
Abstract
The Centers for Disease Control and Prevention recommends universal human immunodeficiency virus (HIV) screening in emergency departments (EDs) for patients (above 13 years). In 2017, Jackson Health System (Miami, FL) established a successful adult ED-based universal opt-out HIV screening program. However, when expanded to its affiliated pediatric ED (PED) as an opt-in protocol, only 1.3% of all adolescents received universal screening (only 1.7% were tested based on their chief complaints). We explore barriers to PED testing by comparing the attitudes of providers, patients, and caregivers. Institutional review board-approved surveys were administered anonymously to each group. Raw aggregate data were analyzed for trends. Providers’ responses were stratified by role and responses were compared via a Mann−Whitney test. Twenty-four providers responded; they agreed that testing is warranted (x = 3.58 σ 1.32) and not time-consuming (x = 2.33 σ 1.05). There was no agreement on the perceived role of providers to perform testing. Attendings reported a high chance of breaching patients’ confidentiality (x̄ = 3.27 σ 1.35), while nurses did not (x̄ = 2.33 σ 1.51). Of the 62 patient responses, 62.9% were amenable to testing, 69.4% would consent to 4th-generation serum testing if less invasive options (e.g., oral swabs) were unavailable, and 77.4% would inform caregivers of results. Of the 37 caregiver responses, 91.9% felt comfortable with their child consenting to testing. In this population, patients and caregivers appear amenable to universal screening. Low testing rates may be explained by providers’ disagreement on their role to perform testing and concerns about confidentiality. Future studies should further explore protocol-based flaws and providers’ views.
Introduction
The Centers for Disease Control and Prevention (CDC) recommends universal, opt-out human immunodeficiency virus (HIV) screening for patients aged 13 and older across all health care settings, including emergency departments (EDs). 1 This recommendation is in response to the ongoing HIV epidemic in the United States. Despite advances in testing and treatment since the start of the epidemic in the 1980s, HIV remains a major public health concern. In 2021, there were approximately 1.2 million Americans living with HIV, with 36,136 new diagnoses reported in that year alone. 2 Despite the high number of new and existing cases of HIV in the United States each year, only about one in eight people living with HIV are aware of their diagnosis. 3
Adolescents are a particularly vulnerable population, with regard to HIV transmission, due to high-risk sexual behaviors, low HIV screening rates, and inconsistent access to regular health care. 4 –6 In 2019, adolescents and young adults (aged 13–24) comprised 21% of new HIV diagnoses in the United States. 4 Although young adults between the ages of 20 and 24 comprised the majority of diagnoses within this population, adolescents (aged 13–19) remain an important target population for HIV screening. 4 It has been estimated that nearly 50% of adolescents living with HIV in the United States are unaware of their infection and that the actual time of HIV infection precedes a formal diagnosis by an average of 2.7 years. This places adolescents at a higher risk for developing disease-defining illnesses and transmitting HIV to their sexual partners. 4,7 –9 Therefore, implementing universal screening in the adolescent population may reduce delays in diagnosis and treatment among young adults. 7
Prior literature demonstrates missed opportunities for screening adolescents in the ED setting. In a 2018 retrospective chart review of patients diagnosed with HIV at Children’s Healthcare of Atlanta, 79% of these patients were adolescents, 41% of all cases presented with late stage disease, and 24% of all cases presented with disease-defining illnesses, such as pneumocystis pneumonia or mycobacterial disease. 10 These findings further highlight the need for standardized approaches to adolescent HIV screening, particularly in the ED—a place through which both high risk and undiagnosed patients seek care.
In response to the CDC’s HIV screening guidelines, universal opt-out screening programs have been successfully implemented in adult EDs. 11 However, the field of pediatrics has not uniformly implemented universal HIV screening protocols for adolescents. Only a handful of studies have described the implementation of similar programs in PEDs or explored potential barriers to universal HIV screening in the adolescent population. Previously highlighted demographic and health care system-specific barriers include race, sex, age, ED crowding, staff availability, cost, individual perception of HIV risk, fear of needlesticks for HIV testing, the presence of a parent or guardian, and the type of ED in which adolescents receive care (i.e., PED vs. adult ED). 12 –14 In the absence of universal HIV screening protocols, most PEDs employ targeted testing, whereby providers offer HIV testing based on their perception of the adolescent patients’ risk. 5 A 2022 study comparing universal screening rates with targeted HIV testing in a large, urban PED found that providers were more likely to offer testing to patients who were older (at least 16 years old), female, or presenting with a gynecological or genitourinary complaint. This study suggested that targeted testing may miss key populations of adolescents who are at risk for HIV, such as young men, who are known to be disproportionally affected by the disease. 5 Given that adolescents more frequently seek care in EDs than in other health care settings, 5 correctly defining and addressing PED barriers to universal HIV screening may lead to earlier detection and treatment of this infection in patients who would otherwise slip through the cracks of the health care system.
