
Abstract
To understand the global dual HIV infection (DI) profiles comprehensively, the databases Cochrane Library, Embase, PubMed, and Web of Science were the data sources up to March 31, 2024 (PROSPERO: CRD42023388328). Stata and R-language software were used to analyze the extracted data. Publication bias was assessed using Egger’s test. Sensitivity analysis was conducted to evaluate the stability of the combined effect values. Data from 17 eligible studies across four continents (Africa, Asia, Europe, and North America) with 1,475 subjects were used. The combined dual infection rate (DIR) was 10.47% (95% CI: 7.11%−14.38%) without a time trend (p = 0.105). The DIRs of target population groups differed significantly, with FSWs having the highest DIR (15.14%), followed by general population (12.08%), MSM (11.84%), and DUs (9.76%). The subtype profiles of 122 patients with dual infection were extracted, and the results showed that intrasubtype infections were predominant in coinfection (16/22, 72.73%) and superinfection (68/100, 68.00%) groups, with the subtype pattern B and B accounts for the largest proportion. The global dual infection rate may be underestimated, even though the data fluctuated around 10% and showed no time trend. The occurrence of DI indicated that individuals still do not acquire sufficient resistance to HIV even after primary infection, which could potentially compromise the patient’s treatment effect and lead to the emergence of new subtypes, posing a significant challenge to HIV prevention, control, and treatment, suggesting that behavioral counseling and health education for all HIV-infected individuals are still crucial during the antiviral therapy.
Introduction
Although the number of people newly infected with HIV each year has decreased since 2010, about 1.3 million people (1–1.7 million) acquired HIV in 2022. 1 Current trends predict that nearly 1.2 million people will acquire HIV by 2025, 2 far exceeding the 2025 target of 370,000 new infections. 3
The diversity of HIV subtypes significantly impacts HIV prevention, diagnosis, therapy, and vaccine development. In addition to the nine HIV-1 group M subtypes, such as A-D, F-H, J, and K, the number of HIV-1 circulating recombinant forms (CRF) has exceeded 100. 4 With the evolution and spread of HIV, the proportion of HIV-1 CRF and unique recombinant form (URF) has dramatically increased globally. Based on 383,519 publicly reported samples from 116 countries between 1995 and 2015, a study evaluated the global distribution and trends of HIV subtypes, dividing the time into four time periods (1990–1999, 2000–2004, 2005–2009, and 2010–2015). 5 Although pure subtypes such as A, B, and C consistently dominated patient subtypes (77.2%–90.7%), the proportion of CRFs and URFs increased over time. Recombinants comprised only 9.3% of all infections worldwide in 1990–1999, but this proportion increased to 19.7% in 2000–2004 and reached 22.8% of the global distribution in 2010–2015.
China has also conducted four national molecular epidemiological surveys on HIV. The proportion of B, C, and E subtypes in the initial survey from 1996 to 1998 was 91.4%. 6 The BC recombinant strains and CRF01_AE have emerged as the most common strains in the second survey, conducted in 2002–2003. 7 Following the findings of the third study conducted in 2006–2007, the CRF07_BC, CRF01_AE, and CRF08_BC have already accounted for 83.2% of the total infected population, 8 this number increased to 85.3% in the fourth survey 9 and remain high in 82.0% in 2020–2022. 10
Meanwhile, the types of CRFs are rapidly increasing. CRF157_A6C was reported as a novel CRF in 2023, 11 just two more years after CRF103_01B was reported in 2020. 12 In addition to the potential contribution of mutation and mismatch during replication, new strains due to dual HIV infections (DI) with different subtypes of strains and recombination of these strains, which gradually replace the original strains and spread to others through various routes, are the leading causes of the emergence and epidemic of novel CRFs. 4 The characteristics of novel CRFs on transmission, treatment, drug resistance, and disease progression also pose additional challenges for HIV prevention and treatment.
Dual HIV infections are defined as two or more strains of HIV infecting the same patient. 13 According to the interval between two infections and more strains, DI can be divided into coinfection (strains that infect the same patients simultaneously or before the seroconversion) and superinfection (the second strain infects the patients after seroconversion). Moreover, DI can be divided into intersubtype (multiple infection strains that belong to distinct subtypes) and intrasubtype (multiple infection strains belong to the same subtype) according to the type of infected strains. However, research on HIV dual infections is limited due to sampling procedures or detection technology constraints. The global prevalence of DIs and DI subtype pattern is unknown. Therefore, we aimed to understand the DI profiles through a meta-analysis based on the data reported from next-generation sequencing (NGS) studies and provide reference information for future timely detection and precise treatment to improve the treatment effect, as well as reduce the generation and transmission of CRFs.
