
Abstract
Cardiac surgery is associated with release of the pleiotropic cytokine macrophage migration inhibitory factor (MIF). The trigger for MIF release has not yet been elucidated. Owing to its intrinsic antioxidative activity, MIF might reduce oxidative stress and protect from myocardial ischemia and reperfusion (I/R) injury.
In the present study, patients scheduled for elective cardiac surgery (n=46) were randomized to undergo coronary artery bypass grafting either conventionally with cardiopulmonary bypass and cardioplegic arrest-induced I/R (cCABG) or in an off-pump procedure (OPCAB) with minimized I/R. We report that only patients who underwent cCABG exhibited a postoperative increase of MIF (p=0.024), while both groups showed an increase in interleukin-6. MIF release appears to be primarily mediated by I/R and to a lesser extent by inflammation. Endogenous peroxidase activity (p=0.021) and serum levels of thioredoxin (p=0.003) were significantly higher in patients who underwent cCABG after surgery. Interestingly, perioperative MIF release was associated with an enhanced antioxidant capacity and a significantly reduced postoperative incidence of atrial fibrillation (p=0.018) and acute kidney injury (p=0.048). The present study highlights the role of MIF increase during cardiac surgery in response to oxidative stress. Based on current observations, we hypothesize that intraoperative MIF secretion is due to I/R and enhances the antioxidant capacity in patients during cardiac surgery. Antioxid. Redox Signal. 19, 231–239.
Introduction
During cardiac surgery, myocardial I/R injury provokes the release of cytotoxic reactive oxygen and nitrogen species (ROS and RNOS). Oxidative stress causes cellular injury that contributes to organ dysfunction. In the past, several investigators reported increased MIF serum levels after cardiac surgery (7). However, neither the trigger nor the significance of perioperative MIF release has yet been understood.
Innovation
Myocardial ischemia and reperfusion (I/R) lead to an excessive release of reactive oxygen species that in cardiac surgery contribute to postoperative organ dysfunction and morbidity. An intraoperative increase of circulating macrophage migration inhibitory factor (MIF) has already previously been demonstrated in patients who underwent cardiac surgery. Despite its critical role in the pathophysiology of various acute and chronic diseases, emerging evidence suggests an overall cardioprotective role for MIF during I/R that is in part mediated by reducing oxidative stress. To our knowledge, the present study is the first clinical trial in humans that indicates MIF's ability to enhance the patient's antioxidant capacity with an impact on organ function.
