
Abstract
The monitoring of progression in amyotrophic lateral sclerosis (ALS) relies on clinical outcome measures that take months to interpret, such as revised ALS functional rating scale (ALSFRS-R) score, with no approved biomarkers. A number of clinical studies have documented the involvement of oxidative stress in ALS pathology. Pertinent to this, we propose to evaluate oxidation–reduction potential (ORP) of cerebrospinal fluid (CSF) as a potential indicator of ALS progression. The case–control study included 24 patients with neurological non-neurodegenerative disorders (controls) and 82 ALS patients with different degrees of disease (ALSFRS-R score: 21–47). ORP was significantly higher in ALS patients than controls. It was not dependent on age or gender. A strong negative correlation was found between ORP and ALSFRS-R score for all patients and patients with spinal onset. In other words, ORP increased with ALS progression. No correlation was found for the subset of patients with bulbar onset, most likely because of the physical distance between neurodegenerative loci and the site of CSF collection. These results lead to the hypothesis that ORP of CSF has a potential as monitoring biomarker in ALS, particularly in the cohort of patients with spinal onset. Antioxid. Redox Signal. 28, 1570–1575.
Introduction
A
The performance of clinical trials in amyotrophic lateral sclerosis (ALS) is limited by the lack of monitoring biomarkers. Herein, we report a strong relationship between oxidation–reduction potential (ORP) of cerebrospinal fluid (CSF) and revised ALS functional rating scale (ALSFRS-R) score, the primary clinical outcome measure in ALS. ORP is among just a few CSF parameters that showed significant correlation with ALSFRS-R score, and the best redox-related candidate for biomarker in ALS so far. The results presented in this study further confirm the involvement of oxidative stress in ALS progression and warrant further evaluation of the applicability of ORP as a monitoring biomarker in ALS.
Oxidative stress is involved in pathological mechanisms of ALS via cell death-related release of pro-oxidative compounds and redox-active iron, mitochondrial dysfunction, inflammation, and excitotoxicity (2, 4). Oxidative damage and iron accumulation have been reported to develop in the motor cortex and spinal cord of ALS patients (1, 5). Pro-oxidative processes in tissues reflect in the composition and properties of cerebrospinal fluid (CSF), which is in direct contact with the extracellular space. The concentrations of products of oxidation of lipids, DNA, proteins, and ascorbate, the level of nonsequestrated iron, and the capacity to generate free radicals are all significantly increased in the CSF of ALS patients (6, 8). Although CSF has been considered as an ideal source for developing biomarkers of neurodegeneration (9), previous search for a particular product of oxidation in CSF that could serve as a biomarker in ALS showed no apparent success. However, it has been contemplated that it is improbable for a single molecule to capture the complex biology of ALS (9). Hence, a potential biomarker should reflect oxidative status of CSF in a more general manner to take into account multiple oxidative pathways and the heterogeneous nature of this disease (1, 9).
Oxidation–reduction potential (ORP) represents an integrated comprehensive metabolimic analyte that measures the balance between oxidative and reductive species in biological fluids, including CSF (7). Higher ORP values stand for increased level of oxidizing and/or decreased level of reducing species in CSF.
Here, we analyzed the relationship between ORP of CSF and the degree of ALS progression (as determined by ALSFRS-R score) and compared ORP of CSF in ALS patients and patients with neurological non-neurodegenerative disorders (controls).
