moderate or low. Two of the above six assessed the effect of age on the acceptability of PrEP for MSM globally, but one 37 was rated as intermediate and the other 38 as low. However, in my opinion, the latter has a more credible rating of evidence, because they are both based on global data and the same population, with the latter's publication year being updated and the sample size being larger.
For the five reviews that assessed the impact of education on the acceptability of PrEP, two were high-quality evidence, one based on global coverage and the other published just last year, so we are confident that education has a significant impact on the acceptability of PrEP. However, we are only moderately confident that the real situation is likely to be close to the estimated effect as to whether condom use affects acceptability. This is because four 34,37,38,51 of five reviews were rated as moderate, and although one review 39 was rated as low, it was published in 2017, while the other four were published in 2018 and later. As for the qualitative credibility of the factors influencing adherence, we consider its rating to be low, with a limited degree of certainty. As for the qualitative credibility of the factors influencing adherence, we consider its rating to be low with limited certainty. Among the three relevant reviews, 14,55,64 66.6% were rated as low. For the studies investigating the stages of PrEP care cascade, the vast majority were observational studies; even one had a high rating because it included RCTs with a high starting quality, which could have created bias.
This study shows that most of the evidence levels are fair, but there is still some heterogeneity in the evidence among different studies. In consequence, future studies need to further optimize the study design to address the above shortcomings and choose the right statistical methods to provide more accurate and high-quality evidence.
Among the systematic reviews, which reported the range or pooled estimate of each stage of PrEP implementation cascade, the most extensively discussed group was MSM, followed by WWID/PWID. As is known to all, knowledge of PrEP serves as a prerequisite for the use of PrEP. Generally speaking, the awareness rates were found to be moderate to low level (0–68%) across populations. Three SR with meta-analyses identified the pooled estimates of awareness among MSM, two of which drew similar conclusions (50.8% 14 and 50.0% 38 ), but one result was lower (29.7%) 39 compared with them. The lower data (29.7%, 95% CI: 16.9–44.3%) was derived from low- and middle-income countries, while the other two were based on the global (50.0%, 95% CI: 44.8–55.2%) and American (50.8%, 95% CI: 43.6–58.0%) data. Consequently, the discrepancy may be attributed to different economy environments, with individuals in the low- and middle-income countries having fewer opportunities to access PrEP.
As for awareness in PWID/WWID, the main reason why the 2 ranges (>1–57% and 7–66%) compared with the range (4–36.5%) were larger could ascribe to the latter range being based on data from only 2 original studies that measured PrEP awareness, however, the former 2 came from 19 and 14 studies that collected awareness data, respectively. In terms of HCPs, their knowledge was not as comprehensive as expected, although the overall trend was increasing, and PrEP knowledge was positively correlated with prescription rate. 47 Collectively, even though awareness of PrEP was varied in different groups, the prevalence needs to be improved owing to limited knowledge. Therefore, enhancing awareness among HCPs becomes crucial, as it increases the likelihood of them recommending PrEP to potentially at-risk populations once they are more informed about its effectiveness. This, in turn, can contribute to increased knowledge of PrEP within these high-risk groups.
According to the data presented, people showed greater interest in PrEP in general. Studies have indicated that PrEP is considered an acceptable strategy for HIV prevention. 5 By comparing relative data, there appears to be minimal disparity in the willingness to use PrEP among WWID, female sex worker, and MSM, with all groups falling within the upper-middle range. On account of the association between acceptability and knowledge, age, income, high-risk perception, HIV testing, education level, focusing on aforementioned areas to integrate PrEP services may be a practical solution to facilitate acceptability. By improving knowledge about PrEP, targeting specific age groups, addressing income disparities, promoting risk perception, encouraging regular HIV testing, and providing education and information, the acceptability of PrEP can be further facilitated.
Compared with PWID, the proportion of MSM and providers who had used or prescribed PrEP was much higher. For instance, the ratio in MSM (15.5%, 95% CI: 12.8–18.2%) and providers (24%, 95% CI: 17–32%) were superior to PWID (nonexistent to 3%). This gradient in PrEP use may be due to the fact that MSM are traditionally considered as a key population for HIV prevention, leading to a higher preference for recommending PrEP to this group. Regarding HCPs, the low prescription rate of PrEP may ascribe to the “Purview paradox.” 47 It means to say, there was disagreement over who should take responsibility for the prescription of PrEP; HIV specialists considered that primary care clinics should be in charge of PrEP because they had greater opportunities to access HIV-negative patients. Whereas, the primary care physicians seemed to hold the opposite opinion, they believed PrEP to be beyond their purview; HIV specialists were more experienced and inclined to work in contexts where HIV-positive patients were easier to access. This difference in perspectives and roles among HCPs may contribute to the lower prescription rates observed.