There is a great need to improve universal HIV screening in PEDs in Florida due to the high incidence of HIV in this state. In 2020, Florida had the third highest rate of new HIV diagnoses (in both adults and adolescents) in the United States. 15 Within Florida, Miami-Dade County is particularly vulnerable with regards to HIV. Miami-Dade County is the seventh most populous county in the nation, and it is an area of great socioeconomic need, leading to well-documented health care disparities in this community. 16 In 2016, Miami-Dade County had the second highest rate of new HIV infections in the country. 17 These uniquely high rates of HIV warrant robust universal HIV screening protocols in the ED to better detect and treat HIV. In response to this need, the “Frontlines of Communities in the United States” (FOCUS) initiative was launched in 2017 in Miami-Dade County’s tertiary public hospital system, Jackson Health System (JHS). This program integrates universal, opt-out testing for HIV and other sexually transmitted infections (STIs) into the existing workflow of the ED. In this opt-out model, patients are informed that HIV testing will occur in conjunction with the blood work required for their ED visit and that they may decline testing if desired. FOCUS has been successful in the adult setting, and it has since expanded to satellite adult EDs within the health system. However, attempts to expand the program to screen adolescents (13–18 years) through a universal opt-in protocol at JHS’s affiliated PED (Holtz Children’s Hospital) have not been successful. Given that blood draws occur less frequently in PEDs than in adult EDs, Holtz utilizes an opt-in model, whereby staff counsel patients and their caregivers about HIV and provide them with the option to consent to serum testing during the visit. As part of an ongoing quality improvement initiative to improve universal HIV screening of adolescents in the Holtz PED, this study aims to compare the attitudes of providers, patients, and their caregivers toward universal HIV screening, describe the influences of these attitudes in screening in the PED, and identify other barriers to screening in the adolescent population.
Methods
Institutional review board-approved surveys were administered to patients, their caregivers, and PED providers at Holtz PED from January 14, 2022, to March 16, 2023. Written consent was obtained from all participants. PED patients were eligible for participation if they were at least 13 years of age. (Note that Holtz PED can treat patients up to 21 years of age.) Caregivers presenting with eligible adolescent patients were also eligible to participate in the study. Providers, including attending physicians, fellows, rotating residents, and nurses, were also eligible for participation. Participants were excluded if they presented with an immediately concerning or unstable condition.
Three surveys were designed—one for patients, one for caregivers, and one for PED providers. These surveys were adapted from a similar study at Children’s Healthcare of Atlanta (affiliated with the Department of Pediatrics at Emory University School of Medicine) in 2015 and were distributed with the permission of the original authors, Middlebrooks et al. 18 The patient and caregiver survey questions were designed to assess participants’ baseline knowledge of HIV, potential interest in free HIV testing while in the PED, and preference of either oral cheek swabs or more accurate serum 4th-generation testing. The patient and caregiver surveys also assessed potential reasons for declining HIV testing in the PED, including cost, confidentiality concerns, recent testing in the last 6 months, lack of perceived risk for HIV, and delays in timely care. The provider survey was designed to assess perceptions of the relevance and feasibility of universal HIV screening in the PED setting, particularly with regards to the presence of caregivers, the ability to create a confidential space for counseling and diagnosis disclosure, and the ability to perform timely testing without disrupting the PED workflow.
The provider surveys were administered via email through a secure Qualtrics link. PED administrative staff also disseminated the Qualtrics link at staff meetings and nursing huddles for optional, anonymous participation. The patient and caregiver surveys were administered either via a QR code for a secure Qualtrics link or via a paper copy, based on personal preference. Trained medical students on the research team identified eligible patients and caregivers, consented them, and administered the survey while they were in the PED waiting room, prior to the start of the PED visit. Patients and caregivers were instructed to fill out their surveys separately, but they were not physically separated during the consent process or survey administration. Surveys were offered in English and Spanish. Spanish interpreters were used for the consent process as needed.