Results
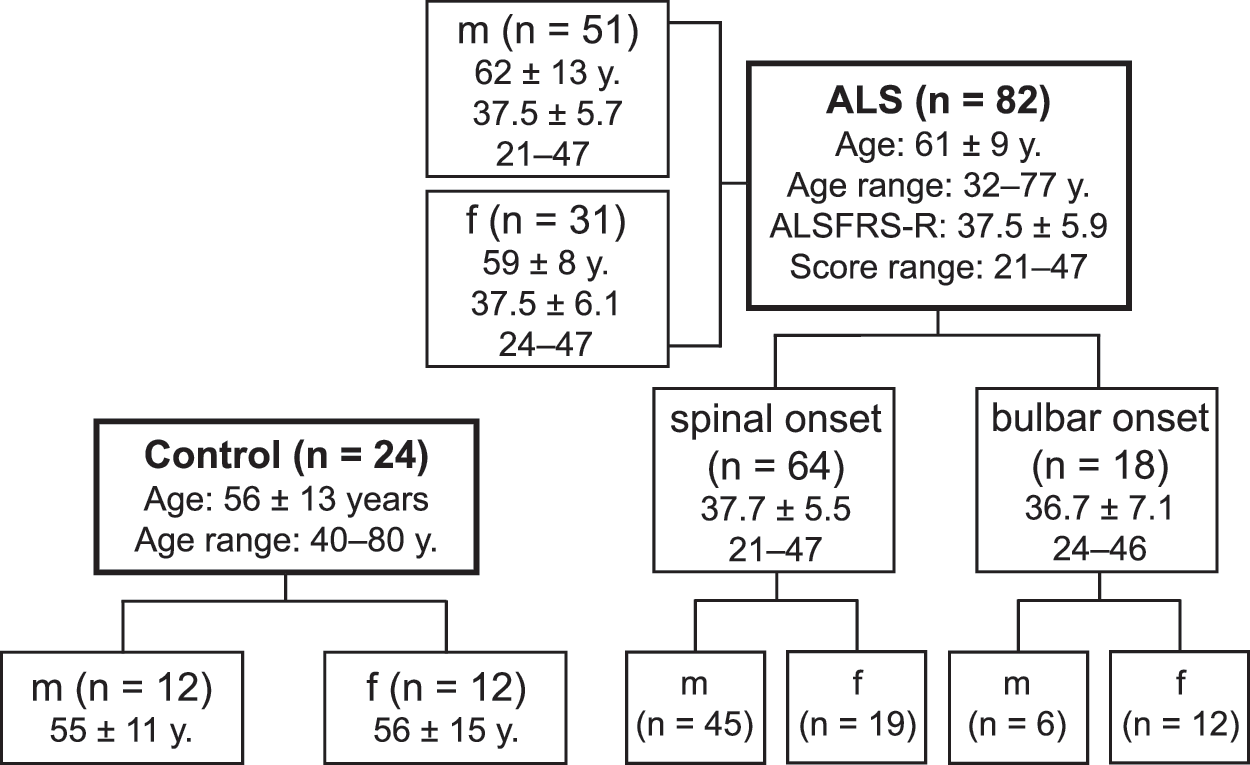
The study involved 82 ALS patients and 24 age-matching control patients (Fig. 1). To follow the results, it is important to have in mind a considerable overlap between the subset of patients with spinal onset and male patients (only ∼12% of male patients had bulbar onset), as well as that the majority of bulbar onset patients were women (∼67%). The distribution among subsets was in general agreement with the available epidemiological data on ALS (9).
ORP was significantly higher in all ALS patients and ALS patients with spinal onset than the control group (Fig. 2A). The highest measured ORP was at 190.4 millivolts (mV). In contrast, there was no significant difference for patients with bulbar onset compared with controls. It is worth mentioning that this is the first report on ORP of human CSF, placing referent control value at ∼110 mV. Three-way analysis of variance (ANOVA) further confirmed that ALS significantly affects ORP independently of gender and age (Fig. 2B). The differences in mean values between the two levels of health status (control and ALS) were greater than it would be expected by chance (p = 0.003), taking into account the differences in gender and age. The differences in the mean values between the two different levels of gender (m and f) and age (≤65 and >65 years of age) could be attributed to random sampling variability. Furthermore, the effects of different levels of health status were independent of gender or age.

Receiver operating characteristic (ROC) curve for all and spinal onset subjects showed significant area under curve (AUC) (Fig. 2C). The optimal cutoffs for these two groups were almost identical—108.4 mV and 108.6 mV, respectively. The cutoff ORP value (set at 108.4 mV for simplicity) represents a threshold that best separates redox settings in the CSF of ALS subjects and controls. The threshold most likely designates a point at which the pro-oxidative component of ALS pathology progressed to a level that has a significant impact on the redox status (i.e., ORP) of CSF. The established threshold was used in further analysis accordingly.