We postulated that the intraoperative release of MIF during cardiac surgery is mainly due to myocardial I/R and may provide protection from oxidative stress. To test this hypothesis, we assessed both perioperative MIF release and the overall inflammatory response in patients undergoing conventional coronary artery bypass grafting (cCABG), which encompasses cardiopulmonary bypass (CPB) and cardioplegic arrest in comparison with patients undergoing beating-heart off-pump coronary artery bypass grafting (OPCAB), in which myocardial I/R injury is minimized.
Enrolled Patients
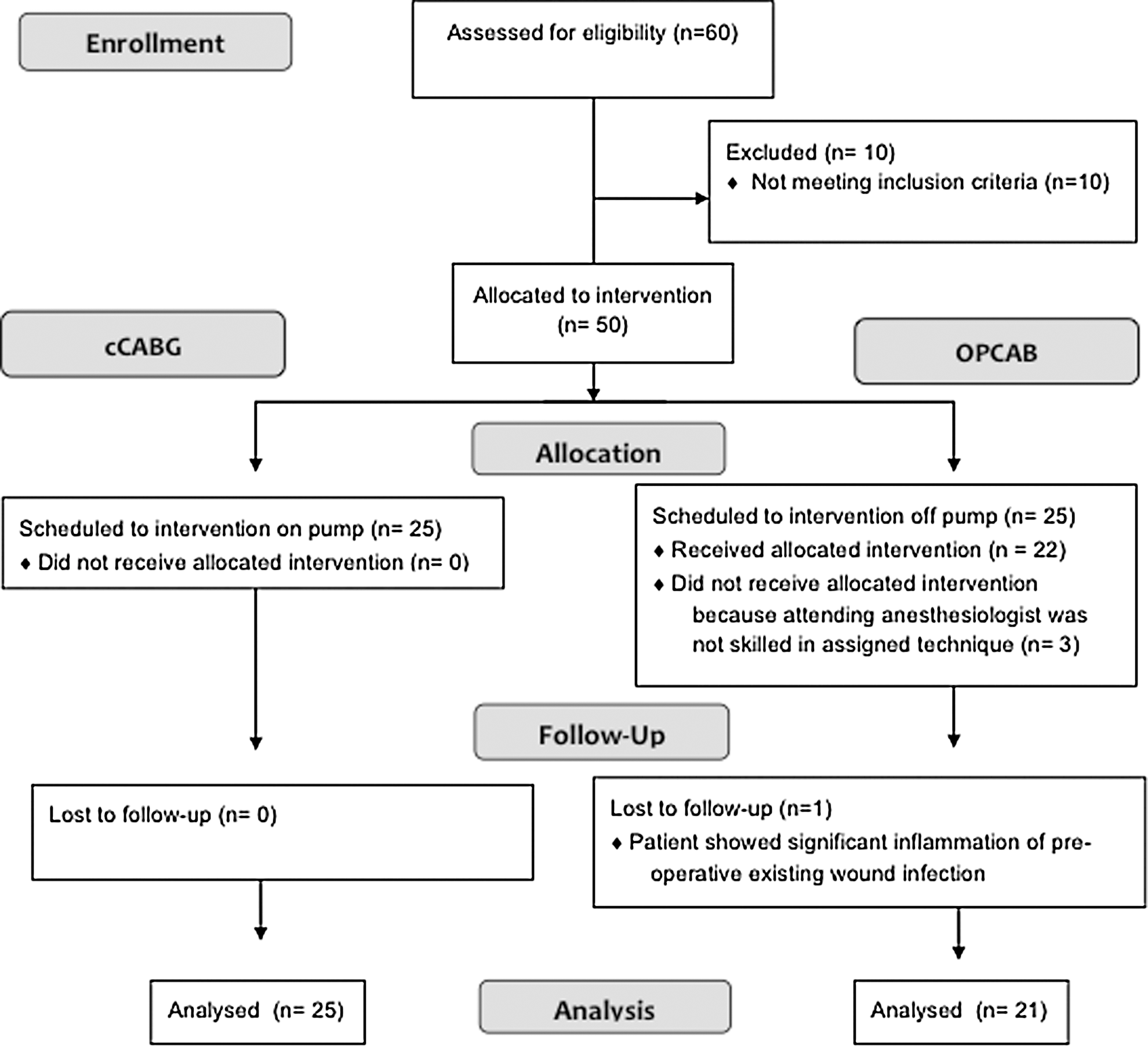
From 60 screened patients, initially, 25 on-pump and 21 off-pump fulfilled the inclusion criteria and were investigated and followed-up until final analysis (Fig. 1). Groups did not differ with respect to baseline and most intraoperative characteristics (Table 1).
Data are presented as median (range) (not normally distributed data), as mean±SD (normally distributed data) or as absolute numbers (with the percentage [%] of the whole).
Bold p-values indicate significant difference (p<0.05) between the groups.
cCABG, conventional coronary artery bypass grafting; OPCAB, off pump coronary artery bypass grafting; CPB, cardiopulmonary bypass; MI, myocardial infarction; PRBC, packed red blood cells; LVEF, left ventricular ejection fraction; n.a., not applicable.
Time Course of MIF Serum Concentrations and Perioperative Inflammation
Before surgery, the majority of patients in both groups already exhibited remarkably increased MIF values in comparison to healthy volunteers (5, 9). Due to its inflammatory characteristics, MIF has been shown to promote the progression of atherosclerosis by activating the proinflammatory atherogenic pathways. Accordingly, elevated MIF levels have been demonstrated in patients with chronic CAD (7, 9). Interestingly, preoperative MIF values significantly correlated with the preoperatively assessed additive euroSCORE I (r 2=0.346; p=0.045), an established predictor of the postoperative mortality rate in cardiac surgery that takes into account cardiovascular and comorbidities. This association between MIF and euroSCORE I confirms observations recently reported by our group (7).
