
Abstract
Aims:
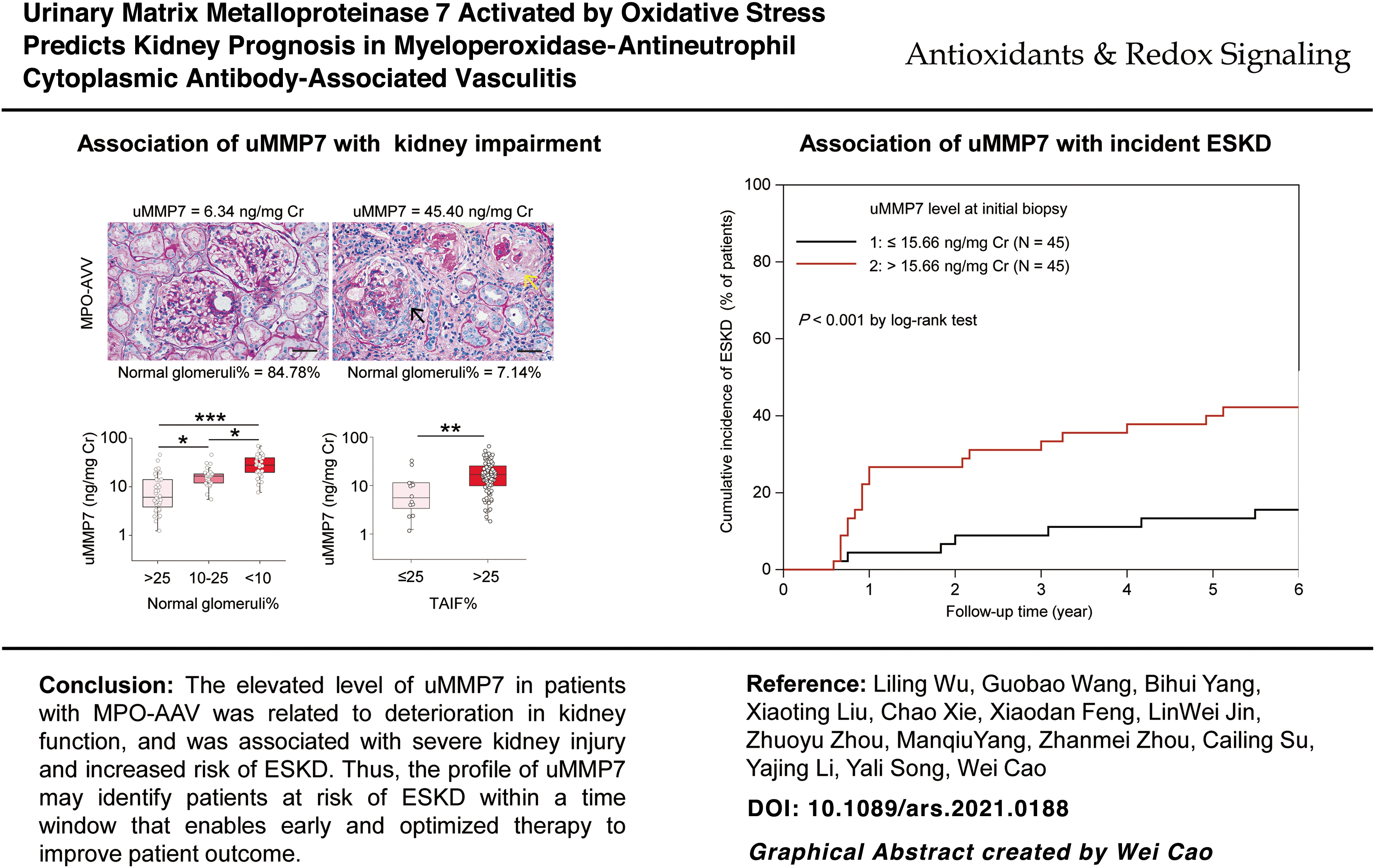
Effective and applicable predictors of end-stage kidney disease (ESKD) are needed for patients with myeloperoxidase–antineutrophil cytoplasmic antibody-associated vasculitis (MPO-AAV) and kidney involvement. We investigated whether urinary matrix metalloproteinase-7 (uMMP7) was associated with kidney injury severity and incident ESKD in MPO-AAV.
Results:
A prospective two-stage study was conducted in 150 patients with newly diagnosed MPO-AAV in two independent cohorts. uMMP7 was measured on the days of initial and repeat kidney biopsies. In stage I, a higher initial uMMP7 level was associated with a lower estimated glomerular filtration rate (eGFR), higher level of proteinuria, and greater extent of kidney pathologic lesions. This elevated uMMP7 protein level is activated and potentially derived from the enhanced kidney production induced by oxidative stress. In stage II, uMMP7 at initial biopsy was independently associated with the incidence of ESKD over 6 years. The higher uMMP7 group (vs. lower) had an adjusted hazard ratio of 3.79 (95% confidence interval [CI], 1.49–6.09) for ESKD in the test cohort. Findings were similar in the validation cohort. A combination of data from the two cohorts revealed that adding uMMP7 into clinical or clinicopathologic models significantly improved risk discrimination for future ESKD.