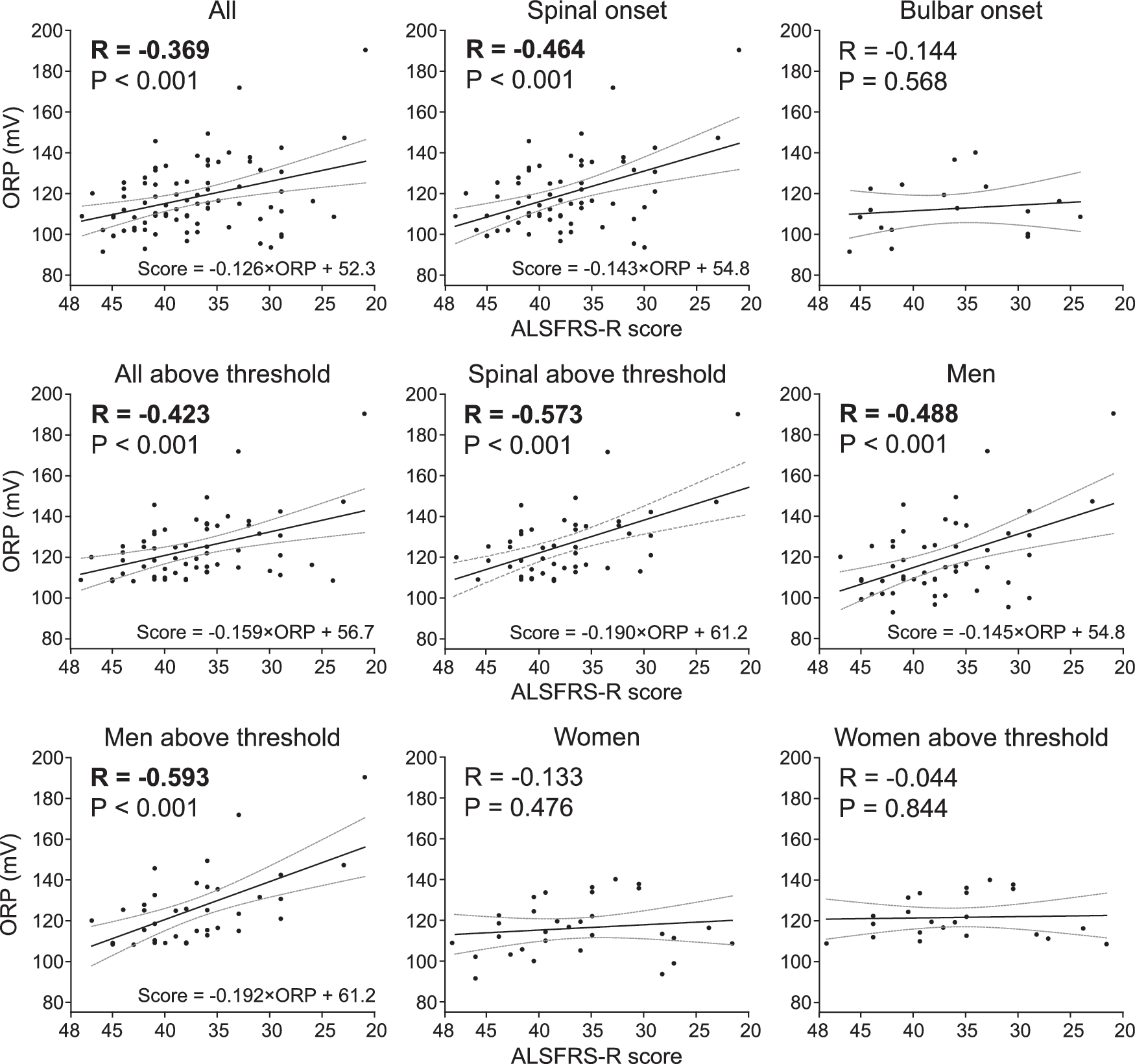
ORP showed significant negative correlation with ALSFRS-R score for all, spinal onset, and male patients (Fig. 3). The correlation was even stronger for patients with spinal onset and ORP above the threshold, and for male patients with ORP above the threshold. The correlation for the subset of men with spinal onset was stronger (R = −0.515; p < 0.001; not shown) than R for all male ALS patients (R = −0.488; p < 0.001). There was no correlation for patients with bulbar onset and for women. It is worth mentioning that there was no significant correlation between ORP and age for both, ALS and control group (R = 0.047; p > 0.05 and R = −0.278; p > 0.05, respectively; not shown).
