
Abstract
The extracellular superoxide dismutase (SOD3, EC-SOD) enzyme is a major extracellular scavenger of the superoxide anion, a free radical with the potential to cause oxidative damage. Previously, R213G heterozygosity has been associated with a decreased risk of chronic obstructive pulmonary disease (COPD) and an increased risk of ischemic heart disease (IHD). We questioned whether SOD3 R213G homozygosity (213GG) influences morbidity, mortality, and lung function. We found 14 R213G homozygotes (213GG) among 95,871 individuals (1/7000) from the Copenhagen General Population Study and the Copenhagen City Heart Study. The hazard ratio for homozygotes versus noncarriers (NC) (213RR) was 2.8 (95% confidence interval: 1.2–6.8, p = 0.02) for IHD, 1.8 (0.7–4.8, p = 0.25) for any form of cancer, and 2.3 (0.9–6.2, p = 0.10) for all-cause mortality. R213G heterozygosity was not associated with morbidity or mortality. Among never-smokers, we found a 20% lower forced expiratory volume in 1 s (FEV1)% predicted (p = 0.003), a 16% lower FVC% predicted (p = 0.01), and a 7% lower FEV1/FVC ratio (p = 0.02) in R213G homozygotes compared to NC. Our results lead to the hypotheses that the SOD3 enzyme plays a role in cardiovascular disease and in impairing and maintaining lung function in never-smokers. However, our findings should be retested in larger studies and in nonsmoking COPD patient cohorts. Antioxid. Redox Signal. 24, 884–891.
Introduction
T
Previously, R213G heterozygosity has been associated with a decreased risk of chronic obstructive pulmonary disease and an increased risk of ischemic heart disease (IHD). However, no information currently exists on the association between the rare R213G homozygosity and morbidity, mortality, and lung function. We extended this research area by studying for the first time 14 R213G homozygotes and found a 2.8-fold increased risk of IHD and a lower lung function in never-smokers. Our findings support a role of the superoxide dismutase 3 enzyme in cardiovascular disease and in maintaining lung function in never-smokers.
A missense mutation in exon 3 of the SOD3 gene leads to an arginine to glycine substitution at position 213 (R213G), the central part of the extracellular-binding domain. For the tissue-bound form of the enzyme, this leads to decreased heparan sulfate affinity with unaltered enzymatic activity. Consequently, R213G heterozygotes (213RG), which comprise 2.2–6% of the population, have up to 10-fold higher plasma levels of SOD3 compared to noncarriers (NC) (213RR) (4, 5). The rare R213G homozygotes (213GG) have up to 30-fold higher plasma SOD3 levels with severe tissue depletion, especially in lung and vascular tissue (5). Previously, R213G heterozygosity has been associated with a decreased risk of chronic obstructive pulmonary disease (COPD) and an increased risk of ischemic heart disease (IHD) (5, 6).
Thus, studying R213G homozygotes provides for a unique opportunity to investigate the in vivo consequences of reduced tissue defenses against oxidative stress. In the present study, we tested the hypothesis that SOD3 R213G homozygosity influences morbidity, mortality, and lung function in 14 homozygotes from among 95,871 individuals from the Danish general population.
Results and Discussion
Distribution of the R213G genotype and participant characteristics
Among the 95,871 individuals from the combined Copenhagen General Population Study (CGPS) and Copenhagen City Heart Study (CCHS), rs1799895 (R213G) genotype frequencies were 97.5% for C/C NC (213RR), 2.4% for C/G heterozygotes (213RG), and 0.01% (n = 14) for G/G homozygotes (213GG). The genotype distribution was in the Hardy–Weinberg equilibrium (p = 0.88). Baseline characteristics did not differ according to R213G genotype (Table 1); however, as previously shown, plasma EC-SOD was ninefold higher in heterozygotes and 29-fold higher in homozygotes, compared to NC in the CCHS (5).
Continuous variables are summarized as median and interquartile range.
p Values were calculated using Cuzick's nonparametric trend test.
Summarized for current smokers only, not the whole population.
Previously published data from Juul et al. in which SOD3 plasma levels had been measured in a subgroup of 2192 NC, 201 heterozygotes and two homozygotes from the CCHS (5).
CCHS, Copenhagen City Heart Study; CGPS, Copenhagen General Population Study; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NC, noncarriers; SOD3, superoxide dismutase 3.