Data analysis was performed in a stepwise fashion. First, raw aggregate data were analyzed for trends in providers,’ patients,’ and caregivers’ responses to survey questions. Next, individual questions in both patient/caregiver and provider surveys were analyzed separately. A 5-point Likert scale (where 1 corresponds to “strongly disagree” and 5 to “strongly agree”) was used to evaluate providers’ attitudes toward HIV testing in the PED setting, and median values were determined for responses to each question. For the provider surveys, data were stratified by provider role (i.e., attending physicians, nurses, and residents), and a Mann−Whitney test was used to compare the results between the different provider groups. For the patient/caregiver surveys, particular attention was paid to the patients’ current sexual activity, patients’/caregivers’ prior knowledge of HIV, preferred type of HIV test administered, and with whom the patients would disclose positive HIV testing results.
Results
During the course of the study, a total of 33,234 patients were seen in the PED, 6421 of whom were adolescents between 13 and 18 years of age (Fig. 1). A total of 197 adolescents (approximately 3% of all adolescents) received an HIV test during their visit, and only 43% of these adolescents were tested through the FOCUS universal screening protocol; the remaining 57% received targeted physician-driven testing as indicated by their presenting complaints (Fig. 1).

Adolescent patients who received HIV testing, compared with the overall PED census during the time of the study. Universal screening refers to adolescents who were tested via the FOCUS opt-in universal screening protocol. Targeted testing refers to adolescents who received HIV testing that was ordered at the providers’ discretion—based on the presenting complaint or the providers’ perception of the adolescents’ risk. PED, pediatric emergency department.
Provider surveys
A total of 24 provider surveys were completed: 11 pediatric emergency medicine (EM) attending physicians (PEM), 7 residents, and 6 nurses. There was agreement among providers that Miami-Dade County’s patient population has a high enough prevalence of HIV to warrant screening (x̄ = 3.58 σ 1.32; Fig. 2) and that HIV screening would not be too time consuming for a PED visit (x̄ = 2.33 σ 1.05). In all subgroups, views differed on the role of PED providers to provide HIV testing; however, PEM responses trended toward disagreement, while nurses’ and residents’ responses were more variable (Fig. 3). There was a statistical significant difference between nurses and PEM, regarding views on maintaining confidentiality while providing HIV counseling and performing testing in the PED. PEM believed that there was a high chance of breaching patients’ confidentiality (x̄ = 3.27 σ 1.35), while nurses did not (x̄ = 2.33 σ 1.51).