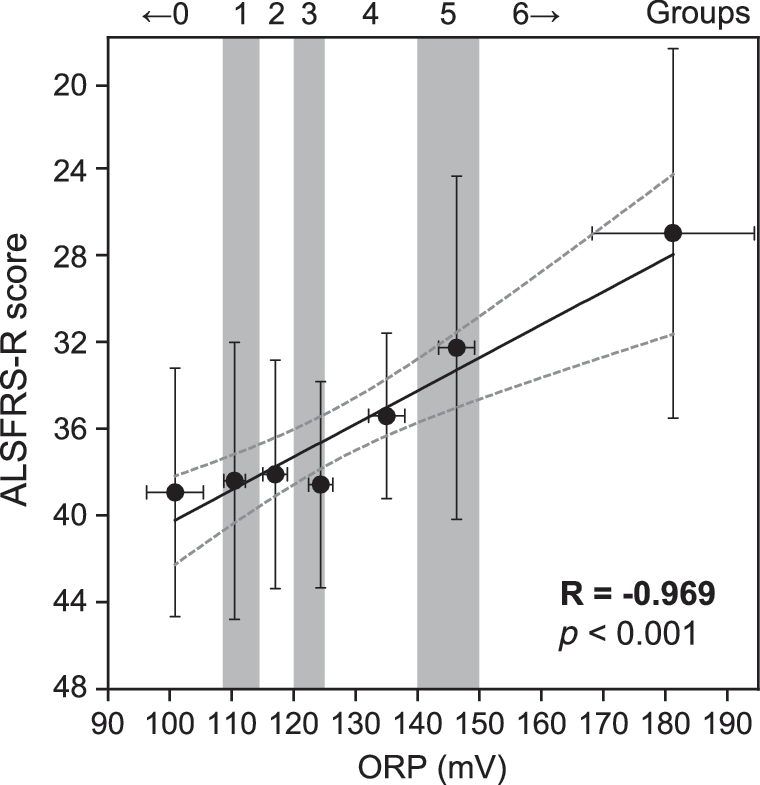
Next, we stratified ALS patients according to ORP (Fig. 4). All values below the threshold were put into one group (group 0). Values above the threshold were divided into six groups using K-means cluster analysis: (1) ORP = 108.4–115 mV; (2) ORP = 115.1–120 mV; (3) 120.1–125 mV; (4) ORP = 125.1–140 mV; (5) 140.1–150 mV; and (6) ORP >150 mV. Range limits were approximated to simplify the practical use of this approach. Mean ORP for the established groups increased with decreasing mean ALSFRS-R score (R = −0.969; p < 0.001).
Discussion
There is a critical need for drug development in ALS. The performance of clinical trials is largely hampered by the lack of sensitive and objective monitoring biomarkers. There are no FDA-approved standards for ALS monitoring. The degree of disease is only evaluated by measures of functional impairment, which do not allow rapid assessment of progression (9). The biological rationale for the development of an integrated redox CSF biomarker of ALS progression is strong. Multiple intertwined oxidative processes in cerebral and spinal tissues act jointly/synergistically to contribute to ALS progression and “spill over” to CSF (2, 6, 8, 9). Redox biomarkers of progression may be particularly important in the development or redox-active drugs, in the light of a recent approval of the second (antioxidative) therapeutic for ALS (edaravone; Radicava). The present case–control study found higher ORP in the CSF of ALS patients than control subjects. ROC curve analysis showed that ORP has a considerable sensitivity (72%) and moderate specificity (58%) in discriminating ALS patients from controls.
More importantly, ORP showed a strong relationship with ALSFRS-R score, the primary clinical outcome measure in ALS (9). In other words, ORP (oxidation) increased with ALS progression. The correlation was notably stronger for patients with spinal onset, which is a more frequent site of onset [about 70% of ALS cases (9)]. There was a considerable overlap between the subsets of spinal onset and male patients, and between bulbar onset and female patients. This overlap might be a confounding factor in the analysis. However, ORP was not affected by gender, there was no correlation for bulbar onset patients, and the correlation for male patients was improved when bulbar onset patients were excluded from the calculus. This implies that bulbar onset is characterized by lower responsiveness of ORP of CSF to pro-oxidative processes in the tissue. This might be related to the physical distance between the neurodegenerative loci (in the brain) and the site of CSF collection and the rostrocaudal concentration gradient of oxidizing species. The correlation between ORP and ALSFRS-R was further improved for the subset of spinal onset patients with ORP above the cutoff value that was extracted from the ROC curve, and particularly when stratification of ALS patients into seven clusters according to ORP was applied. It is important to note that measurements of ORP deliver objective and precise data expressed in physical unit for potential (increment: 0.1 mV; approximate range in CSF: 90–190 mV). The assay is simple (requires only a brief training and can be performed at the bedside), rapid (3 min between CSF collection and the beginning of the measurement +4 min for the measurement), and inexpensive (∼10 dollars per measurement). Finally, ORP showed no relationship with the age, which is a common issue with biomarkers for neurodegenerative diseases. The aging process has been associated with oxidative stress in the brain tissue, but it appears that such changes cannot overshadow the drastic effects of progressive neurodegeneration in ALS. Age independence simplifies the application of biomarkers (no need for age adjusting).
