
Abstract
Inflammation causes a wide range of health disorders. In this process, the formation of inflammasome complexes plays a key role. Although inflammasomes have been extensively studied during kidney disease, their role in kidney transplantation has not been fully elucidated. In this study, we evaluate the gene and protein expression of several components of the inflammasome pathway before and at several time points after kidney transplantation in a cohort of patients of different ages and receiving an organ from older or younger donors. Our findings indicate the activation of the NLRP1 inflammasome in several immune cell population, monocytes and CD4+ and CD8+ cells mainly, in renal transplant, and its level increases gradually in patients who receive an older organ, whereas it has the opposite effect on older patients who receive a younger organ. Despite treatment with immunosuppressants, inflammation persists in some patients. These results lead to the hypothesis that the donor's age is a critical factor in post-transplant inflammasome activation and that specific NLRP1 inflammasome inhibitors should be considered to increase the success of kidney transplantation long-term.
Color images are available online.

Introduction
Kidney transplantation is the preferred treatment for severe kidney failure, as it improves the patient's quality of life and reduces mortality compared with hemodialysis (Yngman-Uhlin et al., 2016). However, as most transplants involve allogeneic organs, an immune response can be triggered against the foreign organ, leading to reduced graft survival and treatment efficacy. Immunosuppressants such as tacrolimus are commonly used to address this issue, but long-term immunosuppression can lead to chronic alloimmunity and nephrotoxicity (Wojciechowski and Wiseman, 2021).
Organ rejection is a severe stress caused by the immune system's inability to recognize the allogenic organ, leading to a destructive immune response against it. Inflammation is critical in the rejection process and is activated in kidney disease cases even before the organ transplant, being associated with secondary pathologies such as cardiovascular events (Tuegel and Bansal, 2017). Despite its complexity, understanding how inflammation influences these pathologies could aid in the development of new and better treatments for patients.
The NLRP-inflammasome complex, a multiprotein complex that drives caspase 1 maturation, interleukin (IL) 1β, and IL-18 processing, leading to a cell death process known as pyroptosis, has been implicated in numerous human diseases (Fusco et al., 2020). The NLRP3 inflammasome has been widely studied and also implicated in several renal conditions (Hutton et al., 2016). However, other sensors could be involved in the immune response raised in renal transplantation. NLRP1 is a potential candidate associated with many conditions such as vascular diseases, brain injuries, or skin diseases, and is currently a subject of study in the inflammaging process (Burian et al., 2023).
Innovation
Kidney transplantation is the preferred treatment for severe kidney failure, as it improves the patient's quality of life and reduces mortality compared with hemodialysis. However, it is not exempt from numerous complications during the process and even long after transplantation; it worsens the quality of life of the patients, inflammation being a major problem. In this study, we show that inflammasome complexes mediate the inflammation during the transplant, which is associated with the donor age on which old donors induce significant activation of NLRP1 and NLRP3 complexes. However, NLRP3 is downregulated after several days and NLRP1 persists for a long time despite the immunosuppressant treatments, suggesting that it may be an attractive therapeutic target. NLRP3-specific inhibitors have been previously tested using animal models with positive outcomes; however, the treatment was only used for several hours after transplant. According to this, our finding shows a need to design inhibitors of NLRP1 or even of both NLRP1 and NLRP3 at the same time.
In this study we provide evidence indicating that NLRP1 inflammasome is persistently activated in renal transplanted patients, and we point to the age of the donor organ as a factor driving higher levels of inflammation. We also explore the possible contribution of currently used immunosuppressant treatments in the inflammasome activation,
Results
Our first analysis focused on evaluating the gene expression levels of two key inflammasome proteins: NLRP1 and NLRP3. Initial findings indicated that NLRP3 exhibited a rapid decline after 7 days after the transplant, whereas NLRP1 remained stable (Fig. 1A). Of note, during the initial time points, we observed significant standard deviation values, suggesting the presence of distinct patient subgroups. Consequently, we divided the sample of patients into three groups based on the age of the donor relative to the patient: Older Donor, Younger Donor, and Matched. Groups and patient data are given in the Notes section.