R213G genotype and risk of cardiovascular disease
To evaluate if the R213G heterozygotes and homozygotes associated with a higher risk of cardiovascular disease, cancer, and mortality, we conducted Cox proportional hazards regression analyses. For IHD, we found a hazard ratio (HR) of 2.8 (1.2–6.8) for R213G homozygotes compared to NC (Table 2), with similar results after accounting for competing risk of death (subhazard ratio [SHR] 2.9 (1.2–7.3), p = 0.02 for homozygotes versus NC, Fig. 1). Estimates were similar for myocardial infarction and ischemic stroke, although the confidence interval for the latter two overlapped 1.0 (Table 2). Heterozygotes did not differ from NC for these endpoints. Finally, for all-cause mortality and cancer, we found no association with R213G genotypes.

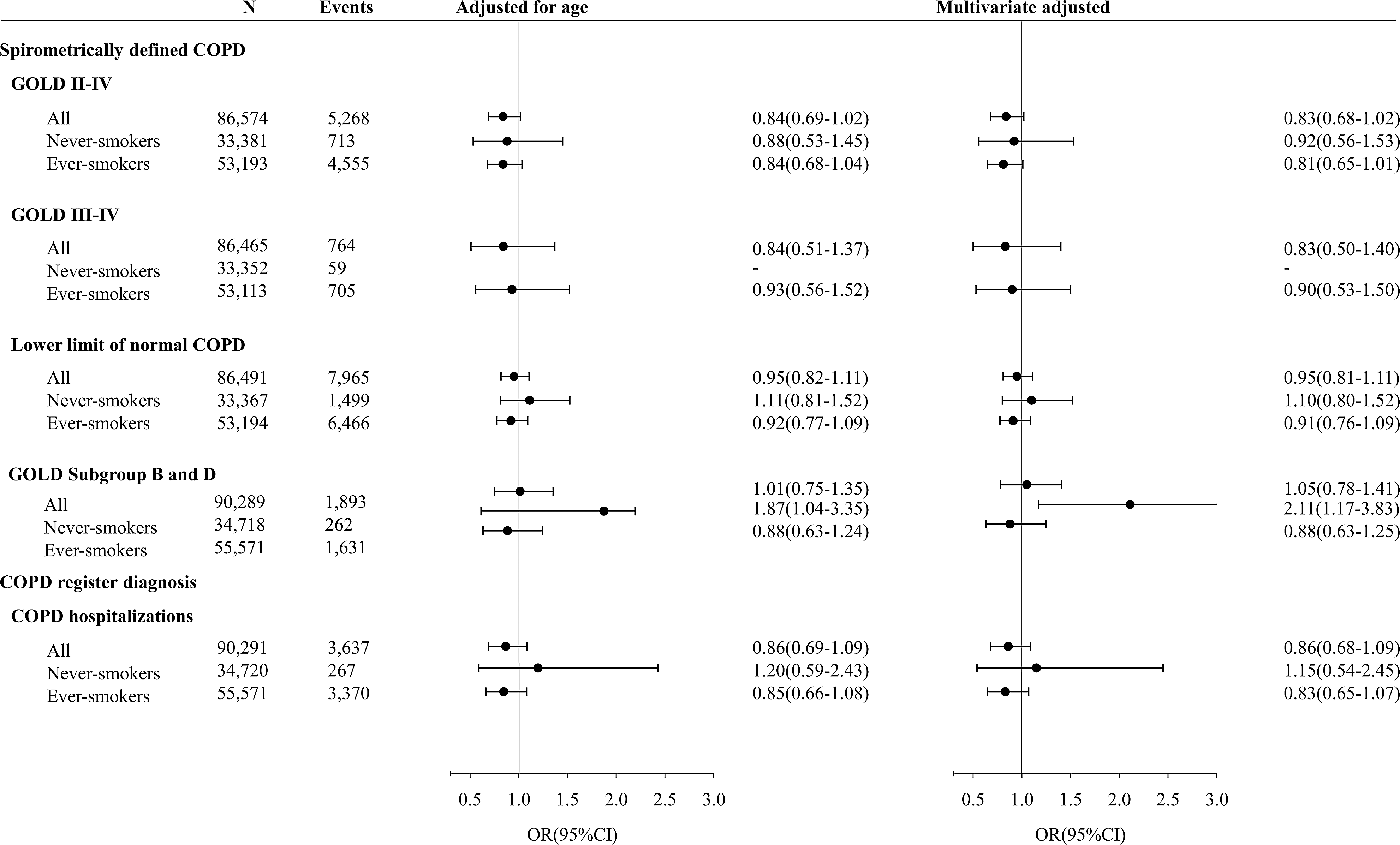
Nonmelanoma skin cancer excluded. HR from Cox proportional hazards regression. All estimates adjusted for age. Self-reported asthma was excluded from analyses of COPD hospitalizations.