Innovation:
An elevated uMMP7 level in MPO-AAV was independently associated with severe kidney injury and incident ESKD.
Conclusions:
uMMP7 in MPO-AAV improves identification of patients at risk of ESKD and may enable early and optimized therapy to improve outcomes. Antioxid. Redox Signal. 37, 246–256.
Introduction
E
Inflammation and fibrosis are two key components of pathogenesis of kidney damage in antineutrophil cytoplasmic antibody-associated vasculitis (AAV) (9). Matrilysin, also known as matrix metalloproteinase-7 (MMP7), is a zinc- and calcium-dependent endopeptidase (18) that is expressed at low levels in normal epithelial cells of various organs (including the kidney). With induced expression, it promotes inflammation by enhancing neutrophil infiltration and promotes fibrosis by activating β-catenin (11, 31).
Innovation
Effective and applicable predictors of end-stage kidney disease (ESKD) or death are lacking for patients with myeloperoxidase–antineutrophil cytoplasmic antibody-associated vasculitis (MPO-AAV). We provided evidence based on samples from initial and follow-up kidney biopsies in two independent cohorts that an elevated level of urinary matrix metalloproteinase-7 (uMMP7) was independently associated with severe kidney injury and incident ESKD.
Thus, the profile of uMMP7 in MPO-AAV with kidney involvement may identify patients at risk of ESKD within a time window that enables early and optimized therapy to improve outcomes. However, this will require prospective clinical trials.
Kidney MMP7 is expressed on tubular epithelial cells that likely contribute to its urinary excretion. Indeed, urinary MMP7 (uMMP7) reflects kidney MMP7 expression and disease severity in chronic kidney disease (26, 31). However, whether the uMMP7 level is predictive of kidney outcome in MPO-AAV remains unclear. Therefore, in two prospective cohorts of patients with MPO-AAV and kidney involvement, we investigated the relationship between urinary excretion of MMP7 and severity of kidney damage, assessed from both initial and repeat kidney biopsies, and explored its association with incident ESKD.
Results
Patients
This is a prospective, two-stage cohort study that was undertaken in two independent cohorts of patients with MPO-AAV and kidney involvement (Fig. 1). It included 150 patients: 90 patients from one hospital in Guangzhou (test cohort) and 60 patients from the other hospitals (validation cohort). Summary statistics for total cohorts or cohorts dichotomized according to the median uMMP7 level (15.66 ng/mg creatinine) are shown in Table 1 and Supplementary Table S1. There was no difference in patient characteristics between the test and validation cohorts.

Characteristics of Patients with Myeloperoxidase–Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
Continuous data are expressed as mean ± SD or median (interquartile range). Categorical data are expressed as n (%).
AZA, azathioprine; eGFR, estimated glomerular filtration rate; MMF, mycophenolate mofetil; SD, standard deviation; TAIF, tubular atrophy and interstitial fibrosis; uMMP7, urinary matrix metalloproteinase-7.
Relationship between uMMP7 and kidney impairment
Levels of uMMP7 on the day of the initial biopsy were contrasted in patients of the test cohort (N = 90) and healthy controls (N = 30). Compared with those in the healthy controls (median 1.37, [interquartile range, IQR 0.91–2.10] ng/mg creatinine), the uMMP7 levels in patients of the test cohort were markedly elevated by >10-fold (15.66 [7.60–24.80] ng/mg creatinine) (p < 0.001, Fig. 2A).

Enzyme-linked immunosorbent assay (ELISA) results were further confirmed by Western blot as the active form of MMP7 (20 kDa) was significantly increased in urine samples from patients of the test cohort (Supplementary Fig. S1). Serum levels of MMP7 were also significantly increased in patients, but the difference from controls was only twofold (Supplementary Fig. S2A), and no correlation was identified between serum and uMMP7 levels (Supplementary Fig. S2B).
Urinary excretion of MMP7 was found to be independently associated with the eGFR or proteinuria in patients with MPO-AAV after adjusting for clinically important confounding variables, including age, gender, use or nonuse of plasma exchange, and the type of maintenance therapy (Supplementary Table S2). Patients with a higher rate of uMMP7 excretion at initial biopsy had a lower eGFR and a greater degree of proteinuria (Fig. 2B, C).