Methods
Search strategy
The review protocol was registered on PROSPERO (CRD42023388328). The Cochrane Library, Embase, PubMed, and Web of Science databases were searched for eligible articles. Search terms included HIV, AIDS, Human Immunodeficiency Virus, Acquired Immune Deficiency Syndrome, coinfection, co-infection, co infections, Dual-infection, Dual infection, Superinfection, Intersubtype, and Intrasubtype. A manual article retrieval strategy was also used to retrieve and supplement the literature listed in the review. Regardless of the article type, every publication between January 1, 2010, and March 31, 2024, was searched on April 2, 2024.
Inclusion and exclusion criteria
Inclusion criteria include (1) studies published in English, conducted among people living with HIV, and published between January 1, 2010, and March 31, 2024; (2) studies targeting persons infected with two or more different HIV cluster strains; (3) reported the number of people included in the study and the detection of multiple infections; and (4) NGS was performed to identify the dual infection. Only the most recent studies that provided the complete information were included for studies that used data from the same cohort.
Exclusion criteria include (1) studies of coinfection with other non-AIDS diseases, (2) animal or cellular studies, and (3) case report, letter, or reviews.
Study selection, data extraction, and quality assessment
Endnote (version X9) software was used to manage the retrieved studies. Two researchers individually examined the literature, and the relevant data were checked and extracted based on the prespecified criteria. Disagreements were settled through debate until an agreement was reached or a third author was consulted. Information extracted included the name of the first author, year of publication, the sample source, the research type, the study population, the type of dual infection, the number of study participants, the successful amplification cases, the number of dual infection cases, and the specific subtype profiles of patients with dual infection. If the information on the number of participants with dual infection was available and the research subjects were from different areas or included distinct populations, they were extracted as multiple data points. We adjusted the literature quality assessment items following the AHRQ’s cross-sectional studies evaluation standards, considering the STROME-ID Statement and the characteristics of the HIV DI studies. A total of 11 assessment items were ultimately identified (Supplementary Data S1, p. 2).
Subgroup design
Asia, Europe, North America, and Africa were the four regions of the Sample Source variable used in this study. Income levels were classified as low-income, lower-middle income, upper-middle income, and high-income according to the World Bank Country and Lending Groups (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519). Cohort and cross-sectional studies made up the majority of study designs. The general population, men who have sex with men (MSM), female sex workers (FSWs), drug users (DUs), and others (population subgroups with only one study were combined in this group) constituted the majority of the study populations. The types of dual infections were grouped as coinfection or superinfection based on the time of dual infection and divided into intersubtype or intrasubtype by the type of dual infection virus strains.
Statistical analysis
Stata (version: 16.0) and R software (version: 4.3.3) were used for the statistical analysis. Stata was used to conduct the temporal trend test, and the Metadata package was used to evaluate the DIR (Arcsine transformation) and cumulative meta outcomes. The heterogeneity test employed the Q test and I 2 test. A p value ≤ 0.05 or I 2 value ≥ 25% indicated study heterogeneity. The combined effect value was determined using the random-effects model when p ≤ 0.05 or I 2 ≥ 50%; otherwise, the fixed-effects model was used. Subgroup analysis and meta-regression analysis were also conducted. Egger’s test was used to assess publication bias. A p value ≥0.05 indicated no substantial publication bias; the clipping and complement approach were employed to rectify publication bias where necessary.