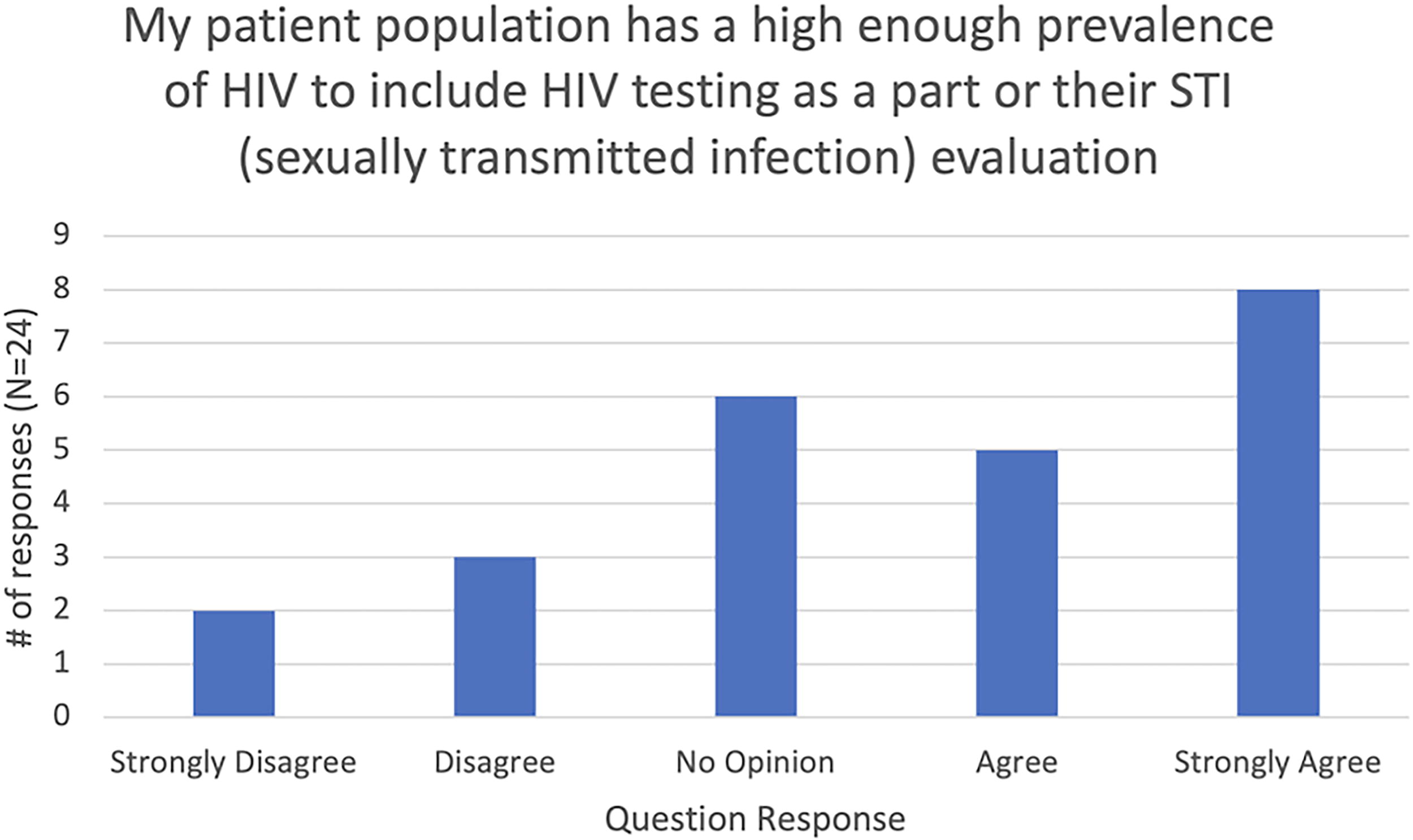
PED providers’ views on the relevance of HIV testing in their patient population. Responses were not stratified by providers’ roles. PED, pediatric emergency department.

Providers’ responses to their role in performing HIV screening in the PED, as stratified by provider type. PED attending physicians are abbreviated as “PEM.”
Patient surveys
Sixty-two patients (aged 13–21) completed the survey, and the average age of the participants was 15.8 years. A total of 41.9% respondents were identified as male and the majority of the patients identified as either African American (40.3%) or as Hispanic (46.8%). Only 32.3% of patients reported sexual activity (Table 1). However, 62.9% of patients stated that they would consent to free rapid HIV testing if offered and 69.4% of patients stated that they would still consent to a 4th-generation serum test if less invasive options, such as saliva or oral swab tests, were unavailable (Table 1). When asked what they would do if they tested positive for HIV, 77.4% of patients indicated they would inform their caregiver and 64.5% of patients indicated that they would seek medical attention (Table 1).
Patients’ Responses to Selected Survey Questions
Caregiver surveys
A total of 37 caregiver surveys were completed—34 in English and 3 in Spanish. Of those who completed the survey, 83.8% identified as female, 56.8% identified as African American, and 37.8% identified as Hispanic. Only one respondent had never heard of HIV (Table 2). Social media was the most common platform by which respondents had previously learned about HIV (56.8%), with clinical settings (i.e., a clinic, hospital or ED) as a close second (51.4%, Table 2). Overall, 91.9% of caregivers indicated that they would feel comfortable with their child consenting to HIV testing during the PED visit (Table 2).
Caregivers’ Responses to Selected Survey Questions
Discussion
This quantitative study seeks to better understand the attitudes toward HIV screening and existing barriers to HIV screening in the PED setting. Our findings suggest that patients and caregivers in the Holtz PED are generally aware of HIV, would be open to universal screening, and would be willing to discuss positive test results with each other, as well as with health care professionals. In contrast, providers do not agree about their role in providing HIV screening in the PED setting, and there are disagreements among provider types regarding the ability to maintain confidentiality during the screening process. However, providers feel that HIV testing is warranted in this population and that it would not result in significant delays in workflow.
