
Abstract
As HIV diagnoses continue to decrease and rates of viral suppression increase in the United States, key populations of underserved individuals represent a disproportionate share of those left undiagnosed, unengaged in care, and not virally suppressed. In 2021, the Health Resources and Services Administration’s HIV/AIDS Bureau funded 20 HIV care organizations across the United States to implement seven innovative evidence-based interventions to engage individuals in the following four focus areas: LGBTQ+ youth, people with substance-use disorder, individuals with incarceration experience, and those for whom telehealth may reduce barriers to care. This article explores themes of implementer experiences common across interventions serving the four focus areas. Data sources include key informant interviews (n = 94) with members of the implementation teams, observation, and document review. Thematic analytic methods were first inductive, identifying semantic themes from observation and document review, then deductive, selecting coded interview data for analysis of latent themes present and salient across focus areas. We identified three main themes as follows: (1) challenging by design, (2) enhanced client-centered care, and (3) leveraging relationships. We present these themes as distinct concepts and discuss how they operate in relation to one another using the Exploration, Preparation, Implementation, Sustainment framework. Teams implementing interventions to engage people with HIV who remain out of care may benefit from adopting the following: an enhanced client-centered orientation with a focus on understanding the context of clients’ lives; a high level of organizational and programmatic flexibility; an individualized, trauma-informed approach to enrollment and intervention delivery; and thoughtfully cultivated relationships among implementers, clients, and organizational partners.
Introduction
In the United States, biomedical advances and innovative behavioral health interventions have redefined the landscape of HIV treatment and prevention. 1 –3 At the population level, key indicators of epidemic control have markedly improved: incidence of new HIV diagnoses has decreased as rates of viral suppression have increased. 4 –7 While these trends drive progress toward closing critical HIV care continuum gaps, there remains a durable percentage of people with HIV who have not been successfully engaged or retained in care and/or whose HIV viral loads have not been effectively suppressed. The most recent HIV Surveillance Report published by the US Center for Disease Control and Prevention shows that by the end of 2022, only 65% of people diagnosed with HIV were virally suppressed. 8 At the same time, the National HIV/AIDS Strategy for 2022–2025 sets targets for ending the HIV epidemic in the United States by 2030, aiming to increase rates of viral suppression to 95%. 7 To close this gap, the needs of those not yet successfully engaged in care must be considered carefully. 9
Some key populations of people with HIV are disproportionately represented among unengaged groups, shouldering a persistent burden of health disparities, including differential rates in HIV diagnosis, linkage to and retention in care, and viral suppression. 10,11 People with substance-use disorder (SUD), LGBTQ+ youth, and people with incarceration experience are among the key populations affected by these disparities most acutely. 12 –20 To address the multi-faceted barriers to care for individuals in these groups, innovative strategies must be explored and implemented.
The HIV/AIDS Bureau (HAB) of the US Health Resources and Services Administration (HRSA) launched the four-year Using Innovative Intervention Strategies to Improve Health Outcomes among People with HIV (2iS) Initiative in 2021. The three high-priority populations listed above (LGBTQ+ youth, people with SUD, and individuals with incarceration experience) comprised three of the four focus areas of this initiative. 21 The fourth focus area, telehealth, is a method by which to deliver interventions to priority populations. Evidence suggests that expanding access to telehealth may lower barriers to HIV care and treatment, addressing issues related to transportation and scheduling, and client concerns about privacy and encountering HIV-related stigma in clinical settings. 22 –24 However, members of priority populations often face additional barriers to utilizing telehealth services, such as a lack of digital devices, unreliable technology infrastructure (such as cellular or broadband connectivity), and difficulty finding private time or space to engage in telehealth visits, among others. 19,25 Addressing inequities in access to telehealth among priority populations will help maximize the benefits of telehealth and improve outcomes along the HIV care continuum. 20
The 2iS initiative funds the rapid implementation of seven emerging evidence-based interventions within those focus areas (Table 1), 26 –35 by teams at 20 Ryan White HIV/AIDS Program (RWHAP) sites, operating across 15 states in a variety of settings. The Fenway Institute, in partnership with AIDS United, is funded to serve as the initiative’s Coordinating Center and Technical Assistance, while the University of California, San Francisco (UCSF) Center for AIDS Prevention Studies serves as the Evaluation Center (EC).
2iS Focus Areas, Interventions, and Participation Eligibility Criteria a
Description of the seven interventions being implemented in the 2iS initiative and participant eligibility criteria for each, presented by focus area and intervention.
Eligibility criteria in this table are the minimum eligibility criteria participating 2iS sites are required to follow. 2iS participating sites may define and follow additional criteria with consultation and approval from the 2iS Coordinating Center and Evaluation Center.