The Trigger for Perioperative MIF Release and Perioperative Inflammation
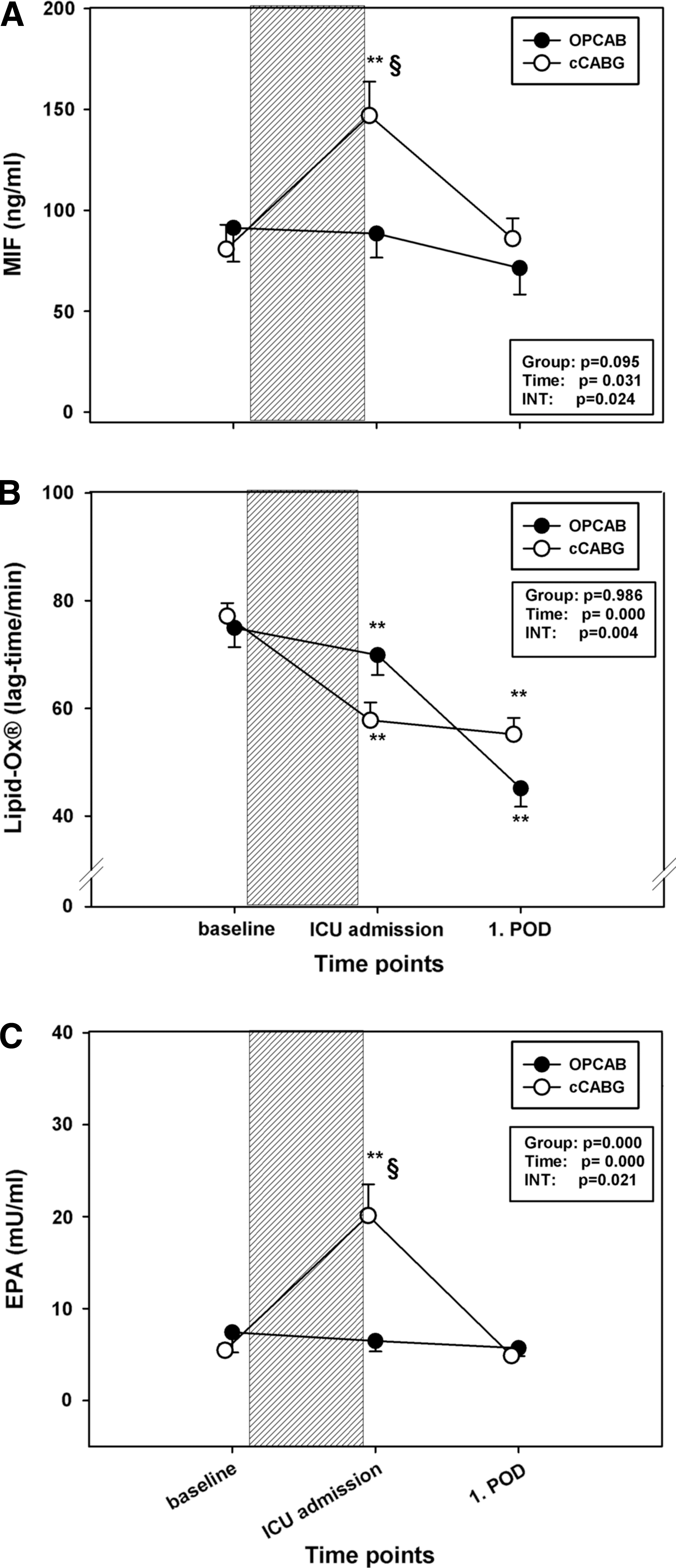
Although several clinical trials repeatedly demonstrated an increase in circulating MIF levels after cardiac surgery (7, 9), the principal trigger/stimulus of the perioperative release of this mediator has not yet been elucidated. MIF may be released from preformed cytoplasmic pools in various immune cells and cardiomyocytes (7, 9) as a response to inflammatory and stress stimuli such as surgical trauma or CPB. Alternatively, the use of cardioplegic arrest and its termination by coronary reperfusion inevitably leads to myocardial I/R, which itself has been demonstrated to be a potent stimulus for MIF release (5, 7). Accordingly, patients who underwent cCABG showed significantly higher circulating MIF levels than patients who underwent OPCAB after termination of surgery (Fig. 2A), and postoperative MIF levels correlated with the myocardial ischemia time (duration of aortic cross-clamping) in patients who underwent cCABG (r 2=0.455; p=0.025). Moreover, the patients who underwent cCABG (with cardioplegic arrest and ischemia) exhibited a significant intraoperative increase of MIF when compared to the patients who underwent OPCAB. In the latter cohort, myocardial ischemia is substantially reduced by avoiding cardioplegic arrest and by the use of intracoronary shunts during the placement of the distal anastomoses. In fact, postoperative CK-MB levels as an indicator for myocardial damage were significantly lower in the OPCAB group. In addition, another observation also clearly points to I/R as the trigger for MIF release rather than an enhanced perioperative proinflammatory state: both groups showed comparable postoperative levels of interleukin (IL)-6 (Fig. 3A) and procalcitonin (PCT) (Fig. 3B). This finding is in accordance with recent investigations demonstrating global surgical trauma to be at least as important for the inflammatory response after cardiac surgery as CPB and contradicting earlier reports that claimed OPCAB surgery to be associated with a lesser proinflammatory response (6). We therefore suggest myocardial I/R to be the major trigger of perioperative MIF release.
