
Abstract

To the Editor:
HIV
Breast cancer incidence has not been shown to be elevated in WWH. 6,7 However, with increasing life expectancy of WWH due to ART use, breast cancer incidence may increase to similar rates seen among women without HIV. 8 In WWH, breast cancer may present earlier in life, have more multifocal lesions, and may present with a more advanced stage than in women without HIV. 9
Appropriate screening is necessary to reduce breast and ICC risk. We examined mammogram and Pap smear uptake in cis-gender women using data from the prospective HIV Outpatient Study (HOPS) cohort collected during January 2010–December 2021. Figure 1 illustrates the selection steps used to create the analysis cohorts.
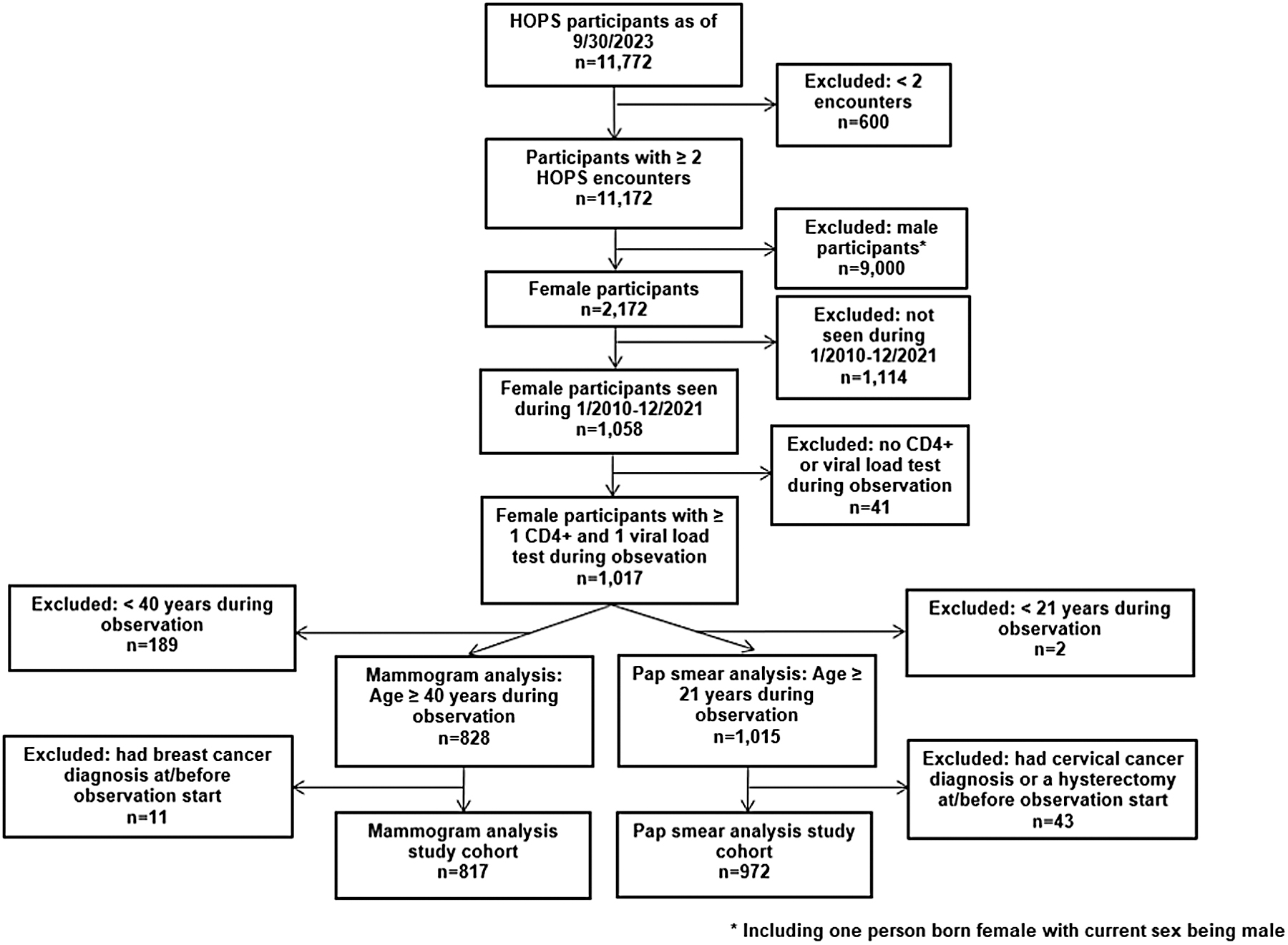
Study population selection process, HIV Outpatient Study, 2010–2021. *Including one person born female with current sex being male. HOPS, HIV Outpatient Study.