CI, confidence intervals; COPD, chronic obstructive pulmonary disease; HR, hazard ratio.
Several conceivable mechanisms could explain the association between R213G homozygosity and IHD. First, by catalyzing the dismutation of the superoxide anion to hydrogen peroxide, SOD3 prevents the superoxide anion from reacting with nitric oxide and, thus, protects the biological activity of nitric oxide as it transverses the interstitial space to mediate endothelial-dependent vasodilation and inhibition of vascular smooth muscle cell proliferation (2). By preserving nitric oxide, SOD3 could play a role in preventing endothelial dysfunction, a possible early step in the atherosclerotic process (2). Furthermore, tissue deficient of SOD3 likely has higher levels of superoxide anions, which could, through the formation of reactive oxygen species, lead to more low-density lipoprotein (LDL) oxidation, which increase LDL uptake by macrophages, leading to foam cell formation, a constituent of the atherosclerotic plaque (8). In mice, R213G homozygosity has been shown to shift the distribution of SOD3 from lung and vascular tissue to extracellular fluids such as plasma and lung epithelial lining fluid, with a marked depletion of SOD3 in the wall of blood vessels and increased vascular wall remodeling (4).
The question of whether the depletion of SOD3 in blood vessel walls of R213G homozygotes leaves the vascular tissue more subject to endothelial dysfunction and plaque formation and hereby to a higher risk of IHD, as found in this study, warrants further investigations.
Previously, R213G heterozygosity has been associated with an increased risk of IHD in the CCHS (5). However, we could not recapture these associations in this expanded study with an additional 14 years of follow-up and including an additional 87,030 individuals from the CGPS. Since heterozygotes have up to 10-fold higher plasma levels of SOD3 than NC, we would expect to find an effect; nevertheless, the fact that we did not could suggest a recessive effect of the R213G variant and that the former finding represented a chance finding.
R213G genotype, lung function, and COPD
Lung function did not differ by R213G genotype among ever-smokers and never-smokers combined; however, we found a 20% lower forced expiratory volume in 1 s (FEV1) in percent of predicted (p = 0.003), a 16% lower forced vital capacity (FVC) in percent of predicted (p = 0.01), and a 7% lower FEV1/FVC (p = 0.02) among homozygotes compared to NC in never-smokers (Fig. 2 and Table 3). Furthermore, we included the α1-antitrypsin genotype Z, associated with reduced lung function among smokers and an established genetic risk factor for COPD, as a positive control for effect of genotype on lung function and found among α1-antitrypsin ZZ homozygotes a similar effect size on FEV1% predicted, FVC% predicted, and FEV1/FVC in ever-smokers as that observed for SOD3 R213G homozygosity in never-smokers (Figs. 2 and 3). SOD3 R213G heterozygotes did not differ from NC with respect to spirometry values (Fig. 2). R213G heterozygotes did not differ from NC (213RR) with respect to COPD hospitalizations and spirometrically defined COPD (Table 2 and Fig. 4) overall, or stratified by smoking status. The two COPD endpoints were with no and only a single event, respectively, among R213G homozygotes, impeding further analyses.


Allergy: asthma, hay fever, or eczema. Any respiratory symptoms: wheezing, any dyspnea, sputum, or cough. Sputum: for more than 3 months a year. Cough: in relation to strain. Continuous variables are mean and standard deviation.
p from SOD3 R213G homozygotes (213GG) versus heterozygotes and NC combined (213RG +213RR) in never-smokers.
p from SOD3 homozygote never-smokers versus A1AT ZZ homozygote ever-smokers. For categorical variables, p is from Fischer's exact test, for continuous variables, p is from Kruskal–Wallis test.
A1AT, α1-antitrypsin Z genotype (rs28929474); He, heterozygotes; Ho, homozygotes; mMRC, modified Medical Research Council; NC, noncarriers.
We examined the clinical characteristics of the SOD3 R213G homozygote never-smokers and compared them to never-smoking R213G heterozygotes/NC (213RR+RG). We found that 80% (4/5 homozygotes) reported dyspnea compared to only 27% of heterozygotes/NC (p = 0.02 from Fischer's exact test) (Table 3). Overall, the clinical characteristics of the α1-antitrypsin ZZ homozygote smokers were comparable to the SOD3 homozygote never-smokers.