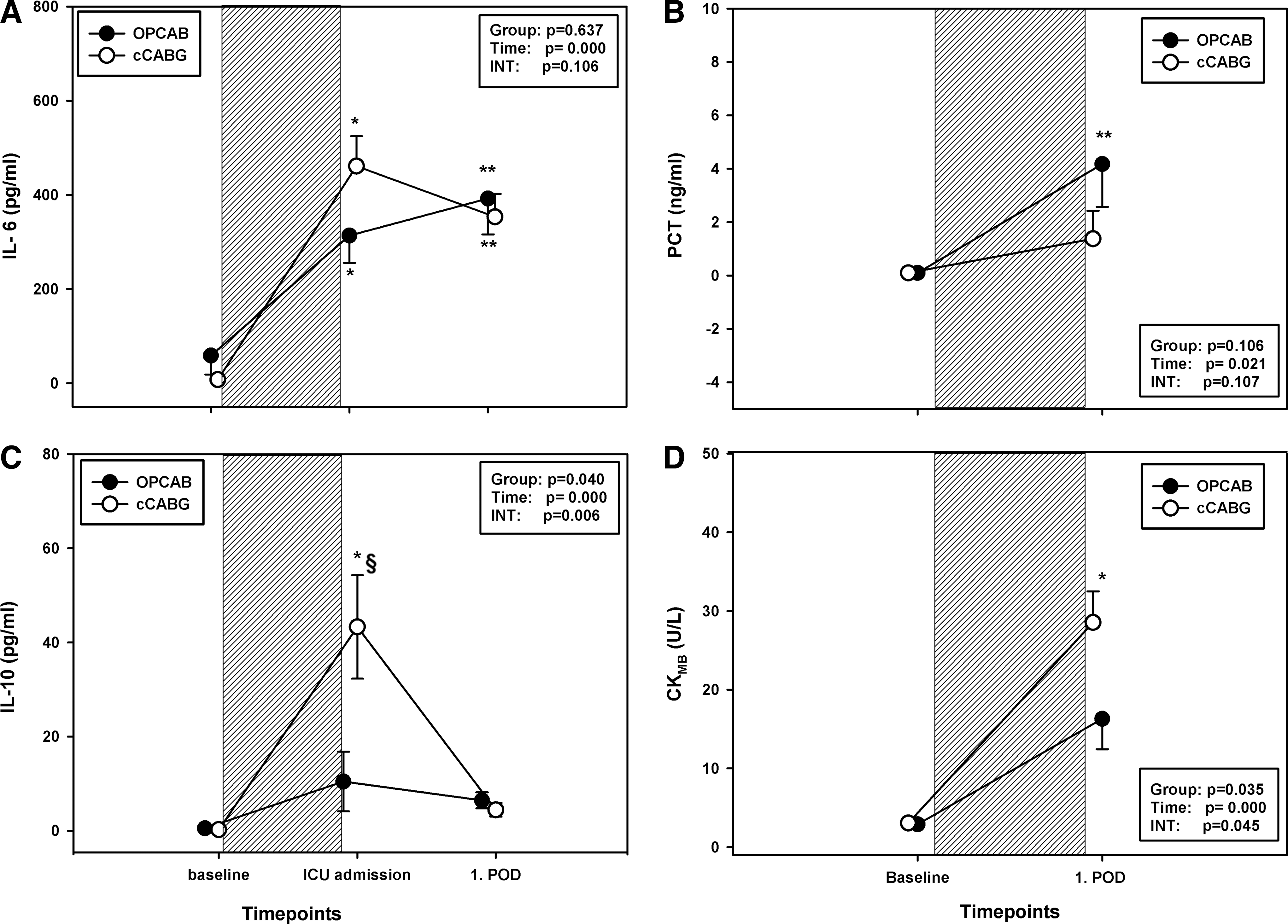
Interestingly, we not only found elevated MIF levels, but also found a significantly higher release of IL-10 in the cCABG group (Fig. 3C). IL-10 generally plays a protective role by suppressing the production of proinflammatory cytokines. Moreover, alterations in the ratio of proinflammatory and anti-inflammatory cytokines leading to a net proinflammatory response have been shown to be associated with vasodilation and myocardial damage after CPB. However, it remains unknown whether the elevated IL-10 levels were the result of an increased MIF release or vice versa or due to other factors, such as cardioplegic arrest or slightly lower intraoperative temperatures in the cCABG group. Together, our findings add further evidence that MIF has cardioprotective properties in humans as recently highlighted (7).