Sites may provide participants with technology (i.e., phones, data plans) to fulfill intervention-specific criteria.
2iS site implementing Max Clinic work with the 2iS Coordinating Center to determine how to assess and identify substance-use involvement.
The evaluation of 2iS, led by the EC, began at the start of the initiative and is composed of quantitative, qualitative, and mixed-methods data collection and analyses. In this article, we report on qualitative baseline findings in response to the following evaluation question: What organizational inner and outer context factors shaped the implementation of interventions?
The goal of the analysis was to identify common themes across the four focus areas. Variations in the inner and outer context factors within and across interventions represent rich areas for study and will be explored in other analyses.
Methods
The qualitative team comprised four analysts (A.T.B., K.A.K., A.M., and L.M.), and the 20 implementation sites were divided up among them relative to the analysts’ percentage effort on the grant. Each analyst was responsible for collecting data for each of the assigned sites.
We used the Exploration, Preparation, Implementation, Sustainment (EPIS) framework 36,37 at each stage of data collection and analysis. The EPIS framework defines four differentiated phases (Exploration, Preparation, Implementation, and Sustainment) over the full arc of implementation of an intervention or innovation. For each of these phases, the framework offers the following four broad constructs, or contextual zones, for consideration: outer context, inner context, bridging factors, and innovation factors. Each of these constructs, in turn, contains a menu of factors for consideration. The baseline qualitative analysis focused on the Implementation phase, and Table 2 provides descriptions and factors of interest related to each construct in that phase.
Descriptions and Factors of Interest—Implementation Phase of Exploration, Preparation, Implementation, Sustainment (EPIS) Framework
The table is depicting the main constructs of the Implementation phase of the EPIS framework, with descriptions of each construct and a list of factors within each construct that were of particular interest in the context of this evaluation.
Construct descriptions from www.EPISframework.com.
Data collection
Qualitative data for 2iS were collected from three sources: (1) document review, (2) observation, and (3) key informant interviews.
Document review consisted of initial and periodic review of secondary documents collected by the EC such as grant proposals, monitoring call worksheets, site visit reports, and slide decks from site presentations. The purpose of document review was to track and contextualize the sites’ implementation progress over time both before and after baseline key informant interviews.
Observational data collection occurred primarily across four settings: in-person at biannual learning sessions and virtually during monthly site monitoring calls, quarterly cohort calls, and biannual organizational assessments. Qualitative analysts attended learning sessions and each of the monitoring, cohort, and organizational assessment virtual meetings with their assigned sites and took detailed field notes.
Key informant interviews (KIIs) served as the cornerstone of the qualitative methods. Baseline KIIs began on a rolling basis, within 6 months of site launch, and, whenever possible, once a site had five clients enrolled and exposed to the intervention. Each site launched at a different time, pending completion of a series of prelaunch requirements, with most launching between December 2022 and February 2023. We conducted 102 baseline interviews across 20 sites from late April 2023 through early September 2023.
The baseline data collection period for both document review and observational data began at the start of the initiative in June 2022 and closed at the conclusion of baseline interviews in September 2023.
The baseline semi-structured interview guide was developed by the qualitative team, designed to address broad constructs and factors corresponding to the EPIS framework, including inner and outer context factors such as staffing, resources, organizational culture, leadership, and champions within and outside of the organization. The interview guide focused on early implementation experiences and was piloted via two mock interviews and refined based on analyst experience and feedback before use in the field.
Key informants were selected in collaboration with the EC and site champions from each site’s 2iS team leadership and operational staff. Participation in KIIs was voluntary, and each participant was offered a $50 gift card upon completion of the interview as a token of appreciation for their time. Participants were free to decline the honorarium if their employer had policies that precluded receipt of an incentive for a research interview conducted in connection with the participant’s professional role at the organization.
Interviews were conducted in person at the implementing sites or via videoconference, depending on the number of individuals to be interviewed at a site and their availability to meet in person. Interviews lasted approximately one hour, were recorded, and then securely transcribed by a professional third-party transcription service. Transcripts were deidentified, and participants were given a unique anonymous ID number.
Data analysis
Of the 102 interviews conducted, 94 transcripts were included in the analysis. Those excluded did not contain information directly related to the intervention implementation. Following the tenets of thematic analysis, 38 the qualitative team developed a codebook inclusive of a priori codes, EPIS constructs and factors of interest, and topic categories denoted in the interview guide.
Transcripts were entered into Dedoose, 39 and the coding scheme was tested and refined via an iterative group process and then broadly applied to all transcripts from November 2023 through February 2024. During this coding process, the analytic team met biweekly to discuss codebook use, repeating themes, and how baseline interview data were concordant with, or divergent from, other interviews within the same site, intervention, and focus area, as well as other data sources. While secondary coding for all 94 interviews was not feasible, we did conduct spot-check secondary coding, in which select coded transcripts were coded by a second analyst and code use alignment was discussed. The interview guide and codebook are available upon reasonable request.