The uMMP7 level was further compared with kidney expression of MMP7. Immunoreactive levels of MMP7 were barely detected in normal kidney tissues (N = 10, Supplementary Fig. S2C), but were markedly expressed in biopsy specimens from patients in the test cohort (N = 90) where MMP7 was predominantly localized within tubular cells (Fig. 3A, blue arrows). Double-label experiments revealed that the tubular MMP7 protein colocalized with MMP7 messenger RNA (mRNA) and Nox4 protein, but not with megalin protein (Supplementary Fig. S3). The urinary excretion of MMP7 correlated positively with its kidney expression (Fig. 3A).
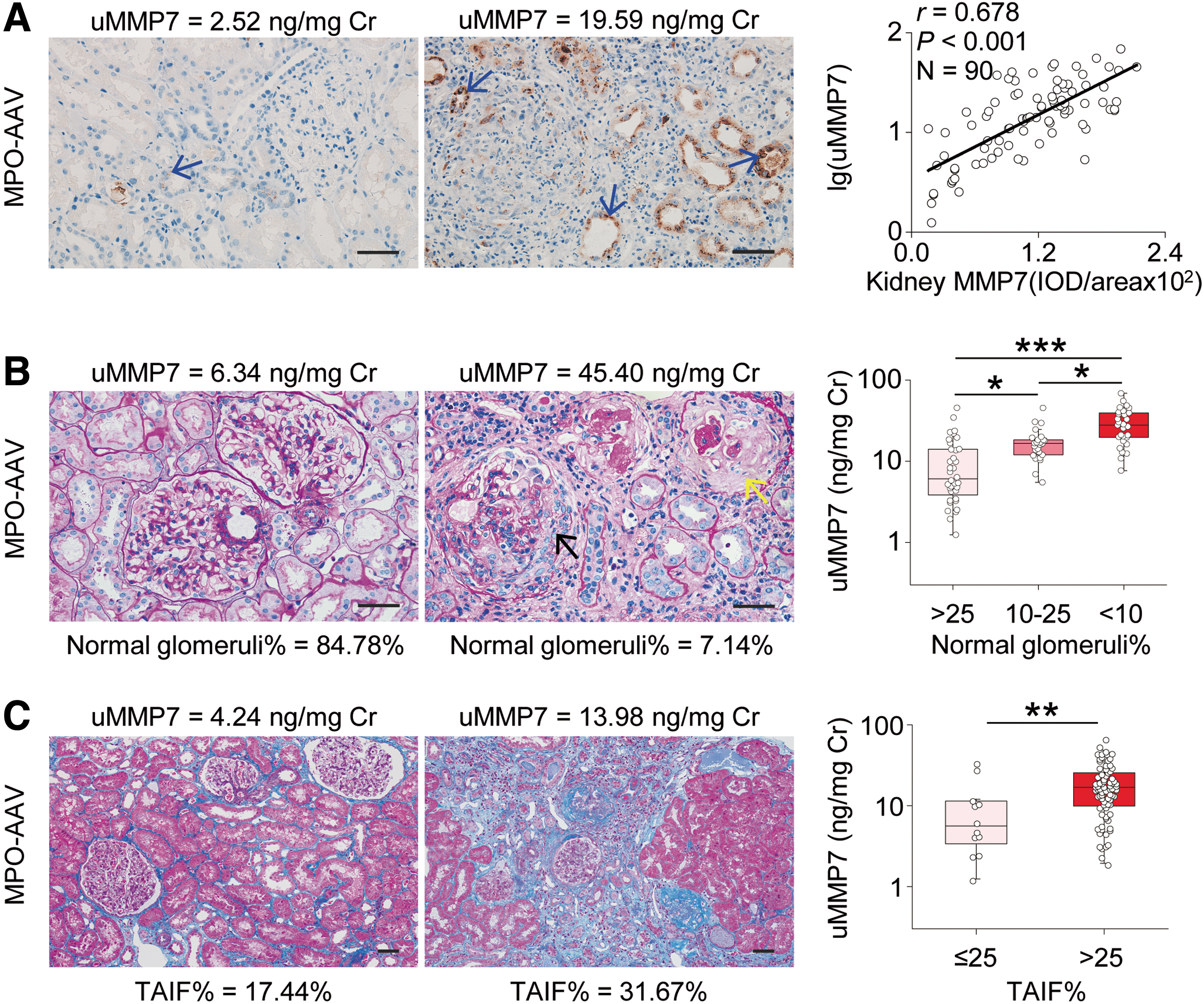
Consistent with the close relationship of uMMP7 with kidney function, uMMP7 excretion was independently associated with the percentage of normal glomeruli, percentage of interstitial inflammation, and degree of tubular atrophy and interstitial fibrosis (TAIF) at initial biopsy (Supplementary Table S2). Thus, patients with the highest rates of uMMP7 excretion had the lowest percentage of normal glomeruli (Fig. 3B) and greatest degree of TAIF (Fig. 3C).