To assess myocardial injury, we measured values of the creatinine kinase isoenzyme CK-MB before and after termination of surgery. Comparison between the groups showed a more extensive myocardial damage in the cCABG group with cardioplegic arrest-induced I/R (Fig. 3D).
Oxidative Stress and MIF's Antioxidant Capacity
In an animal model of myocardial I/R, the hearts of MIF-deficient mice have recently been demonstrated to exhibit significantly higher levels of oxidative stress, resulting in increased mitochondrial injury and larger infarct size in comparison to wild-type hearts (4, 7, 9). In our study, patients who underwent cardiac surgery in both groups demonstrated a significant and comparable increase in oxidative stress as reflected by the intraoperative consumption/decrease of the lipid-soluble antioxidant Lipid-Ox® (Fig. 2B). MIF values at admission to the intensive care unit (ICU) showed a significant correlation to Lipid-Ox® measured on postoperative day (POD) 1 (r 2=0.338; p=0.035). In contrast, only patients in the cCABG group showed a remarkable increase in the total antioxidant capacity as reflected by endogenous peroxidase activity (EPA) (Fig. 2C). EPA was significantly associated with the measured MIF values throughout the whole observation period (Fig. 4), and thus it is tempting to speculate that the increase in endogenous peroxidase activity in the cCABG group might indicate the early initiation of a beneficial process, counter-regulating oxidative stress.

An emerging body of evidence suggests a protective role for MIF during I/R that might be in part mediated by its antioxidant capacity (4). In this context, the intrinsic TPOR activity of MIF has been identified to confer protection against oxidative stress. The MIF sequence contains three Cys residues, which have been found to contribute to several of the functional properties of MIF. Cys-57 and Cys-60 form a CXXC motif that has catalytic TPOR activity in vitro and in cellulo and is a distinct hallmark of the TPOR family of proteins (4, 7).
Thioredoxin or thioredoxin 1 (TRX or TRX1) is a multifunctional protein with anti-inflammatory, antiapototic, and antioxidant properties that is ubiquitously present. Various studies have repeatedly demonstrated a crucial role for TRX1 in the host antioxidant defense, especially in cardiac disorders. Interestingly, previous studies revealed a link between MIF and TRX, suggesting that in the present study, circulating TRX1 levels further underscore MIF's antioxidant capacity (1). In our study, patients who underwent cCABG with increased MIF values also showed significantly elevated TRX1 levels at ICU admission in comparison to the OPCAB group (Fig. 5A). Indeed, these results are in line with previous findings, as the circulating MIF levels significantly correlated with TRX throughout the entire observation period (Fig. 5B).

MIF and Cardioprotection
Atrial fibrillation (AF) has been reported to frequently occur after cardiac surgery. Although most episodes are self-limiting, the occurrence of AF can prolong hospital stay and is recognized as a risk factor for short-term morbidity and decreased long-term survival. While the exact underlying pathophysiological mechanisms for the development of AF are multifactorial, increasing evidence suggests a link between AF and oxidative stress within atrial cardiomyocytes (2).