Results
Study selection
Figure 1 14 shows the literature screening process. A total of 6,023 studies were retrieved from the database search, and 2,858 were screened after deduplication. With 2,654 papers eliminated by unrelated titles and abstracts, the full texts of the remaining 204 articles were screened for eligibility, of which 187 were excluded (124 studies did not relate to the dual infection rate research; 23 reported the dual infection rate identified by non-NGS methods; 19 are the comments, reviews, and letters; ten studies reported the new CRF information; five used the same data with previously published research; three conducted in vitro; and three did not provide accurate data). In addition, seven studies identified through searching the reference lists of related studies were also excluded due to ineligibility after full-text screening (three used non-NGS methods, two had no connection to the dual infection, one was a systematic review, and the other was a case report study). Finally, 17 studies were included. 13,15 –30
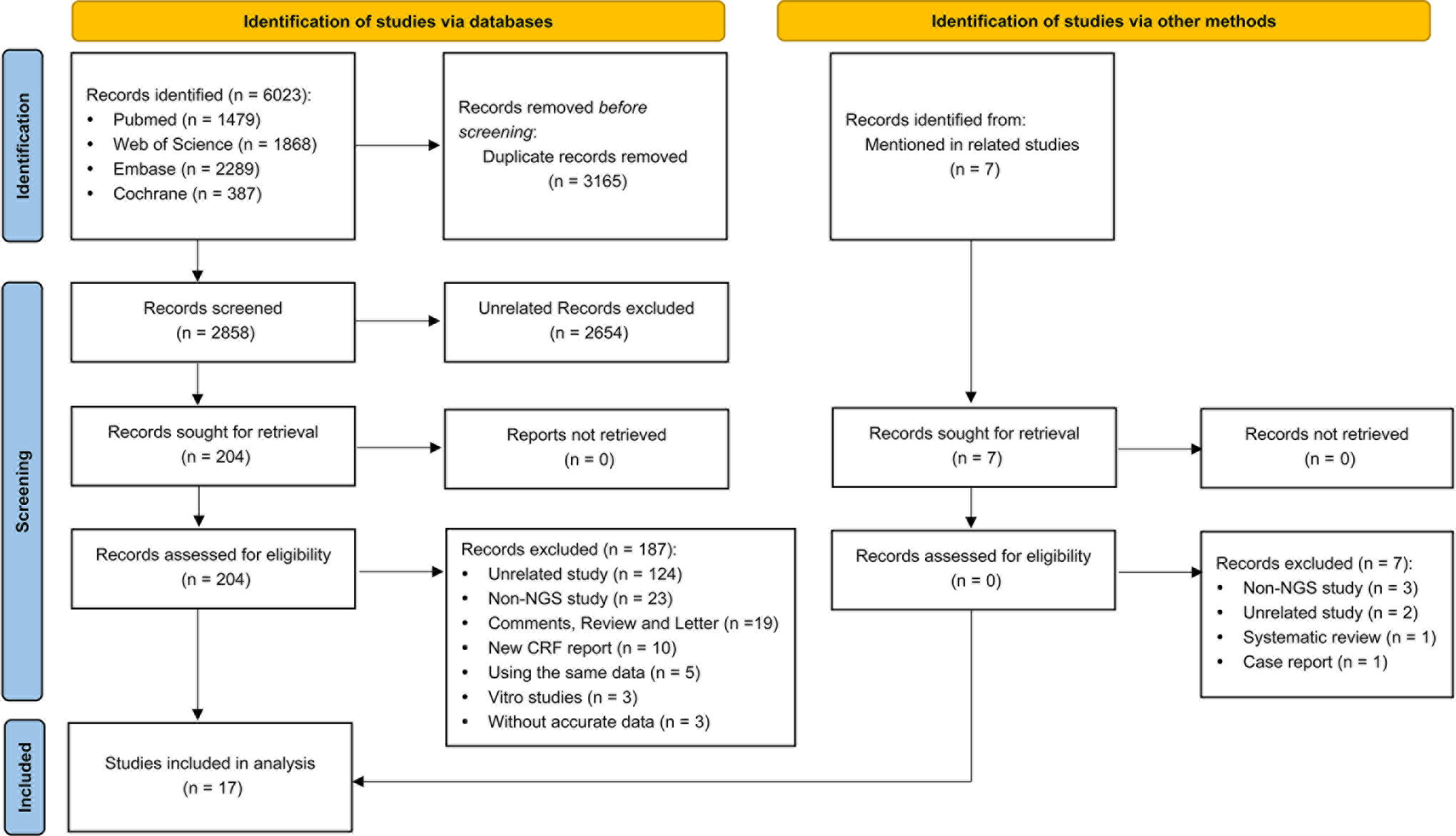
PRISMA 2020 study selection flow diagram for the meta-analysis of HIV dual infection.
Study characteristics
Table 1 presents the characteristics of the 17 studies that were included, all of which used NGS to verify the dual infection and were assessed to be of high quality (quality assessment score ≥8). There were 1,475 participants comprising members of the general population, MSM, FSWs, DUs, TGM, and HIV-infected pregnant women from four continents (Africa, Asia, Europe, and North America). The detailed information of included studies is provided in Supplementary Data S2.
Characteristics of 17 Studies for the Dual Infection of HIV
DUs, Drug Users; MSM, Men Who Have Sex with Men; FSWs, Female Sex Workers; TGW, Transgender Women.
Meta-analysis and trend analysis of dual infection rate
DIR across the 17 data points ranged from 0.00% to 28.13%. Following the meta-analysis, the overall DIR of several HIV strains was 10.47% (95% CI: 7.11%−14.38%) (Fig. 2A). A cumulative meta-analysis per the time of publication was conducted (Fig. 2B). The findings showed that DIR fluctuated around 10% and showed no increasing or decreasing trend (Coef = 0.00103, p = 0.105).
