
Abstract
Increasing use of mobile phones creates growing concerns regarding harmful effects of radiofrequency nonionizing electromagnetic radiation on human tissues located close to the ear, where phones are commonly held for long periods of time. We studied 20 subjects in the mobile-phone group who had a mean duration of mobile phone use of 12.5 years (range 8–15) and a mean time use of 29.6 h per month (range 8–100). Deaf individuals served as controls. We compared salivary outcomes (secretion, oxidative damage indices, flow rate, and composition) between mobile phone users and nonusers. We report a significant increase in all salivary oxidative stress indices studied in mobile phone users. Salivary flow, total protein, albumin, and amylase activity were decreased in mobile phone users. These observations lead to the hypothesis that the use of mobile phones may cause oxidative stress and modify salivary function. Antioxid. Redox Signal. 18, 622–627.
Introduction
Several reviews and epidemiological studies regarding the possible adverse health consequences of mobile phones have been published (6, 8). Although some have suggested that there is a correlation between NIER exposure and the development of tumors in an adjacent organ (8), and most of these articles state that evidence for a relationship between the use of mobile phones and cancer is weak to nonexistent (6). In a recently published article, Sadetzki et al. examined the correlation between parotid gland tumors and mobile phone use (8) and found a positive dose–response trend. Interestingly, various studies that examined the association between NIER and/or mobile phones and oxidative stress (a potential contributor to the risk for developing cancer) found contradictory and indecisive results. For example, in two recently published articles, no effects of electromagnetic radiation and mobile phones were demonstrated on oxidative stress indices in the eyes or blood of rat and rabbit models (3). In contrast, in another recently published article, Aydin et al., who studied the effect of electromagnetic radiation on lymphoid organs in a rat model, found induced oxidative damage, only tissue specific, and occurring only in immature rats, not in mature rats (2).
The anatomic location of the parotid gland (at the anterior border of the external ear and between the mandibular ramus and the sternocleidomastoid muscle, 4–10-mm deep under the skin surface) makes it a plausible candidate for influence by exposure to mobile phones, on the side of the head where the mobile phone is held. Hence, the secreted saliva, loaded with cells and macromolecules, is an ideal candidate for such a study.
The current study compared salivary secretion, focusing on various salivary components and oxidative stress indices, between users of mobile phones and nonusers, thus examining the effect of mobile phone use on human cells and macromolecules at its immediately proximal region.
Twenty healthy subjects (10 men and 10 women), mean age 51.2 years (range 32–63), participated in the research (mobile group). We assumed that subjects who were exposed to more extensive NIER would be more likely to exhibit salivary composition changes. Therefore, we defined our study group as subjects with excessive use of mobile phone—more than 8 years of mobile phone use and above 8 h’ usage per month. These were compared to a control group of 20 subjects, matching in age and gender who do not use a mobile phone (nonmobile group), most of them (90%) are deaf. These individuals were born deaf in almost all cases or suffered from severely deteriorating hearing until they reached total deafness. The deafness was bilateral in all cases and lasted for many years before deciding to turn to our department regarding cochlear implant.
Innovation
In May 2011, the World Health Organization's International Agency for Research on Cancer reviewed available scientific evidence on cell phone radiation and brain tumors, classifying mobile phones in the carcinogenic category 2B—possibly carcinogenic to human beings.
The anatomic location of the parotid gland makes its secreted saliva, loaded with cells and macromolecules, an ideal candidate for influence by exposure to mobile phones. This study compared salivary secretion, focusing on oxidative stress indices, flow rate and composition, between mobile phone users and nonusers, and reports a significant increase in all salivary oxidative stress indices in mobile phone users.