In our study, patients who underwent cCABG (who suffered from decreased antioxidant capacity) demonstrated a significantly higher incidence of AF than OPCAPB patients (Table 2) who exhibited significantly higher postoperative MIF values (Fig. 2A) and, correspondingly, a higher EPA activity (Fig. 2C). Importantly, we found postoperative MIF values to be predictive for the freedom from postoperative AF in all patients (Fig. 6), while EPA values alone showed only a tendency to predict freedom from AF (p=0.106).

Data are presented as median (range) (not normally distributed data), as mean±SD (normally distributed data) or as absolute numbers (with the percentage [%] of the whole).
Bold p-values indicate significant difference (p<0.05) between the groups.
ICU, intensive care unit.
Both on- and off-pump procedures have repeatedly been shown to be associated with a high incidence of postoperative acute kidney injury (AKI) (8). Underlying pathophysiological mechanisms cannot solely be attributed to harmful effects of CPB. An excessive release of ROS represents one potential mechanism involved in the pathogenesis of cardiac surgery-related AKI (3). The reduced incidence of AKI in the cCABG group (Table 2) with higher perioperative MIF levels and an enhanced antioxidant capacity might suggest a beneficial effect of MIF on renal function after cardiac surgery. Furthermore, MIF values at admission to the ICU showed a significant and inverse correlation with the extent of postoperative organ dysfunction as assessed by the simplified acute physiology score (SAPS) II score on POD1 (r 2=−0.446; p=0.003).
Conclusions and Future Directions
Yet overall, the functional role of MIF in inflammation and infection seems double-edged: An unbalanced MIF release might be associated with organ dysfunction in patients with infectious diseases. In contrast, our observations support recent findings that attributed to MIF an overall cardioprotective role during I/R. To the best of our knowledge, we are the first to reveal an association between I/R-triggered MIF release and antioxidant capacity in patients who underwent cardiac surgery. High postoperative MIF levels were associated with less organ dysfunction that might be mediated by enhanced antioxidative capacity.
Given the emerging evidence suggesting an overall cardioprotective effect of MIF during I/R, it is tempting to speculate that in the future, modulating MIF release may represent a fascinating pharmacological approach for patients with myocardial I/R. Moreover, since MIF is encoded in a functionally polymorphic locus, subjects with low-expression MIF alleles who experience I/R injury may be at increased risk for organ dysfunction. An assessment of MIF expression or the MIF genotype may contribute to improved risk stratification, so that low MIF producers have closer postoperative follow-up.
Notes
Materials and methods
Study design and patients
After approval of the institutional review board (Ethics commission RWTH Aachen) and written informed consent, 46 patients were enrolled in this randomized, prospective, noninterventional study. The trial was registered at ClinicalTrials.gov (NCT number: 01409057).
We included patients that were scheduled for elective CABG surgery. Exclusion criteria were emergency operations, patients in which the OPCAB technique was deemed not feasible by the surgeon, combined procedures involving surgical procedures other than CABG, severe pre-existing renal or hepatic insufficiency, age <18 years, and failure to obtain informed consent. Patients were randomized to cCABG with the use of CPB and cardioplegic arrest or to undergo beating-heart OPCAB by a closed-envelope technique.
Surgical procedure
After midline sternotomy, dissection of the internal mammary artery, and harvesting of the venous conduits, heparin was administered (300 IE kg−1) to obtain an activated clotting time of >400 s.
cCABG: Standard cannulation for CPB was performed with ascending aortic cannulas and dual-stage cannulas within the right atrium. Extracorporeal circulation was performed with a nonpulsatile pump flow of 2.2 L min−1 m−2, and the blood pressure was maintained between 50 and 70 mmHg. Antegrade cardioplegia cannulas were placed. Cardiac arrest was induced by a single and antegrade infusion of cold crystalloid cardioplegic solution (Custodiol™; Köhler Chemie) in the aortic root immediately after cross clamping. Patients' temperatures were either kept warm or allowed to drift to 32°C during CPB.
Distal anastomoses were done in ischemic arrest. After releasing of the aortic cross-clamp, proximal anastomoses were constructed to the ascending aorta during a period of tangential clamping. After the patient was weaned from CPB and de-cannulated, heparin was antagonized with protamine in a ratio of 1:1, and aspirin was administered per os (p.o.) starting 8 h postoperatively.