Based on these findings, we hypothesize that the enzyme may play a role in preventing inflammatory pulmonary disease and R213G homozygotes may be more vulnerable to oxidative lung injury. Possibly, the lack of association between the genotype and lung function among former and current smokers could be ascribed to the damaging effects of smoking on lung tissue, far exceeding the damaging effects of the R213G variant, making the effect of the variant immeasurable. In contrast, it is also possible that the displacement of the SOD3 enzyme from the lung tissue to the epithelial lining fluid plays a different role among individuals exposed to tobacco than among never-smokers; the detrimental effects of low tissue levels of the enzyme could be balanced out by beneficial effects of high enzyme levels in the lung epithelial lining fluid among those exposed to excessive inhaled oxidants.
Previously, R213G heterozygosity has been associated with a decreased risk of COPD (6), which we could not recapture in this study. Possibly, this previous association was a chance finding or perhaps the lack of association in this study is due to changes in smoking habits, asthma self-reporting, or general lifestyle changes over time. To our knowledge, the effect of R213G homozygosity on lung function has not previously been examined. Due to the rarity of the homozygotes, previous studies have only included R213G heterozygotes, and overall, the studies found no difference in lung function by R213G genotype. However, the similarities of the α1-antitrypsin ZZ homozygotes and the SOD3 R213G homozygotes for effect sizes of lower lung function in ever-smokers and never-smokers, respectively, in our study could suggest an effect of R213G of similar size as that of α1-antitrypsin ZZ on lung function. Thus, SOD3 R213G homozygosity could be the (rare) cause of clinical respiratory disease among never-smokers, and our finding should be retested, preferably in nonsmoking COPD patient cohorts.
Limitations and conclusion
Potential limitations to our study should be considered. All participants were of Danish descent, and thus, our results may not necessarily apply to other ethnicities; however, this also minimizes the risk of population stratification. Also, inherently any investigation of R213G homozygotes will be difficult due to the low numbers in the general population. Thus, we naturally cannot rule out that the observed findings could represent chance; hence, the need for replication in larger studies.
In conclusion, we observed a higher risk of IHD among SOD3 R213G homozygotes than among NC. Furthermore, we found a lower lung function in R213G homozygote never-smokers compared to NC. Our results lead to the hypothesis that the SOD3 enzyme plays a role in cardiovascular disease and in impairing and maintaining lung function in never-smokers. However, our findings should be retested in larger studies and in nonsmoking COPD patient cohorts.
Notes
Study population
We used the CGPS, initiated in 2003 with ongoing enrollment, and the CCHS, initiated in 1976–1978 with follow-up examinations in 1981–1983, 1991–1994, and 2001–2003. DNA was available in the CGPS and in the 1991–1994 and 2001–2003 examinations of the CCHS. For both studies, individuals aged 20–100 years were invited randomly from the Danish Civil Registration System to reflect the Danish general population. The participation rate was 45% in the CGPS and 61% and 50% in the CCHS 1991–1994 and 2001–2003 examinations. The study was approved by Herlev Hospital and Danish Ethics Committees, and conducted according to the Declaration of Helsinki. Written informed consent was obtained from all participants. No subject was lost to follow-up. We only included white individuals of Danish descent with DNA available, a total of 87,030 individuals for the CGPS and 8841 from the CCHS.
Outcomes
Information on diagnosis of IHD (World Health Organization International Classification of Disease, Eighth Revision (ICD8) codes 410–414, and Tenth Revision (ICD10) codes I20–I25), myocardial infarction (ICD8: 410, ICD10: I21–I22), ischemic stroke (ICD8: 433–434, ICD10: I63), and COPD (ICD8: 491–492, ICD10: J41–J44) was collected from 1977 through April 2013 from the national Danish Patient Registry and the national Danish Causes of Death Registry. Information on diagnosis of invasive cancers from 1943 until November 2011 was obtained from the Danish Cancer Registry, which identifies 98% of cancer cases in Denmark (9). Any cancer was with nonmelanoma skin cancer excluded. The date of death was obtained from the Danish Civil Registration System. For all COPD analyses, individuals with self-reported asthma were excluded (n = 5802). We defined spirometric diagnosis of COPD either according to the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) criteria: GOLD II–IV was defined as the presence of FEV1/ FVC <0.7 and FEV1 <80% predicted and GOLD III-IV as FEV1/FVC <0.7 and FEV1 <50% predicted, or using the lower limit of normal LLN definition for FEV1/FVC calculated as the difference between the predicted value and 1.645 times the standard error of the estimate separately for men and women, as done previously (1). We further stratified COPD into categories GOLD A through D, based on Gold grade and dyspnea as previously described (7), where dyspnea was assessed by questions from the modified Medical Research Council (mMRC) Questionnaire for Assessing the Severity of Breathlessness.