To identify common themes across the four focus areas of the initiative, we first used an inductive and then a deductive analysis. The goal of the inductive analysis was to identify cross-cutting themes that were not just present but also salient across focus areas, 40 even if they were not equally represented across all interventions or sites. Through ongoing team discussion, we identified semantic themes from baseline interview field notes, notes from observational data, and document review (particularly monitoring call forms and slides from site presentations). Semantic themes included but were not limited to the following: treating the whole patient, tailoring, the ethos of not giving up, reframing the locus of care responsibility, and Maslow’s hierarchy of needs. Semantic themes were collapsed and broadened to salient latent themes, which initiated the deductive analysis. We selected codes that aligned with latent themes (patient needs, enrollment), generated code reports, and then summarized first by code and then by focus area. As a content audit, we then generated code reports for three additional codes (partnerships, definitions of success, and inner/outer context) based on the cross-cutting themes we identified from the first code summarization and reviewed the code reports to ensure that the intended scope of perspectives had been captured.
Ethics statement
The study protocol was reviewed and approved by the UCSF Institutional Review Board (IRB [22-36308]).
Results
Across four focus areas, seven interventions, and 20 implementation sites, we interviewed 94 informants, whom we categorized according to role and service environment (Table 3).
Participant Role and Service Environment, by Focus Area
Description of study participants, including role category and service environment of the site from which they operate, presented by focus area.
A site that identified itself using more than one main descriptor (e.g., community-based service organization and hospital- or university-based clinic).
We identified three overlapping and mutually informing themes that applied across focus areas. These themes are presented as distinct concepts with supporting data excerpts below, then discussed in relation to one another using the EPIS framework.
I. Challenging by design: “This work is meant to be hard.”
In baseline interviews, informants were asked to reflect on challenges they experienced in the early implementation periods. In their responses, many differentiated between what they viewed as implementation challenges to be overcome and the core challenge inherent to the initiative. As implementers grappled with the realities of engaging a client population that their standard practices had failed to engage, one of the most common insights, reflected in various ways, was an acknowledgment that, as one participant put it, “this work is meant to be hard. If these patients were easy, they wouldn’t have been eligible [for the intervention]” (Leadership, combination setting, Telehealth).
Despite broad acknowledgment of this core challenge, implementers talked about it in different ways. Some gave examples of potential participants who were not stable enough to even discuss participation or who stated directly that they did not wish to be connected to treatment and did not want to be contacted again. Several informants referred to an upper limit of needs and expressed doubt that these interventions could meet needs beyond that limit:
The place that people have to be in to qualify, at least based on how our population is here, like, their mental state is usually so bad. If they’re not able to come to their appointments, they’re not taking their meds, and they’re getting high all the time – and because a lot of it is meth use, they’re experiencing psychosis and paranoia and all sorts of things secondary to meth, an intervention that’s 12 weeks and offers five behavioral sessions cannot meet those needs.
—(Project management, hospital-based clinic, Substance Use)
Most reflections on the complex needs associated with the initiative’s goal embraced the difficulty. Many informants allowed it to regulate their expectations of how many participants they would be able to engage and how successfully those participants would be retained. One informant reframed the challenge as a reminder of their “why,” or their mission:
A challenge, by design, is who this intervention is working with—the folks that are the least engaged in all systems. … And I keep reminding myself that that’s the work, that’s the whole point of this.
—(Data management, community-based service organization, Telehealth)
Implementers across focus areas further reported that for many of their eligible clients, engagement in care was often not only not entirely about HIV, it was often not even primarily about HIV. Instead, implementers reflected on unmet foundational needs underlying patient disengagement from care, stressing how often the majority of addressing someone’s HIV meant first addressing their hunger, housing, substance use, mental health, and various co-occurring crises that threatened their immediate survival. Informants referred to this in interviews as “basic needs,” “Maslow,” and “social determinants of health.” To effectively serve individuals impacted by economic inequalities and structural racism required strenuous effort.
One participant described their site’s intervention as watering a seed as it grows and caring for a client’s foundational needs as clearing away weeds:
It’s like planting a seed. You open the ground up, you plant a seed. Right? Each time they come in for the 12 weeks, we get to water them. … [But] you got weeds that grow around a plant that’s trying to grow. So you got to … make the way clear.
—(Case management, hospital-based clinic, Substance Use)
II. Enhanced client-centered care: “Outreach versus reaching out”
While the concept of client-centered care is not new, our informants painted a picture of a shift in orientation and ethos that extends beyond the conventional “client-centered” approach and described an elevated praxis that delivers it.