OPCAB: Patients were placed in the Trendelenburg position and rotated to the right to assist in coronary artery exposure and prevent hemodynamic instability during construction of the distal anastomoses. Commercially available mechanical stabilizers were used to facilitate distal anastomoses. During construction of these anastomoses, an intracoronary shunt was inserted in an attempt to prevent myocardial ischemia. Distal anastomoses were done before proximal anastomoses. The left internal thoracic artery-to-left anterior descending coronary artery anastomosis was constructed first. Proximal coronary anastomoses were performed during a period of tangential clamping of the ascending aorta. After completion of all anastomoses, heparin was antagonized with protamine in a ratio of 1:1, and aspirin was administered p.o. starting 8 h postoperatively.
Anesthesia
All patients received balanced anesthesia according to our institutional routine (6). The evening before surgery, all patients received 1–2 mg lorazepam p.o. and 3.75–7.5 mg midazolam p.o. 1 h before arrival in the operating room. Preoperative medication was continued until the day of surgery, except for metformin, ACE inhibitors, and AT2-receptor antagonists. Anesthesia was induced with etomidate (0.1–0.2 mg kg−1) and sufentanil (0.5–1 μg kg−1). Muscles were relaxed with rocuronium (1 mg kg−1). Anesthesia was maintained with continuous infusion of sufentanil (1 μg kg−1 h−1) and sevoflurane (0.5–1 MAC) throughout the whole procedure. Basic fluid substitution was performed with 1 ml kg−1 h−1 balanced crystalloid solutions. Packed red blood cells were transfused when the hemoglobin content was below 7.5 g dl−1. The administration of additional fluids, vasopressors, or inotropic drugs was left at the discretion of the attending physicians.
Intensive care unit
All patients were transferred to the ICU after termination of surgery. ICU treatment was standardized according to our institutional guidelines. After weaning from ventilation, tracheal extubation was performed when standard extubation criteria were fulfilled. Patients were discharged from the ICU after fulfillment of our standardized discharge criteria and transferred to standard care units.
Data collection
Baseline characteristics and any pre-existing diseases were assessed before surgery and subsequently documented. Clinical-relevant data were documented separately at predefined time points: after induction of anesthesia, after weaning from CPB, at admission to the ICU, and on each further morning during the ICU stay. In addition to the duration of mechanical ventilation, the ICU, and hospital length of stay, we recorded the incidence of systemic inflammatory response syndrome, sepsis, severe sepsis, and septic shock according to the ACCP/SCCM consensus conference criteria. Likewise, we used the following established organ-failure variables to determine the incidence of any organ dysfunction: arterial hypoxemia (PaO2/FiO2<300 mmHg), coagulation abnormalities in the absence of pharmacologic anticoagulation (international normalized ratio [INR]>1.5 or a partial thromboplastin time [PTT]>60 s), hypotension (mean arterial pressure [MAP]<70 mmHg) despite adequate fluid replacement, thrombocytopenia (platelet count <100,000 L−1), hyperbilirubinemia (plasma total bilirubin >2 mg dl−1 or 34.2 μM), and neurological dysfunction (Glasgow Coma Score below 15 in absence of sedation or metabolic impairment). AKI was defined according to the RIFLE criteria: a twofold increase of creatinine or glomerular filtration rate <50% or urine output <0.5 ml kg−1 h−1 for at least 12 h.
To quantify the extent of organ dysfunction, we assessed the SAPS II on the 1st POD. Subsequently, the sequential organ failure assessment was determined for the daily assessment of organ dysfunction throughout the ICU stay.
Laboratory assessment
Serum samples were drawn after induction of anesthesia, after admission of the patients to the ICU, and on POD1. All blood samples were immediately centrifuged (3000 rpm, 10 min), and the supernatant was then transferred into cryotubes. Subsequently, the serum samples were stored at −80°C until final analysis.
Cytokines: Serum levels of PCT, IL-6, and IL-10 were measured to assess the perioperative inflammatory response. PCT and IL-10 were measured as a part of the clinical routine practice using a fully automated chemiluminescence analyzer (PCT; Liaison, Byk Sangtec Diagnostica; IL-10; IMMULITE, Siemens Healthcare Diagnostics GmbH). The myocard-specific creatine kinase isoenzyme (CK-MB) was analyzed automatically by a centrifugal analyzer (Cobas 8000; Roche). Serum concentrations of IL-6 were determined with a commercially available enzyme-linked immunosorbent assay (ELISA) (IL-6; R&D Systems) according to the manufacturer's instructions. Serum levels of MIF were assessed using an ELISA technique as previously described (6), using capture antibody MAB289 and detection antibody BAF289 (R&D Systems).