Mobile Phone Use and Its Effects on Saliva
Sialometrical analysis
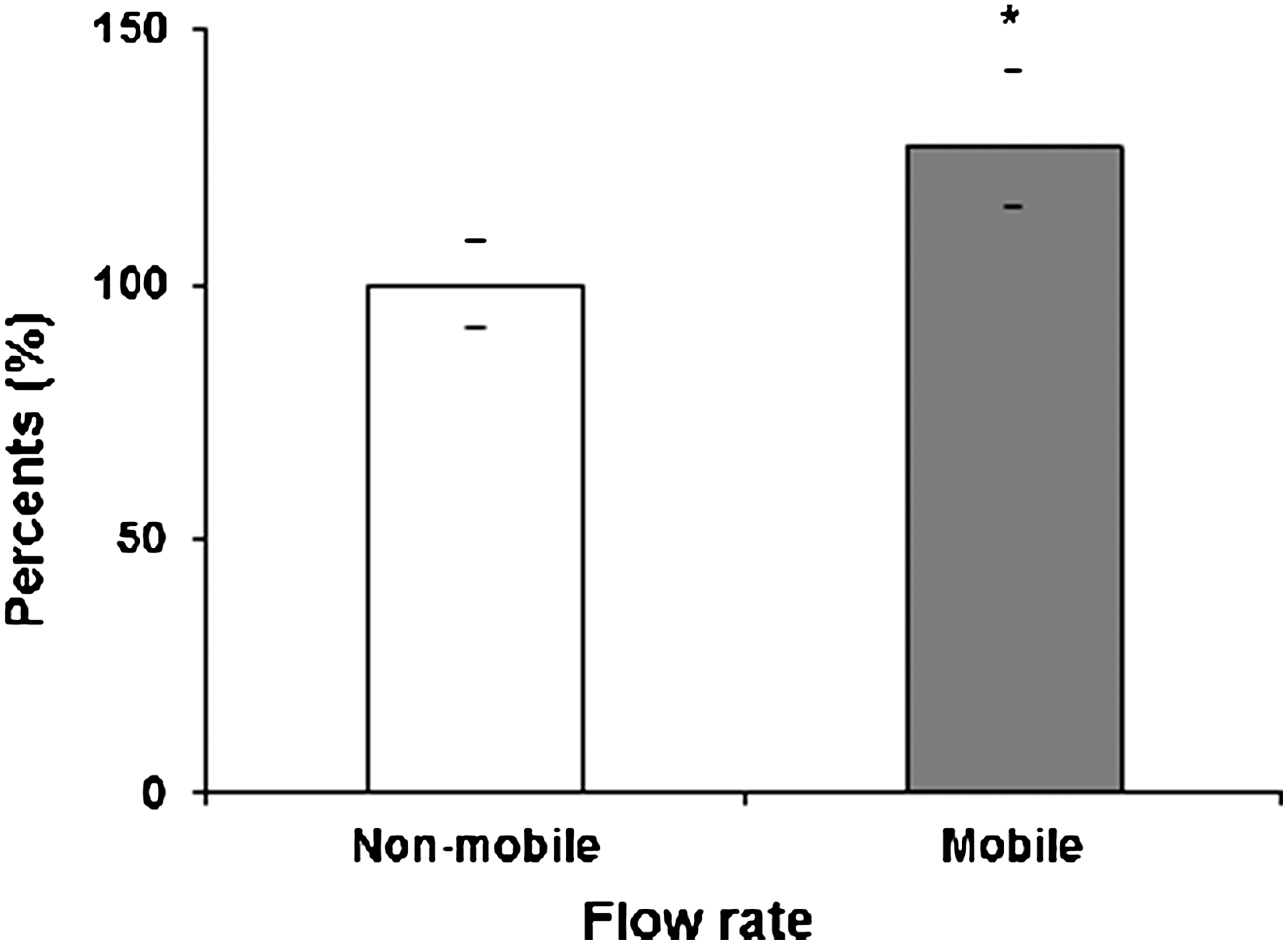
The salivary mean±SEM flow rates in the nonmobile and mobile groups were 0.47 (±0.04) ml/min and 0.6 (±0.09) ml/min, respectively. Hence, the flow rate in the nonmobile group was lower by 21.6% than in the mobile group (p=0.044) (Fig. 1, Table 1).
Difference rate was calculated as the percentage of difference from the mobile group. The results are presented as mean±SEM values.
NS, nonsignificant.