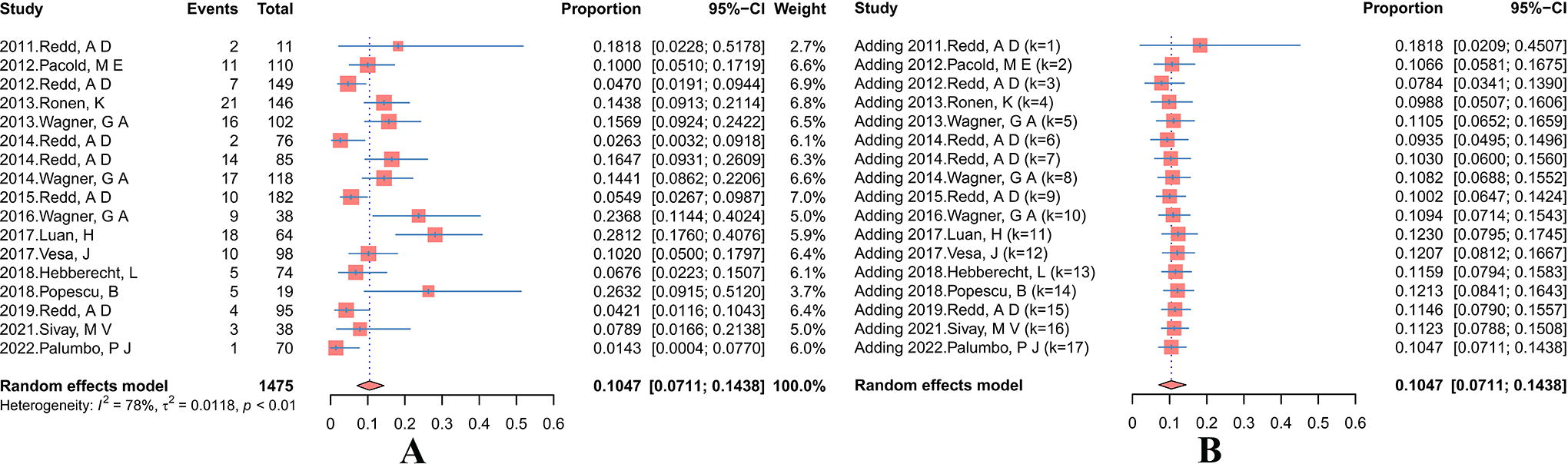
Forest plots of meta
Subgroup analysis and meta regression
Study design, target population, sample source, and income level were considered variables in subgroup analysis and meta-regression (Table 2). Since patients from Indonesia (Asia) and Ukraine (Europe) were included in a single study, 15 which also documented the dual infection rates for study subjects from each location, this study was extracted as two data points, yielding a total of 18 data points for sample source and income level. Our results showed differences between the study design, and target population groups (p < 0.05). DIR varied among the different population groups, with the highest rate found among FSWs (15.14%), followed by general population (12.08%), MSM (11.84%), and DUs (9.76%).
Subgroup and Meta-Regression Analysis for the Dual Infection of HIV
p < 0.05.
DI, Dual HIV Infection; CI, Confidence Interval.
Dual infection rate of different types
Groups divided by the dual infection time interval or the infected virulent strains in patients were not statistically different (Table 3) (Fig. 3). Superinfection (7.54%) had a slightly lower rate than coinfection (8.01%) among DI-type time intervals, and intersubtype (6.95%) had a slightly higher rate than intrasubtype (6.52%) among DI-type virus strains.