The baseline predictor variables included age in years (ages 40–49, ≥50 for the mammogram analyses and ages 21–29, 30–65, and ≥66 for the Pap smear analyses), race/ethnicity, HIV risk group ordered by transmission risk potential, insurance payor, clinic type, ART status, smoking history, body mass index (BMI), CD4+ lymphocyte cell count (CD4, cells/mm3), year of observation, first HOPS encounter year, prior AIDS diagnosis, and HIV viral load (VL).
Statistical analyses were done using SAS version 9.4 (SAS Institute, Cary, NC, USA). Likelihood ratio chi-square or Fisher exact tests were used to compare patient characteristics (binary or class variables) and Kruskal–Wallis or Wilcoxon rank-sum test were used to compare continuous variables by outcome. To examine longitudinal patterns, we performed univariate and multivariable analyses using generalized estimating equations (GEE) modeling assuming a binomial distribution: mammograms and Pap smears analyzed were limited to the first one during each calendar year of observation, with the following characteristics time-updated: age, insurance payor, BMI, ART status, CD4, and VL. Factors with p values ≤0.1 in univariate analyses were included in multivariable analyses.
The 817 eligible participants for the mammogram analysis had a median follow-up observation of 7.4 years [interquartile range (IQR): 2.9–11.7 years], the median age was 46 (IQR: 41–53 years), 166 (20.3%) were Non-Hispanic/Latina (NH/L) White women, 463 (56.7%) were NH/L Black women, 162 (19.8%) were H/L women, and 26 (3.2%) were of other race/ethnicity. Regarding HIV risk, 658 (80.5%) were heterosexual, 92 (11.3%) had used injection drugs, and 67 (8.2%) had other/unknown HIV risk. During observation, 411 (50.3%) had at least one mammogram. In multivariable GEE analyses, the following factors were associated with having a lower mammogram screening during a given observation year: being NH/L White compared to NH/L Black women [adjusted odds ratio (aOR) 0.52, 95% confidence interval (CI) 0.38–0.71], not having a BMI recorded versus a BMI <25 kg/m2 (aOR 0.16, CI 0.05–0.52), having CD4+ <200 cells/mm3 versus a CD4+ ≥500 cells/mm3 (aOR 0.57, CI 0.38–0.85), a VL of 1000–99,999 copies/mL versus a VL <200 copies/mL (aOR 0.59, CI 0.44–0.80), or first HOPS encounter year of 2011–2019 or 2020–2021 versus 2010 or earlier (aOR 0.69, CI 0.54–0.90; aOR 0.35, CI 0.14–0.91, respectively). Selected factors in the multivariable GEE analyses are shown in Fig. 2. Ten participants had a diagnosis of breast cancer during the observation period with an incidence of 175/100,000 person-years (PY) compared to 128/100,000 PY in general population. 10 Of them, six received at least one mammogram during observation before their diagnosis (median days from mammogram to breast cancer diagnosis = 136, IQR: 20–1408 days).