Although our findings suggest that patients at the Holtz Children’s PED are amenable to testing, the universal screening rates remain low. Only about 3% of all adolescents presenting to the ED during the time of the study were tested for HIV, and only about 1.3% of all presenting adolescents received universal screening during their visit. Overall, the existing free, opt-in screening process does not appear to be successful in Holtz Children’s PED, as it fails to capture a significant population of adolescents who may be at risk for HIV.
The presence of a caregiver has been posed as a theoretical barrier to universal PED screening, due to concerns for breaching adolescent patients’ confidentiality. However, in this study, both patients and caregivers perceived HIV screening to be both feasible and acceptable during a PED visit. The data also suggest that both patients and caregivers in this community have a baseline awareness of HIV and would likely seek medical attention (either for themselves or for their dependents) in the setting of a positive HIV test. These findings are consistent with those of a prior study, which demonstrated that the presence of a caregiver did not impede adolescents’ participation in universal HIV screening. 14 Perhaps the low percentage of adolescents tested through universal PED screening at Holtz may not be due to patients’ or caregivers’ concerns about confidentiality or due to a lack of awareness of HIV in this population. In fact, our data suggest that providers’ perceptions may create barriers to universal HIV screening at this site. In this study, PEM felt that there was a high likelihood of breaching confidentiality in this setting. The success of universal screening initiatives is contingent upon provider buy-in, with leaders in the department educating other staff and encouraging participation. If PEM do not feel that HIV counseling, testing, and result disclosure can be done in a confidential manner, they may be less likely to encourage staff participation in this initiative.
Additionally, providers may be less likely to bolster the initiative if they are unsure of their role in universal HIV screening. Traditionally, the primary purpose of the ED has been to address acute complaints, rather than to perform preventative screening, which can be done in the outpatient setting. Although the providers in our study felt that HIV testing was warranted in this population and did not feel that universal HIV screening would be too time-consuming for a PED visit, there was no consensus as to their role to perform such screening as PED providers (although there was a trend towards disagreement in PEM responses). If PED providers feel that it is not their role to perform universal HIV screening—a preventative measure that is not always related to their patients’ presenting complaints—they may be less likely to encourage departmental participation in the initiative. Future studies and quality improvement initiatives should seek to explore this further and should perhaps seek to educate PED providers about the relevance of testing in the PED. Many adolescents and young adults first encounter the health care system through the ED and are less likely to seek care in outpatient settings. 5,19 Therefore, the PED may be an excellent place for universal HIV testing—creating opportunities for earlier detection and treatment of HIV in this population.
Although not explored in this study, flaws in the existing PED workflow may also create barriers to universal HIV screening. For example, currently, Holtz PED nurses are required to ask patients about HIV testing as a part of their online triage questionnaire. There is a force function in place to ensure that the triage process cannot continue until this question has been answered. However, this question also includes an “N/A” option. Anecdotally, it has been observed that “N/A” is sometimes selected by default during the triage process. Therefore, some patients may not be asked about HIV screening at all during their visit. Future studies should explore PED workflow issues, as they could be reflective of potential underlying barriers to screening, such as the staff’s lack of comfort with talking to patients and caregivers about HIV or a desire to triage patients more efficiently during busy shifts with high patient volume and acuity.
Given that universal screening for adolescents is a relatively novel approach, this study offers encouraging evidence for PEDs to implement such programs into their existing workflow. It showcases an understanding of the need for free STI screenings in the Holtz PED patient population and provides valuable recommendations to the current screening team.
It also highlights opportunities for enhancing PED providers’ understanding of HIV screening and its relevance to the PED through educational initiatives. Future studies should address protocol-based flaws and providers’ views on testing in the PED.
Strengths and Limitations
This study contributes significantly to the limited body of literature on barriers to universal HIV screening in the PED—most of which are either theoretical opinions or systems-based barriers. In particular, this study highlights some discrepancies between the perceptions of the providers and those of patients/caregivers regarding HIV screening in this setting. Understanding the views of all parties involved in the screening process is critical to improving screening rates in the PED.