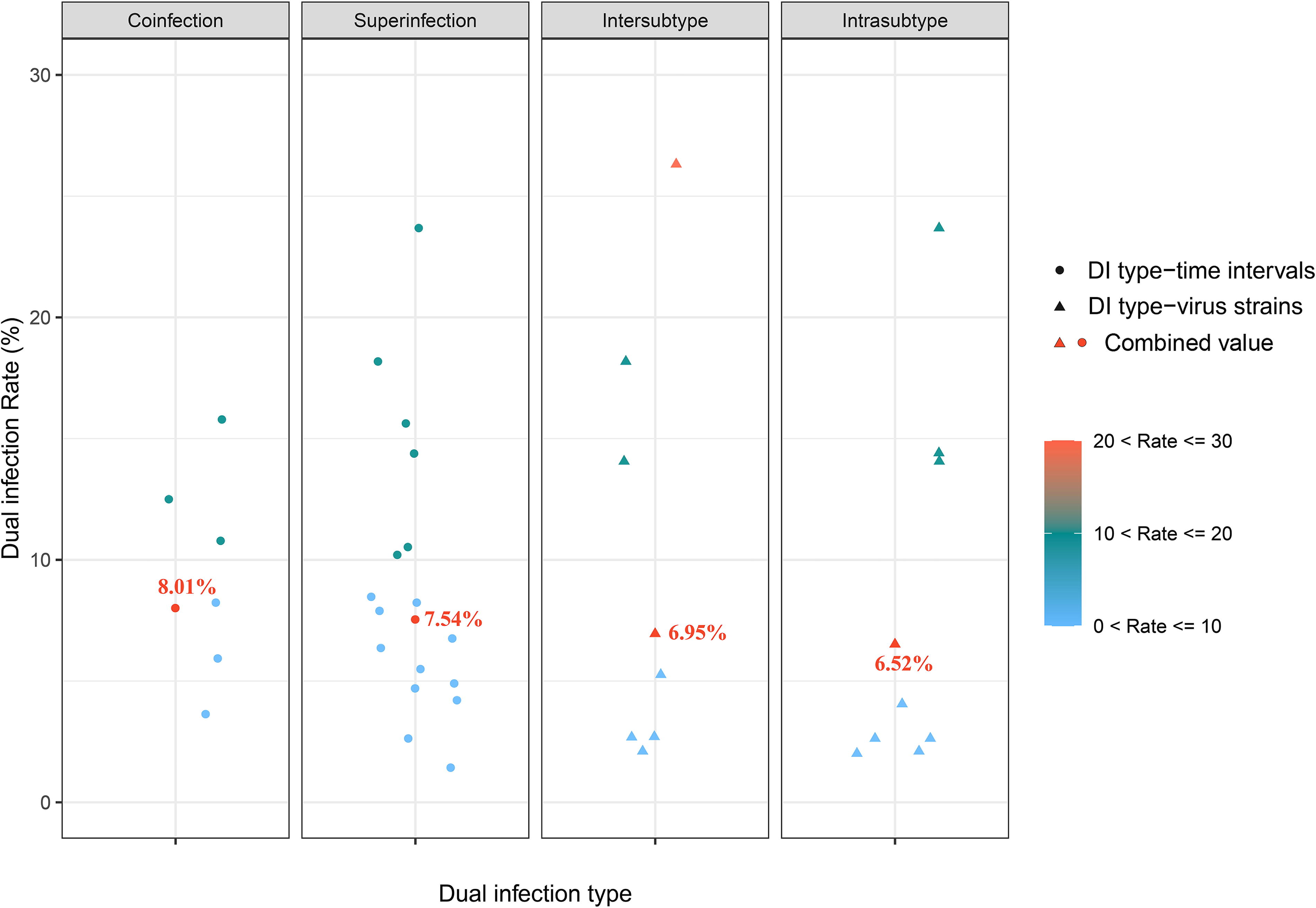
Scatterplot of the DIR of different time intervals and virus strain types.
Subgroup Analysis for Different Dual Infection Types of HIV
Publication bias test and sensitivity analysis
Egger’s test showed no evidence of publication bias (p = 0.2331). Sensitivity analysis was used to eliminate each study independently, which showed that overall DIR did not vary substantially, and the outcomes remained stable (Supplementary Data S1, p. 9–10).
Subtype patterns of 122 patients with dual infection
Subtype profiles of 78.71% (122/155) of patients with dual infection were extracted from 15 studies (88.24%), as detailed in Supplementary Data S2, with 22 and 100 patients identified as coinfection and superinfection, respectively. Within the coinfection group (Fig. 4), intrasubtype infections were predominant (16/22, 72.73%), including B + B (11/16, 68.75%) and 01_AE + 01_AE (5/16, 31.25%). Intersubtype infections comprised the remainder (6/22, 27.27%), including 01_AE + 07_BC and F + 14_BG, each accounting for three cases. In patients with superinfection (Fig. 5), intrasubtype infections were also predominant (68/100, 68.00%), including B and B (41/68, 60.29%), A and A (13/68, 19.12%), D and D (7/68, 10.29%), 01_AE and 01_AE (4/68, 5.88%), as well as C and C (3/68, 4.41%). The remaining superinfections were intersubtype infections (32/100, 32.00%), with D and A (7/32, 21.88%) and 01_AE and 07_BC (4/32, 12.50%) accounting for more than two cases.