Sialochemical analysis
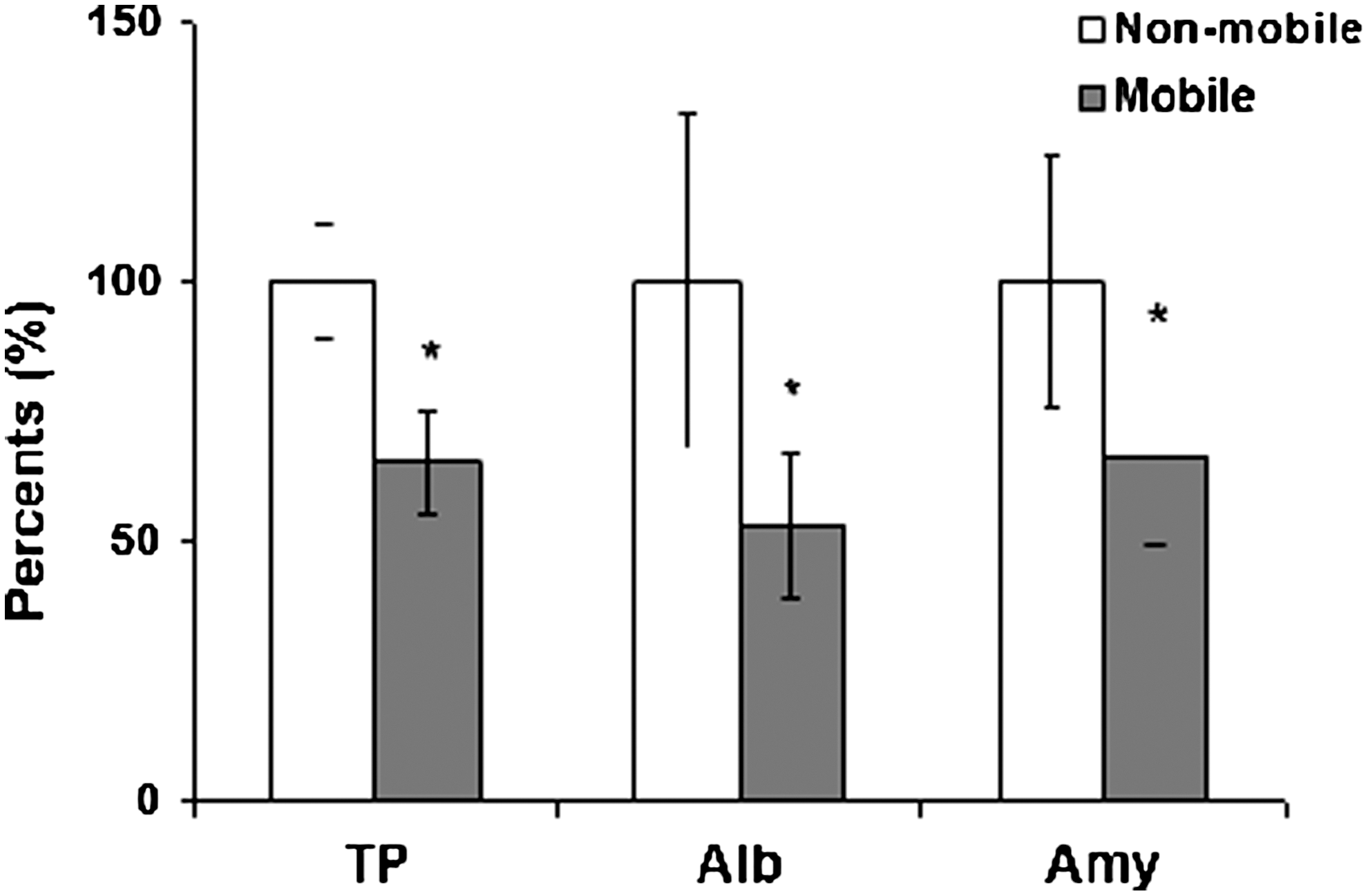
The mean±SEM salivary total protein (TP) levels in the nonmobile and the mobile groups were 144.5 (±16.5) mg/dl and 94.1 (±8.9) mg/dl, respectively; therefore, the TP concentration in the nonmobile group was higher by 53% (p=0.012). The mean±SEM salivary albumin concentrations in the nonmobile and mobile groups were 104.4 (±38.2) mg/dl and 55.2 (±7.6) mg/dl, respectively. Therefore, the albumin level in the nonmobile group was higher by 89% (p=0.032). Similarly, the mean±SEM salivary amylase levels in the nonmobile and the mobile groups were 797.4 (±187.9) U/l and 530.8 (±92.9) U/l, respectively. Hence, the amylase level in the nonmobile group was higher by 50% (p=0.048) (Fig. 2, Table 1). The mean±SEM salivary concentrations of calcium (Ca), magnesium (Mg), and phosphate (P) in the nonmobile group were 4.8 (±0.42) mg/dl, 0.6 (±0.05) mg/dl, and 20.1 (±1.2) mg/dl, respectively, also higher than in the mobile group by 4.3%, 20%, and 9.2%, respectively. These differences however did not reach statistical significance (Table 1).