The overarching barriers affecting PrEP implementation identified in this overview were cost and knowledge, which nearly all risk populations deemed as factors in retarding uptake of PrEP. As a consequence, addressing these barriers requires appropriate strategies such as increasing insurance coverage or implementing measures to reduce the cost burden. Lack of knowledge has a direct bearing on willingness to use PrEP, and it is understood that women expressed anger because they had never heard of PrEP before. 50 To overcome this barrier, it is necessary to provide more educational opportunities to ensure that individuals have accurate and comprehensive information about PrEP. Another obvious barrier to PrEP use mentioned in most reviews was stigma; people at risk of HIV infection were worried about being treated as HIV positive when using PrEP. This stigma arises from a general lack of familiarity with PrEP, with many assuming that it is exclusively for HIV-positive individuals, and the reluctance to use PrEP among the high-risk population can be attributed to this misconception.
To a certain extent, effectiveness of PrEP depends on adherence, so it of great importance to use PrEP continually. We could conclude higher adherence to PrEP by MSM than the WWID in this umbrella review, which was probably due to the highly vulnerable and marginalized nature of WWID. In contrast to MSM, WWID were more likely to be involved in the sex trade and dependent on this work for obtaining drugs. Plenty of WWID in such rather unusual circumstances may have experienced physical and psychological violence, which can disrupt their ability to maintain consistent use of PrEP. In addition, different understandings of the definition would also result in different judgment criteria, so that the proportion of people who could take the PrEP exactly as prescribed in different studies varied. Overall, ensuring high levels of adherence to PrEP remains a critical factor in maximizing its effectiveness. It is also important to note that the PrEP field is only about a decade old, and has changed dramatically in that short period of time. We attempted to weigh several key indicators of the results of the systematic reviews and meta-analyses, but unfortunately the only data available varied widely.
For example, although two or three reviews reported on knowledge and adherence to PrEP, they surveyed different populations and had subtle differences in their geographic locations. Therefore, we were unable to use quantitative analysis to synthesize the ratings, which is a relative weakness of this study. However, we can take a qualitative synthesized description approach to evaluate studies published in different years. For example, the study by Sun et al. 38 and Peng et al. 37 both synthesized the proportion of willingness to take PrEP in the MSM population, while the year of the former was 2022 and the year of the latter was 2018. However, we preferred the results of Sun et al., 38 because the study included a larger number of original studies, had a larger sample size, and a greater proportion of higher evidence based on the results of the GRADE. Similarly, for the two reviews published in 2017 55 and 2022 64 assessing adherence, the one published in 2021 was more credible because it included RCTs with mostly high GRADE ratings that were closer to reality.
However, there are still unresolved issues in the area of PrEP. Relevant studies have shown that some vulnerable populations such as ethnic minorities among MSM are still disproportionately affected by HIV, 65 implying that this population needs more attention. And people at high risk of HIV have different preferences for different forms of PrEP delivery, 66 for example, there is growing interest in PrEP as an over-the-counter medication, because barriers to accessing PrEP can be mitigated through the availability of PrEP over-the-counter medication. 67 Therefore, more research is needed in the future to explore these multilevel approaches to promote PrEP engagement.
In perspective of the present scenario, PrEP is moderately known to potentially susceptible populations. In addition, through the data of acceptability, people expressed a strong willingness once they were informed, therefore, there is much room for knowledge dissemination. It is a pity that despite positive adherence rates, PrEP utilization remains suboptimal. The reliable evidences provided in this umbrella review demonstrating that the PrEP uptake is dependent on a large number of factors, which can be divided into patient level (lack of request for PrEP, low-risk perception), provider level (lack of training, providers' lack of time), and structural level (stigma, insurance coverage, lack of PrEP care models). As a result, addressing these barriers requires coordinated efforts by individuals, governments, and the society; only in this way can we achieve global popularization of PrEP and efficient prevention of HIV. In conclusion, while PrEP has gained recognition and acceptance among at-risk populations, there is a need for focused efforts to enhance knowledge dissemination, overcome barriers, and promote the global implementation of PrEP as an effective HIV prevention strategy.
Limitations
It must be acknowledged that there are following limitations in our research. First, on account of the insufficient data available, we are incapable to calculate estimation of common effects in each stage of HIV PrEP continuum of care across different populations based on included reviews. Consequently, direct comparisons between different groups were not feasible, which prevents us directly comparing whether there are gaps between different groups of people. Second, using AMSTAR tool for methodological quality assessment might be considered overly rigorous. That is why there is no review rated as high or moderate, which could affect the overall assessment of the included studies. Third, we only searched studies published in journals indexed in PubMed, Embase, and Cochrane, unpublished and/or gray literatures were not included, which might introduce publication bias and limit the comprehensiveness of our findings. Finally, our review may be subject to limitation of generalizability of results on account of our language restriction.
These limitations should be taken into consideration when interpreting the findings of this research, and future studies should strive to address these limitations to provide a more comprehensive understanding of the barriers and facilitators related to PrEP implementation across diverse populations.
Footnotes
Acknowledgments
The authors thank all individuals who provided help during the research.
Authors' Contributions
G.J.: Conceptualization (lead); writing—original draft (lead); writing—review and editing (equal). J.D.: Methodology (lead). H.S.: writing—review and editing (equal). H.G. and G.Y.: scanned the title and abstracts. H.Y., Z.Zhu, K.Z., X.Z., X.L., J.Z., W.X., S.W., J.H., Y.S., and P.S.: Writing—original draft (supporting). Z.Zha.: review and editing (equal). All authors have read and approved the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.