In close, ORP met a number of Foundation for the National Institutes of Health (FNIH) criteria for biomarker qualification (3), such as the need for drug and standards development, biological rationale, relationship with clinical outcome, and performance characteristics of the assay that are in line with the clinical application of the biomarker. This leads to the hypothesis that ORP of CSF has a potential as a monitoring biomarker in ALS. Further evaluation of the applicability of ORP in ALS progression monitoring is warranted. The next step is to conduct a prospective study in a larger cohort of spinal onset ALS patients with at least two time points of CSF collection, which was not ethically rationale before this study.
Notes
Patients
The study was conducted on consecutive 82 ALS patients and 24 controls who were treated/examined at the Neurology Clinic and the Neurosurgery Clinic, Clinical Center of Serbia, Belgrade (from March 2015 to March 2017), and who matched the criteria of the study. Patients with sporadic ALS were diagnosed according to revised El Escorial criteria (9). The disease duration was <5 years. A functional assessment was performed using ALSFRS-R scores (max. score = 48) by an experienced ALS neurologist, one day before the CSF collection. Serving as controls was a group of patients with neurological non-neurodegenerative disorders (9): migraine, tension headache, lumbar and cervical disk herniation, polyneuropathy, and idiopathic hydrocephalus. All patients received a balanced diet. Exclusion criteria were chronic medical conditions (diabetes, cancer, metabolic syndrome, and autoimmune diseases) and recent acute illness.
All participants were informed that their CSF samples were to be used for both required medical analyses and our research and provided written informed consent. Internationally recognized ethical standards (The Helsinki Declaration of 1964, as revised in 1975, 1983, and 1989) were followed during the patient recruitment, counseling, sample collection, and handling. Institutional approval for the study was granted by The Ethics Committee of the Clinical Center of Serbia, which followed international guidelines.
ORP measurements
CSF samples were collected, according to standard operating procedures, for routine medical analyses by lumbar puncture after an overnight bed rest and fasting. The remainder of the samples was used for this study. First 2 mL of CSF was discarded to minimize occult blood contamination. About 10 mL of CSF was collected in polypropylene tubes. All CSF samples were clear and blood-free at visual inspection. Static ORP (in mV) was measured at room temperature using RedoxSYS System (Aytu BioScience, Inc., Englewood, CO). CSF (40 μL) was applied to a preinserted sensor exactly 3 min after the collection, and the readings were initiated automatically. Short and fixed period between the sample collection and ORP measurements was required because pH of CSF may change due to dissolution of CO2 from the air, which may affect ORP values.
Statistical analyses
Statistical analyses were conducted using Sigma Plot 11.0 (Systat Software, Inc., San Jose, CA) and OriginPro 9.0 (OriginLab, Northampton, MA) software packages. Results are presented as box plots (or as means ± standard deviation). Boxes represent the median and the 25th and 75th percentiles; whiskers represent the nonoutlier range. Outliers and extremes are defined as data point values that are more than 1.5 × and 3 × interquartile range outside the box, respectively. Differences between groups were tested using nonparametric two-tailed Mann–Whitney U test (when two groups were compared), or using one-way ANOVA on ranks with Dunn's post hoc method (if >2 groups were compared). Results were considered to be statistically significant if p < 0.05.
Three-way ANOVA was run on a sample of 106 participants to examine whether there are interactions between independent variables—health status, gender and age, and the continuous dependent variable—ORP. Each independent variable was divided into two levels: (i) health status into control group and ALS patients; (ii) gender into male and female; and (iii) age into participants older and younger than 65 years. The data passed equal variance test. To meet the assumption of normality, data were square root transformed. ROC curve analysis was performed to evaluate diagnostic discrimination performance via sensitivity, specificity, and AUC, and to establish optimal cutoff value (according to Youden's index: the maximal sum of sensitivity and specificity). AUC of 1 represents a perfect discrimination between ALS and control patients, whereas AUC of 0.5 indicates no better discrimination than would occur randomly by chance. Pearson's correlation coefficient (R) was used to test the degree of correlation between ORP and ALSFRS-R scores, and between ORP and age. In addition, ALS patients were divided according to ORP using K-means cluster analysis, and semiquantitative ORP scores were attributed to each group (0–6). The optimal number of clusters was established using the “elbow” method.
Footnotes
Acknowledgments
We would like to thank Ivana Nešić and her team at the Neurology Clinic, Clinical Center of Serbia, for technical assistance during sample collection. This work was supported by Ministry of Education, Science and Technological Development of the Republic of Serbia, grant numbers OI173014 and III41014.
Author Disclosure Statement
No competing financial interests exist.