Association of uMMP7 with incident ESKD
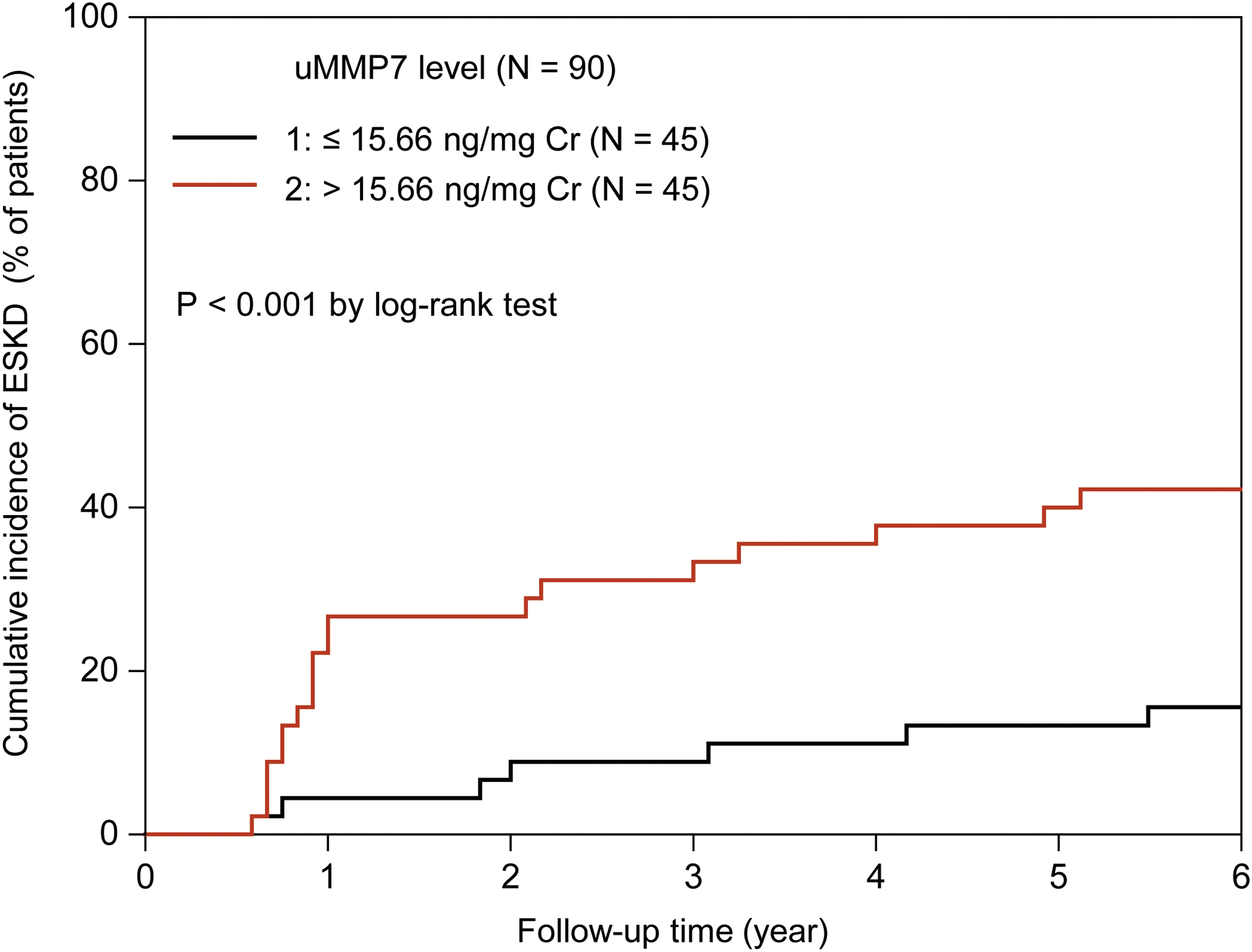
We determined the association of the uMMP7 level at initial biopsy with the incidence of ESKD among 90 participants of the test cohort who had a median follow-up period of 37.98 (12.00–63.90) months. ESKD occurred in 26 subjects and death occurred in 8 subjects. A uMMP7 level above the median value (>15.66 ng/mg creatinine) was associated with a significantly greater cumulative incidence of ESKD (p < 0.001) (Fig. 4) that was 4.90 times (95% confidence interval [CI], 1.98–7.87) that of subjects with a lower uMMP7 level (model 1, Fig. 5A).