Orientation and ethos
Implementers described a form of client-centered care that reflects a fundamental reorientation of care delivery, a reframing of the approach from How can we get you in alignment with this program? to How can this program be in alignment with you? Not all of the sites across interventions described themselves as operating from this orientation or having made this shift, but there was a common acknowledgment that this was an optimal feature of trying to engage clients who had not been successfully engaged in other ways. One informant referred to this shift in orientation from the perspective of not yet having made it:
I think about the Learning Session in LA [initiative-wide bi-annual meeting] when someone made a comment about outreach versus reaching out, and how those two things might be a little different. I think the way we do outreach at the ID clinic is still expecting people to respond to us versus really going to them. … I think there is value added in being in the community, going to places that are frequented by the folks we serve. Versus, “I tried calling three times,” or “I tried texting,” or “if someone randomly shows up at the front desk, let me know.” Those are good things, but I don’t know. It still feels a bit like “come to us” versus “we’re going to try to meet you.”
—(Administrator, hospital-based clinic, Substance Use)
Understanding the context of people’s lives
Embedded in descriptions of this orientation shift was the notion of not just centering a patient’s needs but that the higher, more complex, or more invisible those needs may be, the more important it becomes to understand the context of clients’ lives. Implementers repeatedly anchored descriptions of engagement strategies within the broader context of their clients’ lived experiences, demonstrating that understanding the client is a precondition for knowing how to care for them.
Trying to meet them while they’re in the facility is so critically important because [in incarcerated settings], there’s almost no human connection. I mean, just at a fundamental—people are in there living extremely solitary lives. There’s a basic human need for socialization, for conversation with other people who they can trust and not be worried that they’re going to be taken advantage of, physically harmed or threatened, or used in some way.
—(Project management, combination setting, Incarceration Experience)
Flexibility: “We can figure it out”
Informants from all focus areas further emphasized flexibility as a critical principle underlying this enhanced client-centered orientation. Implementers reported applying more flexibility in their communications with and expectations of clients enrolled in their intervention.
I tell my patients, “I’d rather see you than have you see an urgent care person. If I can see you, call me early in the morning, and we can figure it out.”
—(Medical provider, combination setting, Substance Use)
We have that policy here, in general, of just not giving up on people. So, it’s not like two no-shows and you’re discharged from the practice. Because I can tell you that every single person in [the intervention] would have been discharged already. … They need that flexibility.
—(Data management, community-based service organization, Telehealth)
Organizational flexibility was also key, particularly when it came to staffing. In some cases, specific staff members emerged as especially effective at building rapport or navigating networks, and organizational flexibility meant shifting proportions of responsibilities in real-time, based on these dynamics. As implementation progressed, some teams reported identifying staffing gaps related to unexpected client needs. One site reported reshaping its staffing plan based on a common client need that emerged during enrollment:
[We learned that] the majority of the patients enrolled in the program were sexual assault victims. So having to navigate that and really come to terms with that, we needed a separate behavioral health person just specific for the grant, and that was an adaptation.
—(Case management, community-based service organization, LGBTQ+ Youth)
Implementers further reported applying flexibility to how they internally measured the success of both client outcomes (e.g., medical visit attendance) and implementation outcomes (e.g., program completion rates). For many sites across interventions, enhanced client-centered care meant reconsidering or modifying how implementers defined success for their clients’ participation in the intervention. Implementers we interviewed were mindful of the overarching goals of sustained engagement in care and viral suppression but often spoke of what they personally considered to be a success with their clients, rooted in an understanding of and respect for the bigger picture of their clients’ lives, goals, and relationships with their own health and well-being.
Especially working with the population that we serve at this clinic, I think you have to focus on small successes. I was just talking about one the other day with our psychiatrist. This guy, he hasn’t shown up for a few weeks for his therapy appointment. He basically told me he kind of wanted to take a break from it for a second. And even though he said he wants to take a break, or he hasn’t been coming to therapy appointments, I still consider it to be a success because this guy was referred to therapy multiple times and didn’t show up, didn’t engage, very guarded. … I had to do a lot of rapport-building with him just to get him in the door.
—(Counselor, hospital-based clinic, LGBTQ+ Youth)
Intervention tailoring
Implementers reported operationalizing enhanced client-centeredness in diverse, often site- and intervention-specific ways, but in this analysis, we labeled a common approach that spanned focus areas as highly individualized, trauma-informed 41,42 engagement strategies.