Salivary oxidative stress indices
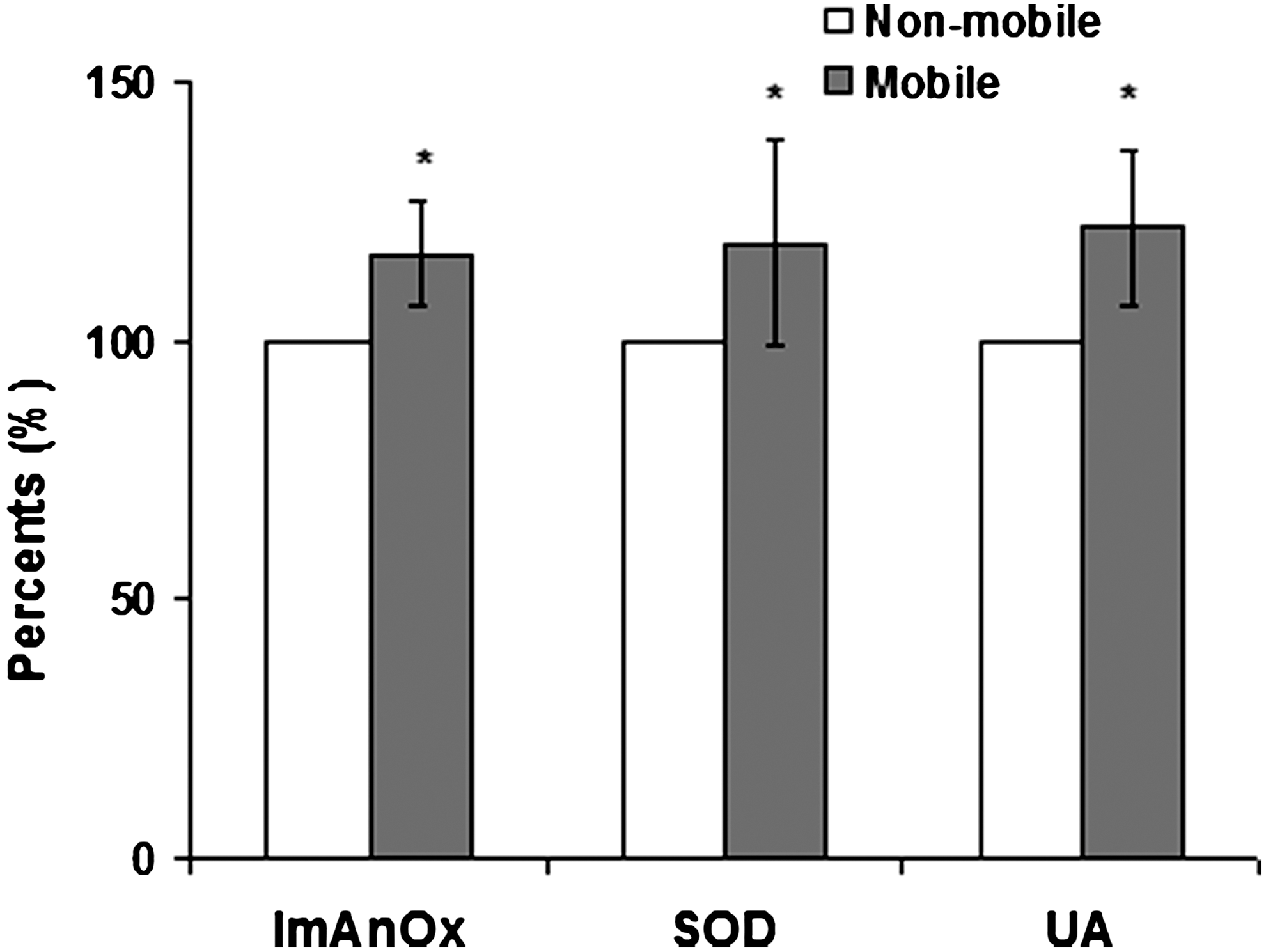
In contrast to the salivary general indices, the salivary oxidative indices were higher in the mobile group when compared with the nonmobile group. The mean±SEM salivary malondialdehyde (MDA) levels in the mobile and nonmobile groups were 23 (±2.9) μM and 5.5 (±1.1) μM, respectively. Hence, the MDA level was 4.18 times higher in the mobile group as compared to the nonmobile group (p=0.0031) (Fig. 3, Table 2). The mean±SEM salivary carbonyl levels in the mobile and nonmobile groups were 0.195 (±2.9) nmol/mg and 0.10 (±2.9) nmol/mg, respectively. Hence, the carbonyl level was higher by 95% in the mobile group as compared to the nonmobile group (p=0.048) (Fig. 4). The salivary ImAnOx, superoxide dismutase (SOD), and uric acid (UA) levels were also higher in the mobile group as compared to the nonmobile group by 19% (p=0.012), 21% (0.044), and 18% (0.042), respectively (Fig. 5).


The results for the 20 mobile phone users and for the 20 nonmobile users are detailed while there is no connection between these two groups of individuals.
Concluding Remarks and Future Directions
Clearly, the two most important results of the current study are the following: (i) The significant, profound increase in salivary MDA and carbonyl levels found in the mobile phone users as compared to the nonusers. The MDA levels increased by 4.18-fold (p=0.0031), indicating the induced oxidative alterations to cell membranes and other fatty macromolecules. However, as soluble fatty acids in saliva are extremely scarce, we conclude that most if not all the oxidative alterations revealed are to the cells. Similarly, the carbonyl levels increased by 95% (p=0.048), indicating the induced oxidative stress to the salivary proteins. Not surprisingly, this outcome was shown to be accompanied by a concomitant rise in the antioxidant salivary systems: ImAnOx, SOD, and UA. SOD and the UA are considered