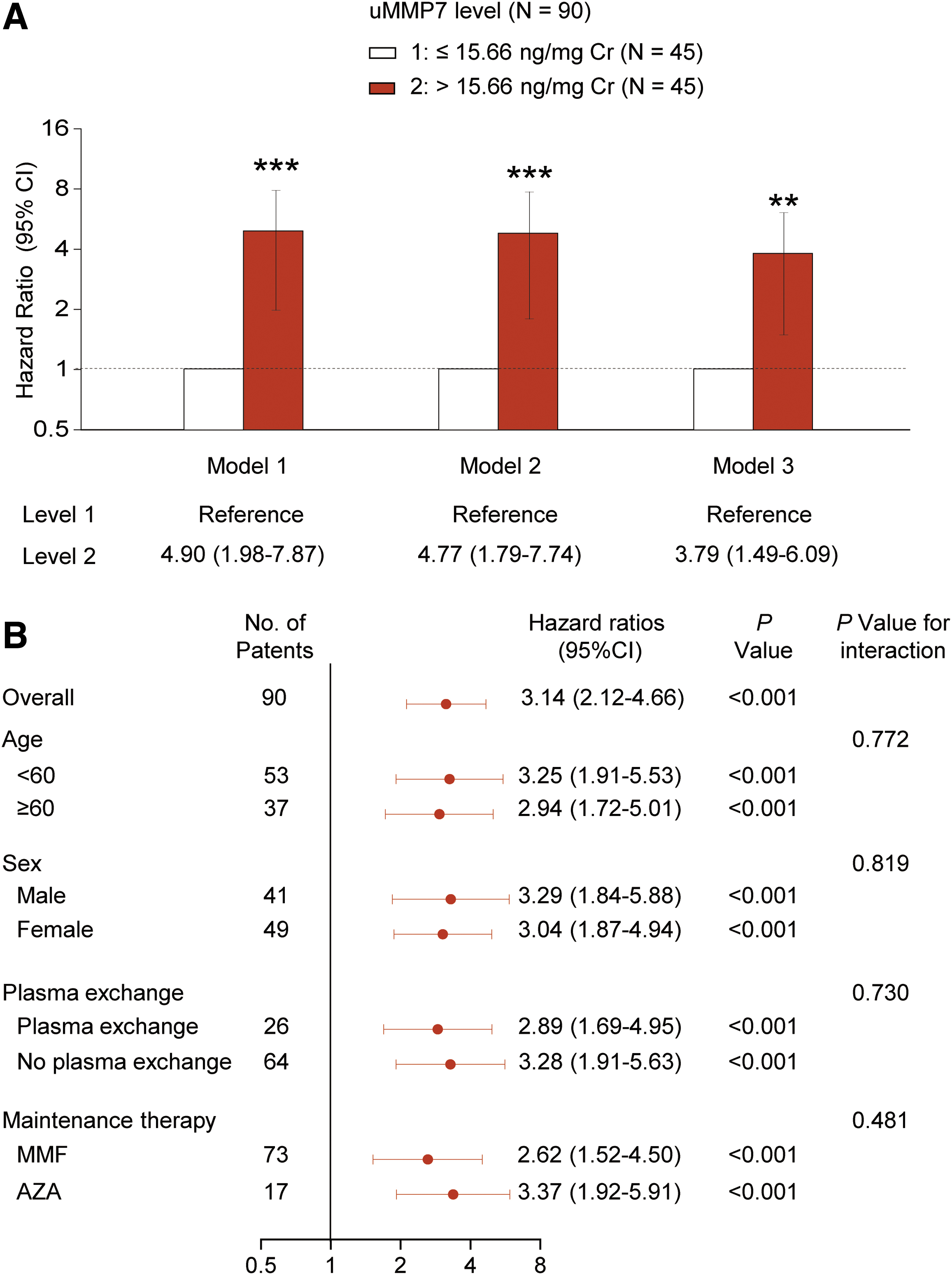
This association of uMMP7 and ESKD persisted after adjustment for clinical parameters (including age, gender, use or nonuse of plasma exchange, and the type of maintenance therapy; model 2) or adjustment for both those and pathological characteristics (percentage of normal glomeruli and degree of TAIF; model 3) (Fig. 5A). The hazard ratio for incident ESKD remained consistent across subgroups (Fig. 5B).
The incremental value of adding uMMP7 to traditional clinical models in predicting incident ESKD was assessed (Supplementary Table S3). The c-statistic of the base model [clinical data at biopsy (1)] was 0.734 (95% CI, 0.638–0.830) at 5 years of follow-up. It was improved by adding uMMP7 to 0.804 (0.714–0.894), which became similar to that of the clinicopathologic model proposed by Brix et al. (1). The c-statistic of the clinicopathologic model also was increased with addition of uMMP7 (Supplementary Table S3).