This study had several limitations. The overall number of participants was low, with a notable lack of caregivers’ responses, in comparison to patients’ responses. Factors contributing to the small sample size may include a lack of a desire to complete a survey while waiting to be seen in the ED, receptiveness of participants toward medical students’ counseling about the study, staff’s availability to complete surveys during their shifts, and seasonal and shift-based fluctuations in adolescent patient volume. This study may not be generalizable to other PEDs in the United States, given South Florida’s particularly high rates of HIV and Miami-Dade County’s “minority-majority” patient population. (Of note, this study’s findings appear to be reflective of our patient population at Holtz PED. JHS, which includes Holtz PED, is the primary health care system for patients in Miami-Dade County. As one of the largest public hospital systems in the country, it also serves as a catchment area for South Florida.)
There may also be additional systemic barriers unique to Holtz PED that were not considered in this study; these barriers may explain the discrepancy between the percent of patients willing to be tested and the percentage actually tested through the screening protocol at this site. In Holtz’s current universal screening process, patients are asked about HIV testing while in triage, which often occurs at the front desk of an open waiting room—generally in the presence of caregivers and without any clear separation from other patients and their families. The lack of a private space to conduct conversations about HIV may help explain providers’ concerns about confidentiality.
Additionally, this study does not explore barriers to linking patients to appropriate care and treatment after identification of a new HIV infection through universal screening. This is critical at both a patient and population level, as low rates of linkage to care (LTC) among those diagnosed via universal protocols have been documented in literature. 20,21 JHS has an intensive, interdisciplinary LTC protocol, starting in the ED and extending to the outpatient setting. This is set up and overseen by members of the FOCUS project. (FOCUS oversees JHS’s adult and PED-based universal protocols). FOCUS team members work with the medical teams to ensure timely LTC. It has been documented in literature that intensive LTC protocols may improve LTC rates in adult EDs with universal screening programs. 21 Therefore, future studies should explore LTC rates and overall success of FOCUS’ LTC protocols at both the JHS adult ED and Holtz PED.
Footnotes
Acknowledgments
The authors would like to thank the PED providers, patients, and caregivers for participating in the study. The authors would also like to thank Dr. Claudia R. Morris (Emory University Department of Pediatrics, Pediatric Emergency Medicine Division) and Dr. Colleen K. Gutman (University of Florida Department of Emergency Medicine) for their advice and insights during the development of this study. This FOCUS (on the Frontlines of Communities in the United States) project is supported by funds from the Miami-Dade County Department of Health and Gilead Sciences, Inc. FOCUS funding supports HIV/hepatitis C (HCV) screening and linking patients to the first medical appointment after diagnosis. FOCUS funding does not support any activities beyond the first medical appointment and is agnostic to how FOCUS partners handle subsequent patient care and treatment.
Authors’ Contributions
N.P.N. conceptualized and designed the study, oversaw study activities, modified questionnaires for data collection, coordinated and supervised data collection, interpreted the data, drafted the article, and implemented all critical revisions of the article. A.K.J. and M.B. conceptualized and designed the study, modified questionnaires for data collection, coordinated data collection, carried out data analysis and interpretation, contributed to the initial article draft, and critically reviewed the article. M.B. also designed the data collection instruments, oversaw the data collection process, and acquired funding for the study through FOCUS. A.K.J. and M.C. were responsible for data acquisition. M.C. also contributed to study design and critically reviewed the article. D.H. conceptualized and designed the study, provided statistical expertise, led data analysis and interpretation, and critically reviewed the article. G.G.R. serves as the FOCUS site coordinator for Jackson Health System and helped conceptualize, design, and execute the study. L.M. developed the original surveys for a study at Emory University in 2015 and authorized this team to adapt and disseminate them for the purpose of this study. L.M. also critically reviewed the article. P.P., H.C., and L.L. conceptualized and designed the study, oversaw study activities, assisted with data interpretation, and critically reviewed the article. All authors approved the final article as submitted and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This FOCUS project is sponsored by the Miami-Dade County Department of Health and Gilead Sciences, Inc. FOCUS funding supports HIV/HCV screening and linkage to the first medical appointment after diagnosis. FOCUS funding does not support any activities beyond the first medical appointment and is agnostic to how FOCUS partners handle subsequent patient care and treatment.