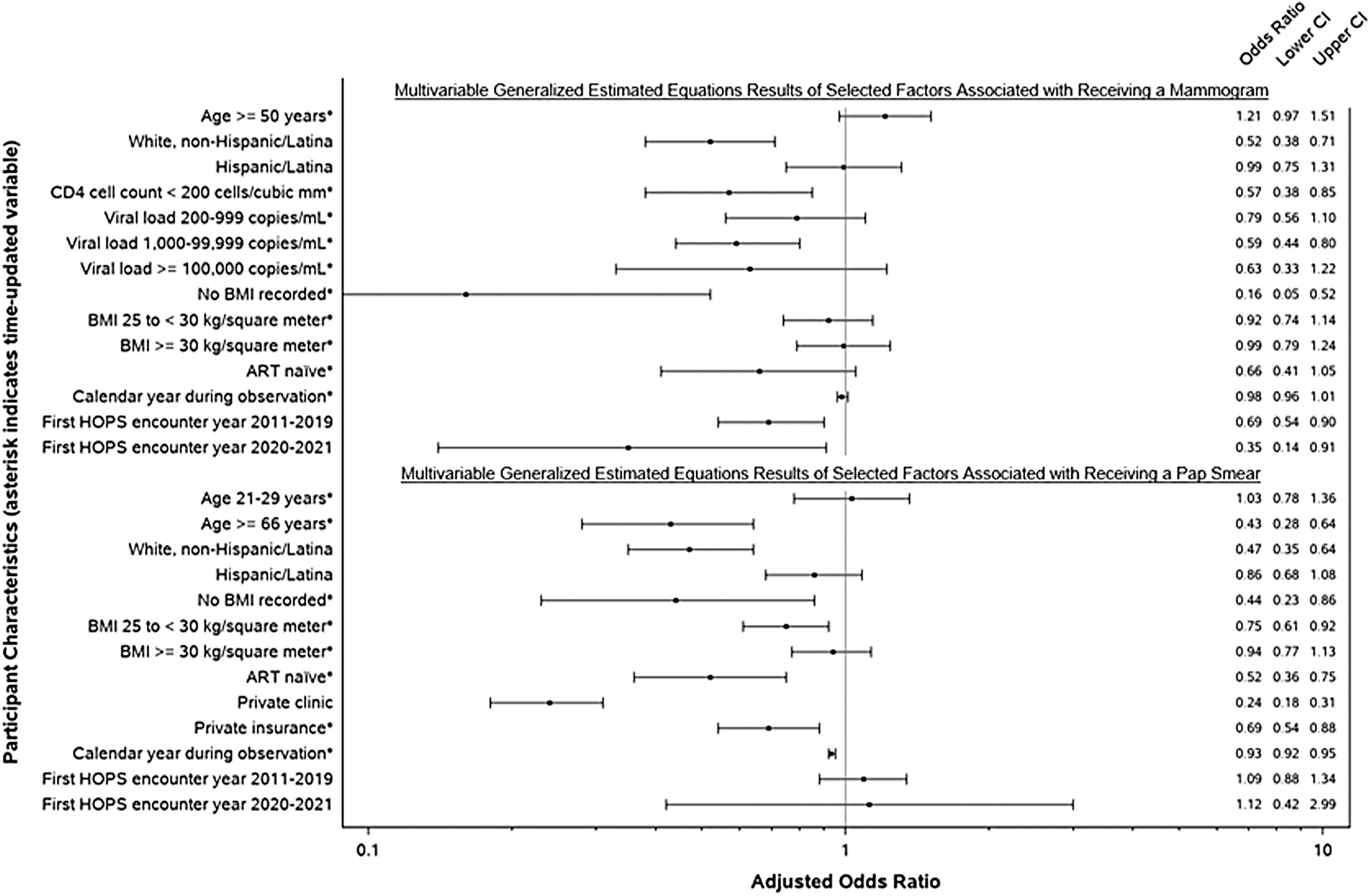
Multivariable generalized estimating equations results of selected factors associated with receiving a mammogram or pap smear, the HIV Outpatient Study, January 1, 2010–December 31, 2021, N = 817 mammogram, N = 972 pap smear. *Indicates time updated variables. Note: Factors with p values <0.1 in univariate analyses were included in the multivariable analyses. Referent groups: VL: <200 copies/mL, BMI: <25 kg/square meter, race/ethnicity: Black non-Hispanic/Latina, first encounter year: 2010 or earlier, clinic type: public, insurance: public, age in years: 40–49 for mammograms and 30–65 for pap smears. ART, antiretroviral therapy; BMI, body mass index; CI, confidence interval.
For the 972 eligible Pap smear analysis participants, the median follow-up was 7.5 years (IQR: 2.9–11.9 years), the median age was 44 (IQR: 36–51 years), 187 (19.2%) were NH/L White women, 560 (57.6%) were NH/L Black women, 186 (19.1%) were H/L women, and 39 (4.0%) were other race/ethnicity. In terms of HIV risk activity, 786 (80.9%) were heterosexual, 88 (9.0%) had used injection drugs, and 98 (10.1%) had other or unknown HIV risk. During observation, 515 (53.0%) had at least one Pap smear. In multivariable GEE analyses, the following factors were associated with lower uptake of Pap smears: ≥66 years versus referent 30–65 years (aOR 0.43, CI 0.28–0.64), NH/L White race/ethnicity versus NH/L Black race/ethnicity (aOR 0.47, CI 0.35–0.64), having private insurance versus public insurance (aOR 0.69, CI 0.54–0.88), being seen in a private clinic versus a public clinic (aOR 0.24, CI 0.18–0.31), being ART-naïve versus ART-experienced (aOR 0.52, CI 0.36–0.75), having no BMI recorded versus a BMI <25 kg/m2 (aOR 0.44, CI 0.23–0.86), and later year of observation (aOR 0.93, CI 0.92–0.95). See Fig. 2 for selected factors in the multivariable GEE analyses. There were seven participants who had an ICC diagnosis during the observation period, with an incidence of 101/100,000 PY compared to general population of 7/100,000. 11 Of them, five received at least one Pap smear during observation before the diagnosis (median days from Pap smear to ICC diagnosis = 315, IQR: 29–653 days).