Addition of uMMP7 to the clinicopathologic model was associated with a change in R 2 of 0.1535, a change that was larger compared with all other variables (Supplementary Table S4). The optimal cutoff point for the uMMP7 level that achieved maximized discrimination was 20.00 ng/mg creatinine, which provided a c-statistic of 0.853 in multivariable analyses (Supplementary Fig. S4).
Characteristics of five subjects who underwent a repeat biopsy due to suspected kidney relapse after a minimum 2-month maintenance therapy (median follow-up of 29 months) are summarized in Supplementary Table S5. ESKD occurred in two subjects with the uMMP7 level >20.00 ng/mg creatinine at both biopsies. The uMMP7 level was increased in all patients at the second biopsy.
However, those who developed ESKD had an exaggerated elevation in urinary and kidney MMP7, which was associated with worse renal histological damage (Supplementary Fig. S5). Consistent with these data, among 45 participants who had follow-up uMMP7 measurements, uMMP7 levels declined with clinical remission (at diagnosis vs. at remission: 13.76 [7.94–19.52] vs. 6.12 [4.10–8.31] ng/mg creatinine; p < 0.001) (Supplementary Fig. S6).
Validation analyses
We repeated the two-stage longitudinal analyses with a validation cohort (N = 60) in which patients had a median follow-up period of 37.20 (12.00–64.89) months. ESKD developed in 19 patients and death in 5. Consistent with findings in the test cohort, an elevated uMMP7 level at initial biopsy was associated with severe kidney histologic damage and with increased risk of ESKD (Supplementary Tables S6–S8) and was associated with a combined outcome of ESKD or death (Supplementary Tables S9 and S10).
A combination of data from the two cohorts revealed that adding uMMP7 to the base clinical model improved the c-statistic from 0.700 (0.628–0.773) to 0.790 (0.717–0.863; p = 0.020) at 5 years of follow-up. The c-statistic of the clinicopathologic model (0.763 [0.706–0.819]) also was increased with addition of uMMP7 (0.829 [0.772–0.885]; p = 0.036).
Discussion
This study of patients with MPO-AAV has demonstrated that an elevated level of uMMP7 is related to severe kidney histologic impairment and incident ESKD.
Three general mechanisms may contribute to elevated uMMP7 excretion: enhanced kidney production, increased glomerular filtration, or abnormal tubular reabsorption. Serum MMP7 did not correlate with uMMP7 in patients with MPO-AAV. Tubular expression of megalin, an endocytic receptor that mediates resorption of MMPs (7), was comparable between healthy controls and patients with MPO-AAV.
Thus, elevated uMMP7 levels are unlikely to be the result of increased filtration or decreased tubular reabsorption. The potential site of MMP7 secretion into the urine is the kidney (26, 30, 31). We observed a dramatic increase in MMP7 expression in kidney tubular epithelial cells from biopsies of patients with MPO-AAV and demonstrated a strong correlation between uMMP7 and kidney MMP7 expression. Kidney tubular epithelial cells, therefore, are likely the main source of uMMP7.
We further confirmed that kidney MMP7 did not colocalize with megalin, suggesting that much of the kidney MMP7 has not been attributed to tubular reabsorption, but is rather locally synthesized. In fact, kidney expression of MMP7 protein and mRNA was strongly correlated, implying that much of the increased uMMP7 is derived from enhanced local production and may be related to pathogenic mechanisms initiating kidney injury.
Evidence that MMP7 plays a pathogenic role in kidney injury has emerged from studies of chronic kidney disease, in which MMP7 enhances neutrophil infiltration and activates β-catenin to induce inflammation and fibrosis (11, 31). Usually, MMP7 is produced in a latent form (8). Upon activation, its proregion is removed, resulting in the final active enzyme (31).
Our results extend reports on chronic kidney disease (27), demonstrating elevation of the active form of MMP7 in urine samples from patients with MPO-AAV. We further confirmed that kidney MMP7 colocalized with Nox4 (a subunit of NADPH oxidase), supporting a potential role of oxidative stress in MMP7 activation (4). Moreover, an elevated level of uMMP7 was associated with impaired kidney function and severe structural damage to the kidney on biopsy.
In a small group, the uMMP7 level at initial biopsy was increased at repeat biopsy, in proportion to worsening kidney function. Among 45 patients who had follow-up uMMP7 measurement, the uMMP7 level declined with clinical remission. All these data support a pathogenic role of MMP7 in kidney injury and establish uMMP7 as a potent biomarker of kidney impairment in MPO-AAV.
ESKD is a frequent outcome in patients with AAV and kidney involvement (3, 20, 23, 25), but current algorithms for identifying patients at risk are limited to measurement of kidney function and histology (1, 5, 15). Other biomarkers have either not been tested in prospective studies or have not provided enough clinically actionable windows (14, 16, 17, 27).