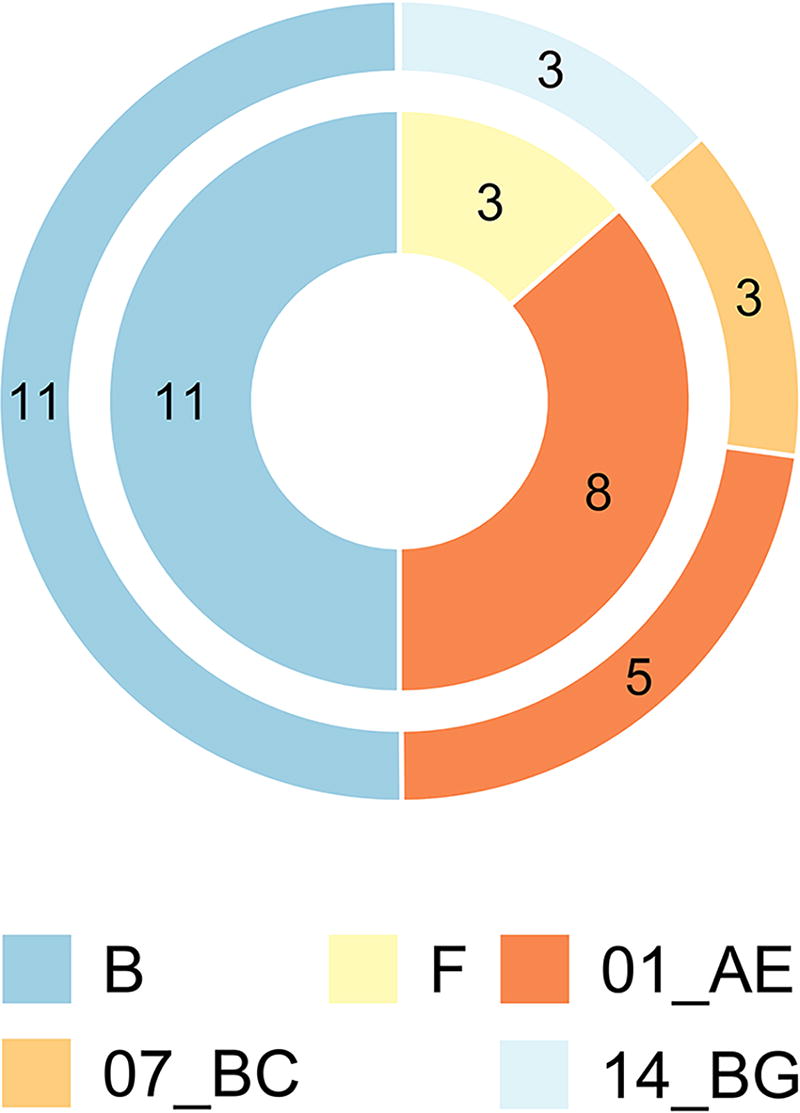
Bilayer pie chart of subtype patterns of 22 coinfection patients. PS: The inner circle represents subtype 1, and the outer circle represents subtype 2. Subtype 1 and subtype 2 coexist in the patient’s body without order.

Sanke diagram of subtype patterns of 100 superinfection patients. PS: Column 1 represents the HIV subtype when the patient was infected, and column 2 represents the HIV subtype in the patient’s body after superinfection occurs. Even if the HIV strain’s subtype before and after superinfection is the same, they belong to different clusters of the same subtype.
The DI types based on the time intervals and the virus strains show differences among different populations (Table 4). This study only found superinfection cases in FSWs and the general population groups, with superinfection being predominant in MSM (70.77%), while confection and superinfection were reported equally in DUs. Among MSM and the general population groups, intrasubtype infection was the main DI pattern, accounting for 80.00% and 81.25%, respectively. In FSWs, intrasubtype infection was slightly higher than intersubtype infection (53.57% vs. 46.43%). However, intersubtype infection was predominant in DUs (83.33%). The HIV subtypes were A, F, and 14_BG in DUs and A, C, and D in FSWs. In MSM, although the intrasubtype of B subtype is predominant (67.69%), there are also reports of intrasubtype and intersubtype infection between B, G, A, D, 01_AE, 07_BC, 12_BF, and 14_BG (Supplementary Data S2).
DI Types between Different DI Populations
The value of Fisher’s exact test. [5 cells (50.0%) have expected count less than 5].
The value of Fisher’s exact test. [4 cells (40.0%) have expected count less than 5].
p < 0.05.
DUs, Drug Users; FSWs, Female Sex Workers; MSM, Men Who Have Sex with Men.