pivotal salivary antioxidants responsible for most of the salivary antioxidant potential (7, 9). (ii) The significant increase of the salivary flow rate in mobile-phone users as opposed to those who do not use mobile phones is not surprising (90% of the nonmobile individuals are deaf ), since mastication is much more developed in hearing people who speak, thus activating their mastication muscles. Noteworthy is the fact that this increase in the flow rate is composed mainly by parotid secretion, which is diluted and watery in nature (serous fluid). It could be postulated that the mastication muscles in the nonmobile individuals are less developed due to their relatively limited use of mastication muscles for speech, as compared to the general population. Several studies have found a correlation between the function and strength of those muscles and the salivary flow rate (5). Moreover, we hypothesized that the relative underuse of the mastication muscles and saliva secretion in the deaf individuals could have led to a form of degeneration of the salivary glands, which in turn would increase the infiltration rate of albumin and other components from the blood stream through the salivary glands and oral mucosa into the saliva. In any case, this observation in deaf people is reported here for the first time (xerostomia was considered one of the exclusion criteria, and therefore did not exist in this group). Furthermore, as the composition of the saliva changes along its pathway in the secretory ducts, the flow rate affects the final concentration of the saliva components. The increase in salivary flow rate is known to have a diluting effect, mostly on salivary macromolecules and to a lesser extent on ions as the ions diffuse relatively easily along with the watery secretion. Indeed, we found that the concentrations of the salivary components examined were lower in the mobile group and more so for the macromolecules: TP, albumin, and amylase.