Our study is one of the first large, multicenter US cohorts that examine breast cancer and ICC screening and incidence rates in a modern era of HIV care: 2010–2021. In our study, WWH who attended public-based clinics had higher odds of getting a Pap smear than those attending private clinics. We observed higher breast cancer screening rates among WWH with lower VLs and higher CD4, which may reflect characteristics of women better engaged in care and adherent to ART. However, only half (50.3%) of WWH who qualified for breast cancer screening had a mammogram during the median follow-up of over 7 years of observation. Observationally, NH/L White women received less ICC screening and mammography than NH/L Black women, which may be a function of different screening practices across participating HOPS sites. Most NH/L Black women in the HOPS receive care in Philadelphia, which performs cervical cancer screening within the Ryan White-funded clinic.
Many public clinics in the HOPS have Pap smears performed onsite, often by the same provider who addresses HIV care. Other studies have suggested that at sites with colocated primary care and gynecologic care, women are more likely to receive Pap smears. 12 Therefore, public clinic attendance may facilitate screening and possibly access to results, which would impact detection rates and opportunities to act on precancerous lesions for ICC. Our data suggest that WWH in the HOPS cohort have higher ICC rates than women in the general population, which could be related to higher frequency of Pap smear among WWH recommended by clinical guidelines, sociodemographic characteristics, immunodeficiency, or other factors, and highlights the need for routine ICC screening.
Among WWH in the HOPS, a demographically diverse, contemporary HIV cohort, with a majority of NH/L Black women, we found low breast and ICC screening rates, despite elevated cancer incidence rates. Our findings indicate missed opportunities to provide comprehensive preventive care and equitably protect health of all WWH.
Footnotes
Acknowledgments
HOPS Investigators. The HOPS Investigators include the following persons and sites: Jun Li, Kate Buchacz, Alex Ewing, HIV Research Branch, Division of HIV Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention (NCHHSTP), Centers for Disease Control and Prevention (CDC), Atlanta, GA; Cheryl Akridge, Stacey Purinton, Selom Agbobil-Nuwoaty, Kalliope Chagaris, Kimberly Carlson, Qingjiang Hou, Carl Armon, Linda Battalora, Jonathan Mahnken, Cerner Enviza an Oracle Company, Kansas City, MO; Frank J. Palella, Conor Daniel Flaherty, Cheryl Carter- Houston, Feinberg School of Medicine, Northwestern University, Chicago, IL; Cynthia Firnhaber, Barbara Widick, Rosa Franklin, Billie Thomas, Vivent Health, Denver, CO; Jessicamarie Fox, Linda Kirkman, DuPont Circle Physicians Group, Washington, DC; Jack Fuhrer, Linda Ording-Bauer, Rita Kelly, Jane Esteves, State University of New York (SUNY), Stony Brook, NY; Ellen M. Tedaldi, Ramona A. Christian, Faye Ruley, Dania Beadle, Princess Davenport, Lewis Katz School of Medicine at Temple University, Philadelphia, PA; Richard M. Novak, Andrea Wendrow, Stockton Mayer, University of Illinois at Chicago, Chicago, IL; Cynthia Mayer, Karen Maroney, Kimberly Braden, Tori Edwards, Brenda Ware, Chrissy LaPointe, St. Joseph's Hospital Comprehensive Research Institute, Tampa, FL; Theo Hodge, Benita Viswasam, Washington Health Institute, Washington, DC; Gina Simoncini, AIDS Healthcare Foundation, Philadelphia, PA.
Authors' Contributions
C.F.: Conceptualization, writing—original draft/review, validation, resources visualization, supervision. G.S.: Conceptualization, writing—original draft/review, validation, resources visualization. C.M.: Conceptualization, resources, validation, writing—review/editing. C.A.: Methodology, data curation, formal analysis, writing—original draft/review. A.E. and K.B.: Methodology, formal analysis, writing—review. E.T.: Resources, writing—review. L.B.: Conceptualization, writing/review, visualization. K.C. and K.C.: Data curation, project administration, supervision, funding acquisition. J.L.: Methodology, software, formal analysis, writing—review.
Ethics
Since its inception, the HOPS has been reviewed and approved annually by the institutional review boards of the Centers for Disease Control and Prevention (CDC; Atlanta, GA, USA), Cerner Corporation (Kansas City, MO, USA), and each HOPS site. The study protocol conforms to the guidelines of the US Department of Health and Human Services for the protection of human subjects in research. All participants provided written informed consent.
Author Disclosure Statement
Gina Simoncini is on the speaker's bureau for VIIV. There are no conflicts of interest among the remaining authors.
Funding Information
Centers for Disease Control and Prevention (contract nos. 200-2001-00133, 200-2006-18797, 200-2011-41872, 200-2015-63931 and 75D30120C08752).