Discussion
Findings from this study showed that the global HIV DIR based on the NGS data is 10.47% and DIR fluctuates around 10% and does not exhibit an upward or decreasing trend. Even after two more decades, studies on multiple infections are still relatively few due to detection techniques and the challenge of gathering samples for dual infections since the first incidence of multiple infections was reported. 31 Early research utilized multi-region hybridization assay (MHA), heteroduplex mobility assay (HMA), subtype-specific PCR, and bulk PCR + selective cloning, whereas recent studies employed single genome sequencing (SGS) and NGS to identify dual infection. 32 DI for HIV-1 and HIV-2 is detected by several techniques such as rapid test kit + SD Bioline HIV 1/2 3.0, first response HIV card 1–2.0, and others. 33 –35 However, the early techniques had issues, including limited sensitivity, low throughput, and the need for extra cloning for confirmation. Although SGS is a more sensitive test, it is also more costly and involves more workload. Therefore, despite the difficulties of NGS in fragment assembly and data analysis, the benefits (such as the high sensitivity, high throughput, and multiple regions sequence) still provide researchers a greater chance of identifying DI. Some cohort studies have noted that some patients had dual infections (coinfection) at the time of cohort inclusion, but only one strain could be found in this group of patients after one or two years of untreated follow-up, even with NGS. 13 The ideal situation is for a specific strain’s viral load to drop naturally below the detection threshold. However, the more concerning possibility is that the multiple strains of the initial infection are recombining in the patients and progressively displacing the original strain, complicating the HIV epidemic with the generation of new recombinant strains. Even if DI was not detected in some studies, it does not mean that DI does not exist; instead, it may simply be that the samples were not collected at the appropriate time (i.e., the viral load of a strain was below the detection line, or recombination had already occurred in the patients). In addition, only one-third of the studies 22,23,26 –29 included in this review included more than 100 subjects which suggests that the actual profiles of DI may be more severe than we realize. Therefore, further studies with more samples are needed to better understand the prevalence of dual infection and provide information for further measures and reducing the generation of novel recombinant forms.
It is worth noting that DIR in North America was numerically higher than in Africa (13.35% vs. 8.36%). However, the reported data showed that 76% of patients living with HIV (PLWH) in North America received ART, compared to just 51% of the sample from the African region, which is comprised mostly of individuals from Uganda and Kenya (East Africa). 1 Despite of having a high ART rate, North America has a higher DIR, which could be related to regional variations in patient composition and behavioral characteristics. In contrast to North America, where data showed that MSM accounted for 64% of new infections, 2 77% of new HIV infections reported were women and girls in Africa in 2022. 1 Meanwhile, among the five North American studies included in this study, only one study targeted the general population, 21 with the other four were MSM, 20,23,26,29 suggesting that even with higher rates of ART uptake, high-risk sexual behaviors among MSM (such as multiple partners, 20 unprotected anal sex, poor adherence, and high drug resistance 36 ) may contribute to higher DIR in North America. This regional variation in DI may be due to non-policy-related factors, indicating that prevention and treatment strategies based on local patient composition and behavioral characteristics are also required, in addition to improved treatment outcomes to reduce the incidence of DI and the generation of novel CRFs.
Key populations such as drug users, sex workers, and MSM represent less than 5% of the global population. However, due to their greater likelihood of being infected (drug users have a 35-fold higher risk of HIV infection compared to nonusers, FSWs have a 30-fold higher risk than adult females in the general population, and MSM are 28 times more likely to be infected than adult males in the general population), these population and their sexual partners accounted for more than 70% of all newly reported HIV infections in 2021. 2 In addition, our findings showed that the combined DIR surpassed 5%, regardless of the patient population. This suggests that behavioral counseling and health education for HIV-positive patients should also be strengthened in addition to previous HIV prevention strategies for high-risk populations, emphasizing the likelihood of DI and its potential impact on ART treatment to improve both the efficiency of ART and the quality of patients’ life.
This study extracted subtype profiles from 122 DI individuals, with coinfection only accounting for 18.0%. However, the combined rates were slightly higher for coinfection than superinfection; this could be attributed to fewer studies on coinfection and the small number of included subjects. In contrast, superinfection-related studies were more and involved multiple populations. Many patients start ART shortly after receiving an HIV diagnosis because most nations are currently implementing aggressive treatment strategies for newly diagnosed HIV patients. Therefore, assessing coinfection may be hindered by the short time from diagnosis to ART initiation, which could explain the low number of relevant reports. Previous studies reported both HIV primary infection and superinfection profiles during the follow-up cohort among HIV-negative participants found that the incidence of HIV superinfection was not significantly lower than the primary infection rate, 15 indicating that HIV-infected individuals did not possess sufficient resistance to dual infection by other HIV strains. The latest research showed that about 20% of individuals remain experience viral breakthrough episodes after viral suppression, 37 studies also indicate that patients who maintain good ART effectiveness experience resistance to multiple drugs after being superinfected with drug-resistant strains, 38 leading to a rapid increase in viral load, 15 emphasizing that PLWH should still be cautioned to adopt HIV prevention behaviors, adhere to ART, and avoid high-risk sexual behavior to reduce the transmission and recombination risks of drug-resistant strains.