The major limitation to this study is that, under its current design, one cannot exclude the possibility that deafness itself, and not the lack of being exposed to NIER, is responsible for the observed reduced oxidative stress in the nonmobile group, though this seems unlikely. An association between deafness and oxidative stress and/or with an alteration in salivary composition or flow rate has never been reported in the literature. Furthermore, the opposite trends of the changes in the levels of the examined salivary components versus the salivary oxidative indices and the fact that the reduced levels of all salivary components are expected when the flow rate increases (as in the mobile phone users), further emphasizes the unexpected increase of the salivary oxidative stress indices, which is therefore, most probably explained by the effect of the closely emitted NIER. It is therefore expected that the level of NIER emitted will correlate with the biological impact induced, which in turn depends on the different mobile phone technologies used. The rate at which the human body absorbs NIER is measured by specific absorption rate (SAR). The amount of radiation emitted by mobile phones depends on the model of the handset. Different handsets have different SAR ratings, and different countries have placed radiation exposure limits on the maximum levels of SAR for modern handsets. These limits vary according to the country; for example, in the United States, the Federal Communications Commission has set a maximum SAR limit of 1.6 W/kg, whereas in Europe, this limit is 2.0 W/kg.
As for the demonstrated altered salivary components, our results are supported by Goldwein et al., who collected parotid saliva simultaneously from both glands, and compared salivary secretion between dominant and less-dominant sides of subjects who used mobile phones. They found a lower salivary TP concentration and a higher flow rate in the dominant side (4). Noteworthy also is the study published by Augner et al., who reported that NIER emitted from base stations altered salivary cortisol, immunoglobulin A (IgA), and amylase (1).
In summary, our study indicates that mobile phone users experience considerable oxidative stress on proximal tissue as shown in the saliva, which mostly originates from the parotid glands. Oxidative stress is a potential contributor for the risk for developing cancer, and the currently demonstrated rise in salivary oxidative damage indices may result from an attempt to counteract this risk. Unfortunately, this may not be successful in all cases. Accordingly, perhaps our results can be considered novel evidence for WHO/IARC to reclassify the possible health threat of mobile phones to human beings.
The currently reported results may contribute to influencing the pattern of future mobile phone use, perhaps to the widespread use of earphones or the use of antioxidants, or to developing altered forms of NIER. Finally, we note that salivary analysis is valuable in noninvasively monitoring the human health consequence of the mobile phone use.
Notes
Subjects
This study was conducted in the Department of Otorhinolaryngology, Rabin Medical Center, and the Oral Biochemistry Laboratory of Rambam Medical Center and the Technion Faculty of Medicine. The 20 subjects in the mobile-phone group had a mean duration use of mobile phone of 12.5 years (range 8–15), and a mean use time of 29.6 h per month (range 8–100). There were no statistically significant differences between this group and the nonmobile group regarding sex, age, or cigarette smoking habits between both groups. (Table 3)
Exclusion criteria included usage of hands-free accessories while talking on the mobile phone, less than 8 years, and less than 8 h per month of mobile phone use in the mobile group, and drug or chronic alcohol abuse, systemic chronic diseases, past head and neck trauma or surgery, or complaint of xerostomia for all subjects. With respect to smoking habits, 2/20 of the nonmobile group and 4/20 of the mobile group individuals smoked, and this difference in smoking status of both groups was not statistically significant (Table 3).
All the subjects in the mobile group completed a questionnaire regarding their mobile phone habits. The study protocol was approved by the Ethics Committee of Rabin Medical Center, and written informed consent was obtained from all participants.
Sialometrical analysis
Unstimulated whole-saliva specimens were collected by using the widely accepted procedure previously described. The specimens were collected under resting conditions in a quiet room during morning hours. No oral stimulus was permitted for 90 min before collection. Subjects were asked to collect saliva in their mouths and to spit into a wide test tube for 15 min as previously described (7, 9). Saliva flow rates expressed as the volume of saliva (ml) secreted per min were calculated. After the collection, the specimens were frozen at −70°C for further analysis.