Spirometry and lung symptoms
FEV1 and FVC were measured as described (1). Algorithms for calculation of FEV1% predicted were made using multiple regression with age and height as covariates on a subsample of never-smokers for men and women separately, as previously described (1). We had genotype information and spirometry data on 91,782 participants for the R213G genotype and on 91,486 participants for the alpha1-antitrypsin Z genotype. Symptoms were self-reported and any dyspnea was any report of breathlessness. Cough in response to exertion and sputum, defined as sputum production for at least 3 months per year, was self-reported. Any respiratory symptoms were the composite of wheezing, any dyspnea, sputum, and/or cough.
Covariates
Baseline characteristics were recorded from a self-administered questionnaire, a physical examination, and from blood samples. Participants reported on exposure to occupational dust or fumes and on smoking status (never, former, current), and if relevant number of years of smoking and daily tobacco consumption, from which cumulative tobacco consumption in pack-years was calculated; a pack-year was 20 cigarettes or equivalent smoked per day for 1 year. Ever-smokers were defined as those reporting current or former smoking. Self-reported weekly alcohol intake was in units of ∼12 g of alcohol. Furthermore, information on weekly physical activity (highest vs. lowest half of physical activity groups) and level of income (highest third vs. lowest two-thirds) was obtained from the questionnaire. Systolic blood pressure was measured. Body–mass index was calculated from measured weight in kilograms divided by measured height in meters squared. The data were >99% complete and missing values for covariates were imputed according to age and sex for multivariable adjustment to obtain a complete data set; however, if individuals with any missing data were excluded, results were similar to those presented.
Laboratory analyses
In the CGPS, we genotyped 87,030 individuals for the SOD3 rs1799895 R213G variant, using a TaqMan-based assay (Applied Biosystems) and TaqMan GenoTyper v1 · 2 with a call rate of 99.3%. We used DNA extracted from leukocytes in peripheral blood using the Qiagen blood kit for DNA extraction. Genotypes were assigned in smaller batches, each containing around 5500 individuals. In the CCHS, 8841 individuals had been genotyped previously using polymerase chain reaction followed by restriction enzyme digestion and agarose gel electrophoresis, and all R213G carriers had been reanalyzed and confirmed by DNA sequencing (5). We used the R213G heterozygotes (213RG) and homozygotes (213GG) previously identified by RFLP and DNA sequencing as controls for the TaqMan-based assay. We included the alpha1-antitrypsin Z variant rs28929474 as a positive control on 87,019 and 8069 individuals from the CGPS and CCHS, which had already been genotyped in our laboratory for other projects, also using a TaqMan-based assay. Plasma concentrations of C-reactive protein, triglycerides, LDL cholesterol, and high-density lipoprotein cholesterol were measured with standard hospital assays. Plasma SOD3 had been measured using ELISA and results have been reported previously (5).
Statistical analyses
We used Stata v.13.1. A chi-square test evaluated Hardy–Weinberg equilibrium. p-Values for trends were estimated using Cuzick's nonparametric trend test and the Kruskal–Wallis test was used when comparing two samples. Fischer's exact test was used to compare categorical data when less than five individuals were expected in one group.
To examine the association between SOD3 R213G genotype and cardiovascular disease, cancer, COPD, and mortality, we used Cox proportional hazards regression models to estimate HRs with 95% CIs. We surveyed for morbidity from January 1977 (start of the Danish Patient Registry) until the latest update of diagnosis at April 1, 2013, with a median follow-up time of 36 years, and used all endpoints. For mortality, we surveyed from date of examination until April 1, 2013, with a median follow-up time of 5 years. Because all measured confounders were evenly distributed between genotypes, we adjusted only for age. However, adjusting also for sex gave similar results. Those dying or emigrating (n = 292) during follow-up were censored at their death or emigration dates, respectively. Test for proportionality of hazards over time was performed using graphical methods and residuals; no major violations were observed. We estimated cumulative incidence of IHD with the method of Fine and Gray and calculated an SHR for IHD, accounting for the competing risk of death, by using competing-risks survival regression.
We used a kernel-weighted local polynomial smoother to graph percentiles of FEV1 as a function of age in the two large populations of never-smokers and ever-smokers separately. We used logistic regression to estimate odds ratios with 95% CIs for spirometrically defined COPD adjusted only for age or multivariable adjusted for sex, age, and exposure to occupational dust or fumes.
Footnotes
Author Contributions
C.J.K., S.A., and B.G.N. designed the study, C.J.K. analyzed data, C.J.K., S.A., and B.G.N. interpreted data and wrote the article. All the authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.