In this prospective study, we demonstrated that the level of uMMP7 at presentation (initial biopsy) was predictive of ESKD in two independent cohorts, across subgroups, and that it was independent of conventional risk factors (i.e., kidney function and histologic changes). Incorporation of uMMP7 into a standard clinicopathologic model (1) significantly improved risk discrimination for incident ESKD, as evidenced by the significant increment in the c-statistic.
An improved assessment of the risk for ESKD at an early stage, especially before a kidney biopsy, would allow for informed decision-making with an actionable time window and help to identify a subgroup of patients who could benefit from immunomodulation therapy.
The present study was prospective, but observational, and therefore potentially subject to bias. However, with the use of a log-rank test with a Cox proportional hazards model, we demonstrated a significant association between the initial level of uMMP7 and the risk of ESKD. Importantly, this was confirmed in a sensitivity analysis and in a validation cohort and remained significant after adjusting for multiple clinical confounders, including age, gender, use or nonuse of plasma exchange, and the type of maintenance therapy, percentage of normal glomeruli, and degree of TAIF.
In addition, our study includes only Chinese people with a modest sample size. Thus, further validation of our results will require prospective clinical trials with larger sample sizes and multiethnic subjects.
The present study has some strengths. Consistent results were obtained from two independent cohorts with a total of 150 MPO-AAV subjects and a wide range of kidney injury severity scores. The findings that the level of uMMP7 predicted kidney damage and outcome from both initial and repeat kidney biopsies strengthen the conclusion. Finally, the level of uMMP7, especially the active form of MMP7, was measured and validated by an ELISA kit and Western blot.
In conclusion, an elevated level of uMMP7 in patients with MPO-AAV was related to deterioration in kidney function and was associated with severe kidney injury and increased risk of ESKD. Thus, the profile of uMMP7 may identify patients at risk of ESKD within a time window that enables early and optimized therapy to improve patient outcomes.
Materials and Methods
Study design and patients
This prospective, two-stage cohort study was performed in two independent cohorts of patients with MPO-AAV and kidney involvement (Fig. 1). The study was approved by the local Ethics Committees in each hospital (NFEC-2019-209, L[2018]-3, and GZKYEC-201608-K1-02). Written informed consent was obtained from each subject in accordance with the Declaration of Helsinki. The electronic laboratory notebook was not used. The STROBE_checklist_cohort was used in reporting this study.
Study participants were recruited from three tertiary university hospitals in two cities between 2000 and 2018. For the test cohort, 90 patients were recruited from one hospital in Guangzhou. For the validation cohort, 60 patients were recruited from other hospitals in Foshan and Guangzhou.
All eligible patients were 18 years of age or older and had new microscopic polyangiitis consistent with the Chapel Hill consensus definitions (6), a history of a positive test for the antimyeloperoxidase (MPO) antibody, and biopsy-proven kidney involvement. Patients were excluded if they had other coexisting glomerular diseases. Thirty age- (53 ± 14 years) and gender- (female, 56.7%) matched healthy volunteers were included as normal controls.
Stage I used these two independent cohorts to investigate the relationship of uMMP7 at initial biopsy with kidney function (eGFR and proteinuria) or kidney histologic impairment (percentage of normal glomeruli, percentage of interstitial inflammation, and degree of TAIF) (1). All patients underwent initial kidney biopsies at clinical onset and before commencement of immunosuppressive therapy.
Stage II examined the association of uMMP7 at initial biopsy with ESKD or with a combined outcome of ESKD or death from any cause in the two cohorts of patients who were followed up for at least 12 months (including those who had died within 12 months). ESKD was defined as 3 or more months of kidney replacement therapy or kidney transplantation. A repeat biopsy was performed in five participants who were under suspicion of kidney relapse after at least 2 months of clinical remission and maintenance therapy. This permitted us to assess the relationship of uMMP7 at both biopsies with kidney histologic impairment and outcome in this small group. All patients were followed up for at least 23 months.
Remission was defined as the absence of disease activity (i.e., Birmingham Vasculitis Activity Score [BAVS] >0, hematuria, or increase of serum creatinine) attributable to active disease (27). Renal relapse was defined as the presence of hematuria or an increase of serum creatinine (15).
Treatment
All participants were initially treated with daily intravenous methylprednisolone (1 g/day) for 1–3 days, followed by oral prednisone at a starting dose of 1 mg/kg/day, which tapered to 5 mg/day after 18–24 months. Patients also received intravenous cyclophosphamide (15 mg/kg/pulse, maximum dose 1.2 g/dose) administered every 2 weeks for the first 3 doses and every 3 weeks thereafter.