Informants described an elevated praxis in which care was trauma-informed and tailored with consideration to clients’ specific barriers, goals, and circumstances. This tailoring happened at an individual level and at a community level. One site, for example, tailored its care delivery to the population’s needs, where traversing various gang territories to get to a clinic would be especially complicated for many recently incarcerated clients.
One of the things that [our champion] has been very aware of are issues related to potential gang affiliations and crossing gang lines. If our clinic is in a place where it’s not safe for a client to travel to, it can make it hard to come for an HIV care visit. This is what prompted our focus on delivering care through mobile van outreach.
—(Data management, university-based clinic, Incarceration Experience)
At the individual level, implementers reported making myriad decisions, large and small, about care delivery in direct response to various regulating elements of a client’s life. Informants described being mindful of the traumas that clients had experienced—and continued to experience—socially, structurally, and interpersonally and integrated this mindfulness into intervention delivery and client interactions. For some clients, trauma was emotional and relational, and the interventionist took care to avoid reinforcing or calling upon that trauma in the course of responding to client behavior, be it drug use, missed appointments, or reincarceration.
And you got to be careful, because these are individuals that have been stigmatized. These are individuals that have lost relationships because of their addiction. I’m sure the majority of them have been made to feel that they’ve let people down. So, we don’t want them to feel that they’re letting us down.
—(Case management, hospital-based clinic, Substance Use)
For other clients, trauma events, such as sexual assault, parental abuse, and intimate partner violence, were an active dimension of receiving HIV care, navigating communications, and taking medications regularly. For still others, interacting with health care providers and settings had been a source of complex historical trauma, and informants described both the promise and the peril embedded within efforts to build rapport and trust with such clients.
She hadn’t been in the clinic in several years. She was traumatized by something that had happened to her in the clinic and had not come, and so this is actually life-changing for her to be routinely engaging, and so it’s just huge. And I’m hoping that we’ll get to a place of stability for her so that we can start to tackle her medical issues.
—(Program management/medical provider, hospital-based clinic, Substance Use)
III. Leveraging the relationship: “Connect on a human level”
Three types of relationships featured prominently in interviews across focus areas: relationships between implementers and clients, relationships between program staff and partners within their organization, and relationships between program staff and external partners.
Relationships between implementers and clients
The theme of relationships between implementers and clients was interwoven throughout interviews, across informants, sites, and interventions, playing a crucial, multi-dimensional role in trying to engage clients.
The relationships created and sustained through interpersonal communication between implementers and clients could generate or degrade trust and rapport. It served for some as the primary catalyst to and vehicle of engagement. The connection between a client contending with complex barriers to engagement and a care provider trying to engage them was shown to be as delicate as it was powerful, and one that implementers worked hard to cultivate effectively.
Relationships that facilitated client engagement were described as overtly client-centered, patient, nonjudgmental, and celebrating any successes, regardless of the client’s overall participation in or adherence to the program.
For me, it became just connect with her on a human level. … March 13th, she was enrolled, and then after that, I couldn’t reach her. I couldn’t reach her, and I already know from doing the assessment she had huge mental health issues. So, while it took extra effort, I said, “I’m not going to let up on her. I’m going to keep texting her.” But I just really made it more personal. I didn’t mention anything about [the intervention]. And this week she sent me a text message that almost floored me. I’m sorry. I’m going to get so emotional because she said, “I just want you to know—I’m so sorry. I know I pushed away from you. But you didn’t stop reaching out to me. You didn’t stop caring. And now I just want to move forward and continue with the sessions where we left off.”
—(Counselor, hospital-based clinic, Telehealth)
We further heard in interviews that for some clients, what begins as a relationship with a person or with a team or clinic can translate to a relationship with systems of care more broadly, with essential services, and with the embodied experience of being well. Informants from across interventions reflected on how the connection that implementers make with clients can last beyond the intervention:
Developing that relationship, developing that connection, hopefully trying to create a lasting tether, if you will, to the clinic that then lasts beyond the intervention was appealing to me, in thinking about some of my patients who, otherwise, don’t have a lot of connection in their outside lives.
—(Leadership, combination setting, Telehealth)
Relationships between program staff and inner context partners
Implementers from one-stop shops, hospital systems, and multi-service agencies often reported consulting with colleagues in other departments on engagement or care strategies for specific clients. Many relied heavily on other areas of the organization for referrals, and the quality of the communication and relationships between the 2iS team and these internal partners was a critical element. When the relationships were constructive, engagement was notably more successful.
We’ve had tremendous success … enrolling people who are hospitalized. … Some of these people have been referred to us, and then others, [our staff] might identify as, “Oh, this is a really good [Clinic] patient. Let’s, you know, involve them now.” Our woman who hadn’t stepped foot in the clinic in several years and is now coming daily, she is an example of somebody that we enrolled in the hospital.