Markers of antioxidant capacity: The circulating plasma levels of human (TRX1) were determined using standardized ELISA kits (Human TRX1; LabFrontier Co., Ltd.). The EPA in serum was determined by the reaction of endogenous peroxidases with hydrogen peroxide, using 3,5,3′,5′-tetramethylbenzidine (TMB) as the chromogenic substrate (EPA®; Omnignostica GmbH). Serum peroxidase activity was calculated in relation to the horseradish peroxidase standard curve. Results were expressed as mU/ml. The lag-time of ex vivo degradation of the fluorophore1-palmitoyl-2-((2-(4-(6-phenyl-trans-1,3,5-hexatrienyl)phenyl)ethyl)-carbonyl)-sn-glycero-3-phosphocholine (DPHPC) by ROS in serum was determined with a fluorescent diagnostic assay, which is a biomarker for the specific determination of lipid-soluble antioxidants (Lipid-Ox®; Omnignostica GmbH). Briefly, 100 μL serum was incubated with 2 nMol DPHPC and kept under argon at 37°C for 12 h. Oxidation was started via a peroxide (0.004%)–peroxidase (10 U/ml) reaction, and the time-dependent decrease in fluorescence intensity at 430 nm (excitation at 360 nm) was monitored on a FluoStarfluorometer (BMG Lab-Technologies). Results were expressed as lag-time in minutes.
Statistical analysis
All data were statistically analyzed using a commercially available software package (SPSS 19.0; SPSS, Inc.).
As a primary endpoint, we determined perioperative MIF release and compared patients who underwent surgery with I/R due to cardioplegic arrest with patients who received a beating-heart procedure without extracorporeal circulation and cardioplegic arrest.
The sample size was calculated based on previous observations in which we found MIF to show a nearly 100% increase at admission to the ICU (6). We hypothesized that this MIF increase would only occur in the patients who underwent cCABG. Power analysis revealed a minimal sample size of 21 patients per group to detect a 90% effect for MIF at admission to the ICU, when a level of significance of 0.05 and a power of 90% were to be achieved.
Secondary endpoints were clinically relevant outcome parameters consisting of SAPS II, the duration of mechanical ventilation, the hospital and ICU length of stay, the degree of perioperative inflammation (as assessed by serum levels of PCT, IL-6, and IL-10), and the perioperative redox homeostasis as assessed by oxidative biomarkers. We predefined an observation period of 1 day that adequately reflects the period that is most interesting for the assessment of I/R.
All data were tested for normal distribution using the Shapiro-Wilk-W test. Normally distributed results of single measurements were compared between the groups using the Student's t-test. Results of repeated measurements were compared using a repeated-measurement analysis of variance to take into account the correlated observations within the groups, with the within-factor time, and the grouping factor treatment (on-pump vs. off-pump). Receiver-operating characteristic curves were constructed, and the area under the curve (AUC) was calculated to determine the optimal sensitivity and specificity of circulating MIF values for predicting freedom from AF. Nonparametric data were compared using the Wilcoxon signed-rank test. In case of significant results, post hoc testing was performed using the Bonferroni test and (for not normally distributed data) the Wilcoxon signed rank test with the Bonferroni adjustment for multiple measurements, respectively.
Given the explorative character of our study, the significance level of the fixed-effect results was not adjusted for multiple hypotheses (i.e., for all cytokines and marker of oxidative stress tested in this investigation).
Proportions were compared using the Chi-square test. For correlation studies, linear regression analysis was used. In all cases, a level of p<0.05 was considered statistically significant.
Footnotes
Acknowledgments
We are indebted to the laboratory staff of the Institute of Biochemistry and Molecular Cell Biology (RWTH Aachen University Hospital) for excellent scientific and technical assistance, as well as the patients who participated in this trial.
This study was supported by the Deutsche Forschungsgemeinschaft (DFG) grants Be1977/4-2 (TP1 of DFG-FOR809), GRK1508/1 (project P13), and Ra969/6-1 to J.B., and by the Rotation and START Program of the Faculty of Medicine of the RWTH Aachen University to C.S.