Sialochemical analysis
The sialochemical analysis was performed as previously described and included calcium (Ca), phosphate (P), magnesium (Mg), TP, albumin (Alb), and amylase (Amy). Briefly, the TP and albumin were determined on the Hitachi 911 automated clinical chemistry analyzer (Roche Diagnostics, Mannheim, Germany). Amylase was measured by the Phadebas amylase test (Pharmacia Diagnostics, Uppsala, Sweden) at 37°C using 4,6-ethylidene (G7)-p-nitrophenyl (G1)-α,D-maltoheptaoside as the substrate. The salivary phosphate concentration was measured spectrophotometrically, and calcium and magnesium concentrations were measured by atomic absorption.
Salivary oxidative stress indices
MDA
Salivary levels of MDA (also known as TBARS—thiobarbituric acid-reactive species) were assessed with the use of the Slater–Sawyer method. Briefly, thiobarbituric acid was used during the reaction to assess the level of induced lipid peroxidation, as there is a direct correlation between the two.
Carbonyls
Salivary carbonyl levels were examined with an enzyme-linked immunosorbent assay (ELISA) colorimetric test kit (Biocell Corporation, Papatoetoe, New Zealand), which was used to quantitatively measure carbonyls in saliva samples, according to the manual provided by the manufacturer.
ImAnOx
The antioxidative capacity was determined by the reaction of antioxidants in saliva with a defined amount of exogenously provided hydrogen peroxide (H2O2) using an ELISA colorimetric test system (Immundiagnostik AG, Bensheim, Germany). The antioxidants in the saliva sample eliminated a certain amount of the hydrogen peroxide provided. The residual H2O2 was determined colorimetrically by an enzymatic reaction that involves the conversion of tetramethyl-benzidine (TMB) to a colored product. After the addition of a stop solution, the samples were measured at 450 nm in a microtiter plate reader and quantified by a calibrator. The difference between applied and measured concentration in a defined time is proportional to the reactivity of the antioxidants of the sample (antioxidant capacity).
SOD activity
Total activity of SOD isoenzymes (Cu\Zn-SOD and Mn-SOD) was measured using the Xanthine Oxidase\XTT method. That is a spectrophotometric assay for SOD based on tetrazolium salt 3′–{1-[(phenylamino)-carbonyl]-3,4- tetrazolium}-bis (4-methoxy-6-nitro) benzene sulfonic acid hydrate reduction by xanthine–xanthine oxidase. The method is a modification of the NBT (nitroblue tetrazolium) assay. XTT is reduced by the superoxide anion (O2•) generated by xanthine oxidase. Formazan is read at 470 nm. SOD inhibits this reaction by scavenging the O2•. One unit of the enzyme is defined as the amount of enzyme needed for 50% inhibition of absorption in the absence of the enzyme.
UA concentration
UA concentration was measured with a kit supplied by Sentinel CH (Milano, Italy) as previously described (7, 9). In the assay, UA is transformed by uricase into allantoin and hydrogen peroxide, which under the catalytic influence of peroxidase oxidizes the chromogen (4-aminophenazone/N-ethyl-methylanilin propan sulfonate sodic [ESPT]) to form a red compound whose intensity of color is proportional to the amount of UA present in the sample, and it is read at a wavelength of 546 nm.
Statistical analysis
Data concerning the levels of various indices evaluated in saliva were observed and calculated in nonmobile and mobile subgroups of subjects. For categorical indices, numbers and percentages were calculated. For continuous indices, means, standard error of the mean (SEM), and ranges were calculated. Distributions for categorical variables were compared and analyzed by the Fisher-Irwin exact test. The results of salivary indices between subgroups of patients were compared by Wilcoxon rank-sum test (a nonparametric test) or by two-sample t-test to compare between means (a parametric test). A p-value smaller than 0.05 was regarded as statistically significant.