—(Program management/medical provider, hospital-based clinic, Substance Use)
Teamwork within a closed system is crucial because, as informants explained, it is not uncommon for a client who has been disengaged from HIV care to pop up in another area of the hospital or agency, and the quality of the communication among departments contributes directly to the ability to coordinate across departments within that closed system:
It will happen that we have somebody who we’ve been looking for, who we would love to get back engaged in care, who is sitting in a chair 20 feet away.
—(Leadership, combination setting, Telehealth)
Relationships within the agency may also allow for leveraging existing relationships that clients have with other providers. At one telehealth intervention site, program staff enlisted the support of peer navigators who had established rapport with some of the potential participants the team was hoping to reengage in HIV care.
It just felt like the natural way to leverage the relationship that’s already been built by the peers. The peers are the ones who can identify like this client has been through XY and Z, this client is not regularly taking their medication, these are the labs that just came through. … And so, because they’ve already built that rapport because they already have the relationship with the client, it just felt like the next logical step to be like let’s make this a two-way referral.
—(Counselor, community-based service organization, Telehealth)
Relationships between program staff and external partners
Finally, relationships between program staff and partners outside the organization were reported as being extremely influential in many sites but often in different ways.
Some sites relied heavily on external partnerships for various elements of engagement, from identification of potential participants to recruitment to coordinated care. Incarcerated settings relied almost entirely on various staff and officials within the jail, prison, and court system for every level of access to information about eligible participants up to the point of their release from incarceration (and sometimes beyond). One site was so dependent upon this access that whether the intervention would be able to move forward was, at one point, seemingly hanging in the balance of a challenged reelection of the County Sheriff.
In these cases, constructive relationships were not just important, they were essential. One site implementing the incarceration experience focus area intervention was unable during pre- and early implementation to cultivate meaningful relationships with key staff members inside the prison system, and this team struggled considerably with early enrollment as a result.
Other meaningful relationships with external partners included those with departments of public health or other service agencies from which program teams could solicit referrals or to which teams could refer clients for assistance with housing, legal protection, or other supportive services. Some sites served primarily as linkage hubs, so for them, the quality of their relationships with external partners informed the quality of the referrals they could provide to their clients.
If the clients need birth certificate and ID resources, or they need food, shelter, anything that they’re lacking that’s a barrier for them to be successful with whatever goals they have, then I come in to help link them to resources that could be beneficial to them. [All our] resources are external.
—(Data management, community-based service organization, Telehealth)
Finally, Learning Sessions—biannual initiative-wide collaborative meetings—were heralded across nearly all sites in interviews as being uniquely generative. Some informants mentioned having forged unofficial partnerships with implementers from other sites to meet regularly and brainstorm novel approaches to shared challenges. This suggests the importance of developing a community of implementers, particularly in the rarified zone of implementing new strategies to address needs that have yet to be successfully met.
The EPIS framework
While these individual themes are important, as evidenced by their common identification across diverse interventions and implementation settings, it is the way that these themes relate to and interact with one another that is perhaps the most salient finding of this analysis.
The EPIS framework provides a useful cluster of constructs that relate to one another in a constant flow, allowing us to represent our findings not as static, distinct concepts but as living elements of an organism. In Fig. 1, we map our findings onto the following four primary EPIS constructs: outer context, inner context, bridging factors, and innovation factors.

Exploration, Preparation, Implementation, Sustainment (EPIS) framework representation of key findings. Visual representation of the EPIS framework (inner and outer context factors, innovation factors, and bridging factors), to which key findings from the study are applied.
In the outer context sit population needs and social determinants of health, client characteristics such as generational factors or incarceration, external partners, and the service environment (politics, policies, society, and culture). In the inner context sit our findings pertaining to the implementing individuals, teams, and agencies.
Because this analysis takes a high-level view focusing on unifying themes, we populate the innovation factors not with functional details of the individual interventions but rather with common elements of an elevated client-centered approach that we identified across focus areas (individualized, trauma-informed care and an iterative practice of assessment and adjustment).
It is with the addition and positioning of bridging factors—the relationships among clients, implementers, internal partners, and external partners—that our findings transform from static concepts to interactive features of a larger whole, a reflection of their true performance in the implementation experiences reported in KIIs. Our data demonstrate how these relationships served as the bridging, translational, and catalytic features of early implementation in the 2iS initiative.
To wit, individualized, trauma-informed care is not an out-of-the-box feature of any implementation strategy. Rather, it relies on a client-centered orientation that endeavors to understand the context of clients’ lives and requires flexibility in the intervention delivery and a flexible idea of how success for an individual client should be considered. Making thoughtful, effective, and iterative adjustments to meet client needs relies upon understanding the context of clients’ lives, a high level of operational flexibility, and an orientation of delivering care that firmly centers the needs of the client and privileges it over the allure of routinized care.