After 3–6 months of cyclophosphamide induction, patients received mycophenolate mofetil or azathioprine as maintenance therapy for at least 2 years. Patients who presented with severe pulmonary hemorrhage and/or acute renal injury at diagnosis received hemodialysis and plasma exchange.
Measurement of kidney function
Serum creatinine and 24-h proteinuria were assessed at the day of the biopsy and subsequently as required in a clinical laboratory. Twenty-four-hour proteinuria was dichotomized according to the median proteinuria level in the test cohort (1.5 g/day). The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation (10) and divided into four groups: ≥60, 30–59, 15–29, and ≤15 mL/1.73/m2.
Sample collection and measurement of MMP7
Arterial blood samples were obtained after overnight fasting. Fresh urine samples were collected upon waking, as previously described (29). Plasma and urine samples were stored at −80°C. MMP7 was measured using an ELISA kit (DY907; R&D) (26) with an interassay variability of 5.3%. uMMP7 was expressed as ng/mg creatinine. uMMP7 was further assessed by standard Western blot analyses with the anti-human MMP7 (1:200, AF907; R&D) antibody.
Kidney specimens were obtained from diagnostic kidney biopsies. Nontumor kidney tissues from patients with kidney carcinoma served as normal controls (21, 28). Kidney expression of the MMP7 protein was determined using an anti-human MMP7 (1:100, AF907; R&D) antibody (26). MMP7 immunostaining was measured using Image-Pro Plus software (version 6.0; Media Cybernetics), and data are expressed as the ratio of integrated optical density (IOD) to observed area (IOD/area) (2).
Kidney expression of MMP7 mRNA was examined using in situ hybridization (12). The probe sequence for MMP7 was /5DiGN/ATGCGGTAAGTCTCGAGTATA/3DiG_N/. Kidney localization of MMP7 was determined by double staining using the anti-MMP7 antibody (1:100; R&D) as the first primary antibody and anti-megalin (1:100; ab76969; Abcam, Cambridge, United Kingdom) or anti-Nox4 (1:100; GTX121929; GeneTex) antibody as the second primary antibody.
Histologic evaluation
Kidney tissue with a minimum of 10 whole glomeruli was processed for periodic acid-Schiff and Masson trichrome staining (19). The percentage of normal glomeruli was assessed and divided into three categories according to the renal risk score system proposed by Brix et al. (1): N0 (>25%), N1 (10%–25%), and N2 (<10%). The degree of TAIF was classified into two groups (1): T0 (≤25%) and T1 (>25%).
Kidney tissue was examined by two independent nephropathologists who were blinded to participants' data. The inter- and intraobserver reproducibility of scoring (22) displayed good reliability (intraclass correlation coefficient [ICC] 89.9%, 95% CI 84.7%–93.4%; ICC 88.4%, 95% CI 82.9%–92.2%).
Statistical analyses
Continuous variables are presented as means (±standard deviations) or as medians (IQRs), and categorical variables are expressed as proportions. We used independent sample t-tests or the Kruskal–Wallis test to compare continuous variables and chi-square tests to compare categorical variables. Correlations were determined using Pearson's correlation coefficients.
The association of uMMP7 levels at biopsy with kidney function (eGFR and proteinuria) or kidney histologic injury (percentage of normal glomeruli and degree of TAIF) was assessed using a multiple regression analysis with adjustment for clinically important confounding variables (age, gender, use or nonuse of plasma exchange, and the type of maintenance therapy, percentage of normal glomeruli, and degree of TAIF).
We included participants who had follow-up eGFR measurements for at least 12 months to evaluate the occurrence of ESKD or a combined outcome of ESKD or death according to the MMP7 level, using the log-rank test and a Cox proportional hazards model with adjustment for the aforementioned covariates. The c-statistic was calculated to test the incremental value of adding uMMP7 to traditional risk models predicting incident ESKD.
Two-tailed p values of <0.05 were considered to be statistically significant. All analyses were performed with R, version 3.2.0 (The R Foundation;
Data Availability
All data required to evaluate the conclusions in the article are present in the article or its Supplementary Data. Further information on the study protocol or deidentified datasets generated and analyzed within this publication are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
W.C. contributed to the conception and design of the study. C.X., X.F., L.J., Z.Z., M.Y., Y.L., and Y.S. contributed to acquisition of data. L.W., G.W., B.Y., and X.L. were responsible for data analysis and L.W., G.W., B.Y., X.L., and W.C. were responsible for data interpretation. W.C. wrote the original draft. All authors were involved in reviewing and editing of the article and approved the final version. L.W., G.W., and W.C. verified the data, had full access to all the data in the study, and had final responsibility for the decision to submit for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (grant Nos. 81922014, 81870473, 81870489, and 82100710) and Guangdong Basic and Applied Basic Research Foundation (grant No. 2020A1515110398).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
STROBE_checklist_cohort
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.