The extracted data show that intrasubtype is the most common subtype pattern in patients with coinfection or superinfection, including B and B, A and A, C and C, and 01_AE and 01_AE. However, it is worth noting that all new CRFs were formed by recombination between strains of two different subtypes. In recent years, the number of newly reported CRFs has been increasing, 4 consistent with our finding of a higher intersubtype rate than intrasubtype, indicates that the reporting of new CRFs is not only related to the improving detection techniques but also to the more frequent recombination between subtypes. Even if intersubtype recombination does not lead to the formation of new CRFs, research has shown that dual infection, including both intrasubtype and intersubtype, can increase the genetic diversity of HIV, affecting the estimation of HIV infection time and incidence rate based on HIV genetic diversity, 39 and leading to higher viral load, it also accelerates the loss of CD4+ T cells and disease progression. 40 Considering that second-generation CRFs such as 01_AE, 07_BC, and 08_BC replaced the original pure subtypes as the main circulating strains in China quickly, 10 monitoring the occurrence of dual infections in HIV/AIDS patients not only provides reference information for personalized and precise treatment but also helps to prevent or timely identify the emergence of new third-generation recombinant strains with various advantages of parental subtypes, assisting in HIV prevention and control.
This study has certain limitations. First, the included studies were highly heterogeneous. Although the subgroup and meta-regression analysis revealed that variations in target populations contributed to the heterogeneity, this only partially explained it. Second, we included samples from four continents (East Africa, Asia, Europe, and North America) since we only included studies that utilized NGS to identify DI. There were no samples from South America, despite the sporadic reports of research there (from Brazil and Argentina), 41,42 which were excluded since they used techniques like the subtype-specific PCR with lower throughput. The absence of such a region might have impacted our results, so more research should be conducted and included to offer additional information in the future. Third, the effectiveness of subgroup and meta-regression analysis may be constrained because some subgroups had fewer references. Fourth, this study found that most of the patients extracted were intrasubtype infections, indicating that some intersubtype cases have yet to be identified and reported considering the rapid increase of CRFs, which means that the results obtained in this study may underestimate the DI profiles.
This study found that dual HIV infection is not a rare phenomenon; the DIR remains stable at around 10% globally but with the possibility of being underestimated. Regardless of the sample sources, income levels, population types, and dual infection types, the combined DIRs were higher than 5%, indicating that HIV-positive individuals may be infected by another HIV strain even under ART, behavioral counseling and health education for HIV-infected individuals are also essential to improve the effectiveness of ART and lower the risks of dual HIV infection and recombination, as well as control the transmission of drug-resistant strains.
Footnotes
Acknowledgments
The authors want to express our sincere appreciation to Gifty Marley for her valuable help on the spell and grammar check. We also express our heartfelt gratitude to all the researchers and study individuals who have conducted and participated in the included studies.
Data Availability Statement
The data used in this study are provided in Supplementary Data S1 and Supplementary Data S2.
Authors’ Contributions
Conceptualization, DF.Y., F.Z., B.W., and B.S.; methodology, DF.Y. and F.Z.; software, DF.Y., F.Z., SS.L., YY.L., and HX.Y.; validation, B.W., B.S., and LF.L.; formal analysis, DF.Y., F.Z., SS.L., and YY.L.; resources, DF.Y., F.Z., SS.L., HX.Y., LF.L., B.W., and B.S.; data curation, D.Y., F.Z., SS.L., and YY.L.; writing—original draft preparation, DF.Y., F.Z., and SS.L.; writing—review and editing, B.W., B.S., LF.L., and HX.Y.; visualization, DF.Y., F.Z., SS.L., and YY.L.; supervision, B.W. and B.S.; project administration, B.W., B.S. and LF.L.; funding acquisition, B.W., B.S., and LF.L. All authors had full access to all data in the study and had final responsibility to submit for publication. All authors read and approved the final version of the article.
Author Disclosure Statement
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This study is financially supported by the National Key R&D Program of China (
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.