The relationships here provide the circulatory system of information, connection, trust, and access connecting these implementation elements and making them what they are. Understanding the context of a client’s life requires connection with that client and the rapport necessary to be granted access to private struggles and strengths. Relationships with other service providers who have existing connections with these clients further expand the capacity for understanding and tailoring how one offers them services. Partnerships with individuals who serve as points of entry to foundational support services—such as housing, food, or legal aid—expand the scope of client needs that an interventionist can help a client address. Relationships with people who serve as gatekeepers to systems such as a county jail or courthouse can help mediate and mitigate the trauma of clients moving through systems of incarceration.
Figure 2 provides a concrete example of this interplay at work. In this figure, we provide an interview excerpt, a truncated version of which appears in our thematic findings above. Within this single excerpt, we can see our prevalent themes at work, as well as the dynamic network of relationships driving them.
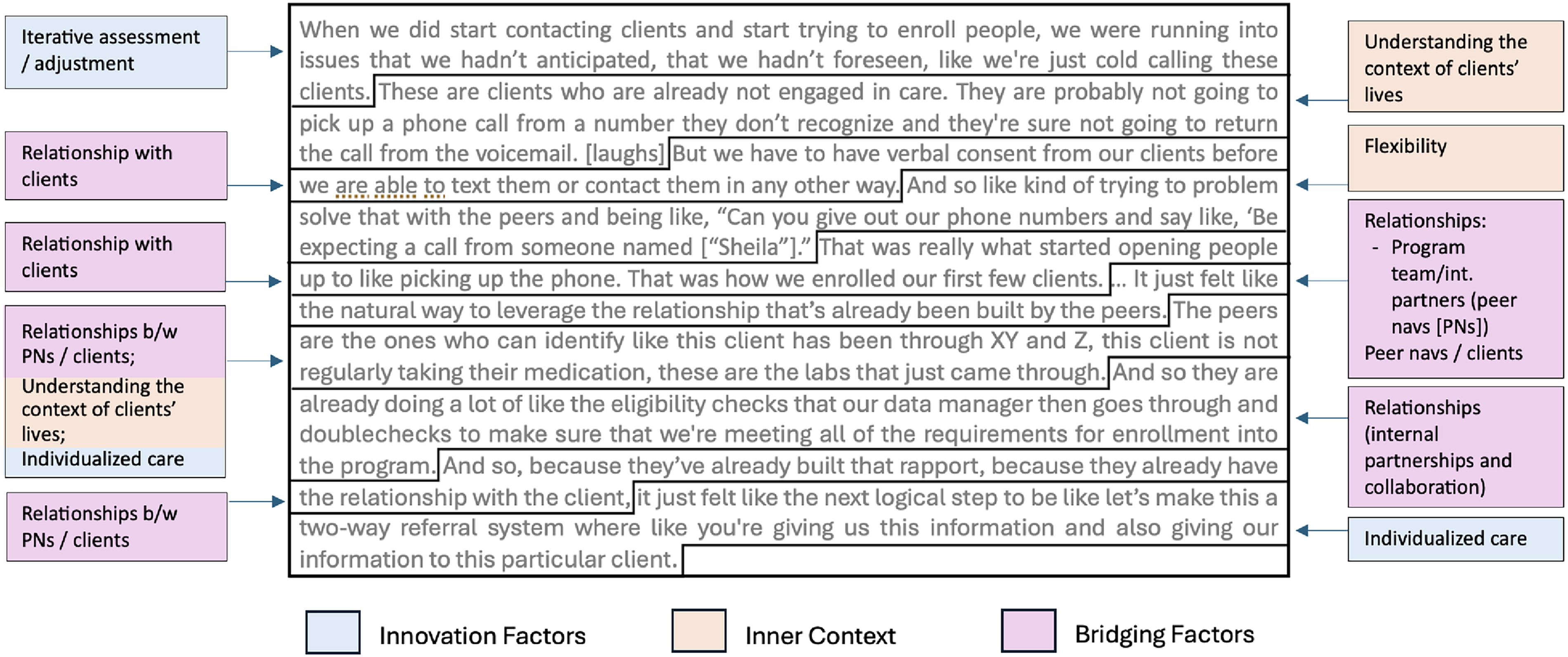
Application of findings themes applied to a single-interview excerpt, by Exploration, Preparation, Implementation, Sustainment (EPIS) construct. A visual representation of how multiple themes from study findings—and the EPIS constructs into which they fit—are woven throughout a single-interview excerpt.
Observing these themes as a whole within the EPIS framework, we can further identify a logical shift in how client service is considered, mirroring the shift in orientation and ethos that informants described. What has endured as a vexing tautology—that the most difficult-to-engage clients are the most difficult to engage—represents a closed logical premise, descriptive perhaps but not instructive. Our data, particularly the implementer insights linking the high needs of unengaged clients with a drive to understand the lived context from which those needs emerge, crack this tautology open. The logic behind intervention delivery became instead: if the most complexly underserved people with HIV are the most difficult to durably engage in HIV care, engagement efforts must address clients’ complex needs in addition to offering HIV care.
Discussion
Our findings contribute broadly to ongoing efforts to end the HIV epidemic by illuminating the link between the seemingly unrelated needs facing clients in their daily lives, their ability to achieve desirable clinical outcomes, and—even more salient in the study of implementation—what it will take to successfully serve them.
This study adds to an evidence base that highlights the complex interplay of social, environmental, and logistical factors that affect HIV care engagement among underserved populations in the United States 43,44 and the promise of population-focused interventions that consider these determinants in the goal of improving health outcomes. 45
Tailored services and effective client–provider communication strategies have been shown to facilitate engagement among those who experience HIV health disparities. 46,47 One 2020 study highlights both the importance of interpersonal relationships and social support in helping underserved clients achieve viral suppression and the critical role of understanding the lived context in which people with HIV operate. 48 Models for how to understand trauma within the context of HIV services continue to emerge, 49 –51 and trauma and HIV have begun to be studied as syndemic conditions. 42
The findings from this study, particularly when viewed in relation and interaction with one another as illustrated through the EPIS framework, carry implications for clinical practice and policy changes. Teams implementing innovative strategies to engage clients who have not been successfully engaged through other means may benefit from adopting the following approaches: An enhanced client-centered orientation, with a focus on understanding the context of clients’ lives. A high level of flexibility (organizational and staffing flexibility, flexible care delivery, and flexible measurements of success). An individualized, trauma-informed approach to recruitment and intervention delivery. A conscious and methodical approach to cultivating and strengthening relationships between implementers and their clients, between all members of a client’s “team” (more broadly defined as people occupying different roles across a service delivery organization), and between members of this team and partners in external agencies and sectors.
These approaches may also benefit other key populations and people with HIV requiring different services as they age. 52 They should be considered when advanced or specialized implementation measures are needed.
Limitations
This analysis was meant to be broad and identify common themes across a wide range of highly varied intervention implementations. This breadth, however, partially obscures some of the variations that can provide an important context to how and why some strategies were deployed and whether and why they were successful. This is critical information, particularly as innovative strategies become increasingly central to addressing remaining HIV care continuum gaps, and implementation of these strategies needs to become more easily achieved by service providers. We anticipate further analyses of the outcomes of this initiative that explore barriers, facilitators, and adaptations at the intervention and focus area levels.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the RWHAP site staff who participated in this initiative and to the clients they serve for their willingness to participate in these innovative programs. They also would like to thank the 2iS Coordinating Center at the Fenway Institute and AIDS United for their ongoing partnership and collaboration. The authors are also grateful to their HRSA/HAB colleagues for their leadership and support throughout the project.
Authors’ Contributions
L.M. is the lead and corresponding author. G.M.R., J.J.M., B.B., S.B.S., P.S., A.S.K., D.P., and K.A.K. conceived the overall study design and selected and tailored the theoretical approach. K.A.K. designed the qualitative approach and analyses. D.P. contributed to the refinement of the theoretical approach and the study design. L.M., K.A.K., A.T.B., and A.M. performed all qualitative data collection and analyses. M.A.G., M.P., and G.H. contributed to data collection. All authors contributed to the drafting, reviewing, and revision of the article.
Data Access Statement
Due to ethical restrictions, data are available only upon request. Our data consist of interviews with participants who work together on small teams that often have only one person in each role and which include details and contextual information that could reveal the identity of the participants. Further, participants did not consent to transcripts of their interviews being publicly available. While these transcripts have been technically deidentified, there is no way to ensure that they are functionally deidentified given the highly contextualized nature of the personal experiences participants shared.
Researchers who meet the criteria for access to confidential data may send requests for the interview transcripts to the Human Research Protection Program (HRPP)/IRB at the University of California, San Francisco at 415-476-1814 or
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This project is supported by the HRSA of the US Department of Health and Human Services (HHS) RWHAP Part F Special Projects of National Significance under grant number U90HA42154 in the amount of $4,200,000 awarded to the Regents of the University of California, San Francisco. No percentage of this project was financed with nongovernmental sources. The contents are those of the author(s) and presenter and do not necessarily represent the official views of, nor an endorsement by, the HRSA, HHS, or the US government. For more information, please visit HRSA.gov.