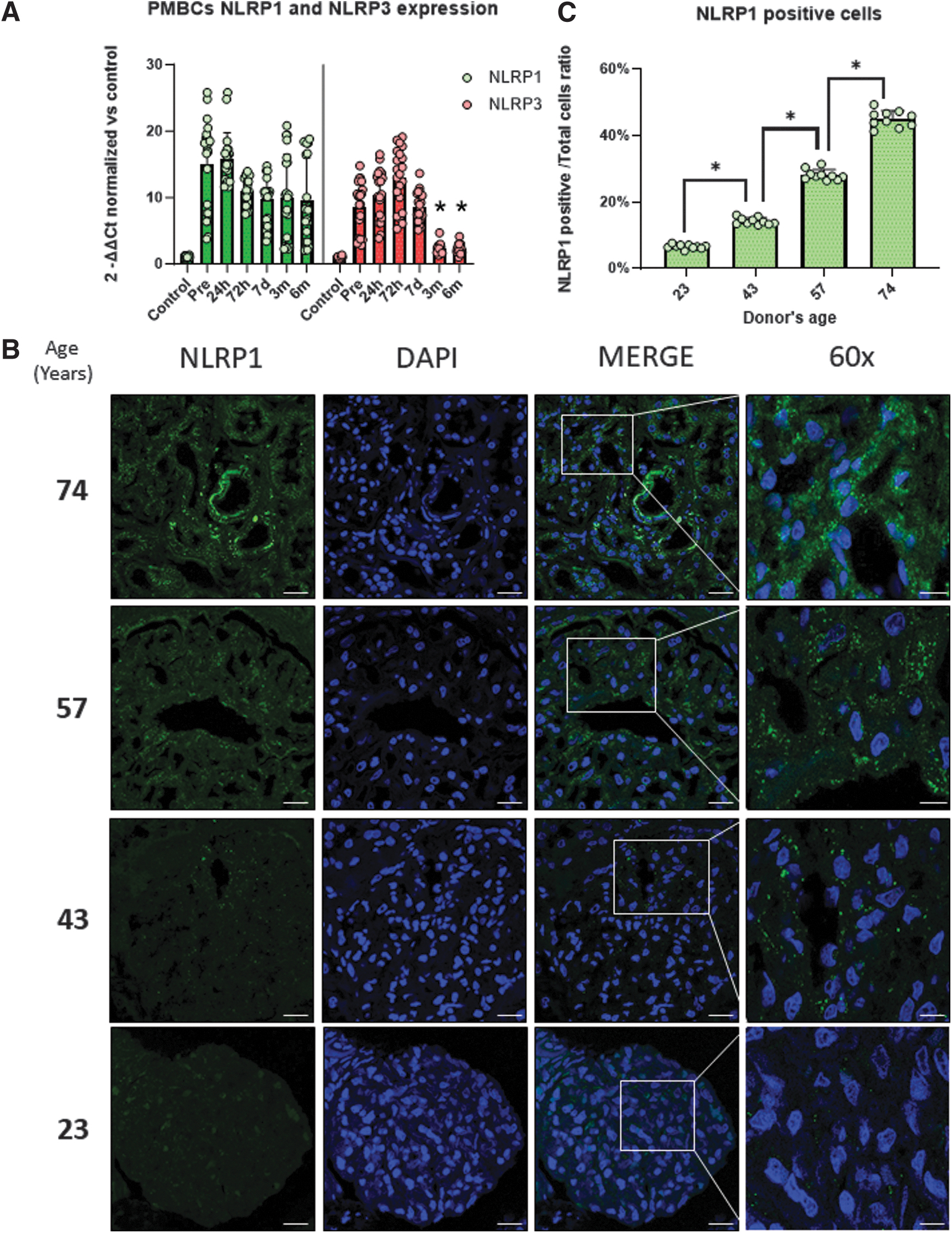
In addition, we aimed to assess the levels of inflammation in the kidney of the donor. To achieve this, we conducted an immunofluorescence assay on a pretransplant kidney biopsy, specifically examining NLRP1. We selected biopsies from donors of different ages: 23, 43, 57, and 74 years. Our observations revealed a progressive increase in NLRP1 expression associated with age, predominantly localized around blood vessels (Fig. 1B).
Next, we analyzed the expression levels of several genes and proteins related to inflammasome formation and activity of each group, including NLRP1, ASC, caspase 1, and NLRP3.
Our results showed that donor age correlated with inflammasome expression levels. Receiving an older kidney increased NLRP1 expression over time, whereas receiving a younger kidney had the opposite effect (Fig. 2A). ASC and caspase-1 both increased in the first few days after surgery, but their levels stabilized at later times (Fig. 2B, C). NLRP3 expression followed a similar pattern but decreased faster in all groups (Fig. 2D). For all studied genes, initial expression levels were lower in young patients than in older ones, but they rose or fell depending on the donor's age. This difference in starting expression could be owing to previous renal failure and/or the inflammaging process. Regardless of that, the presented results suggested the potential activation of the NLRP1 inflammasome in all patients.
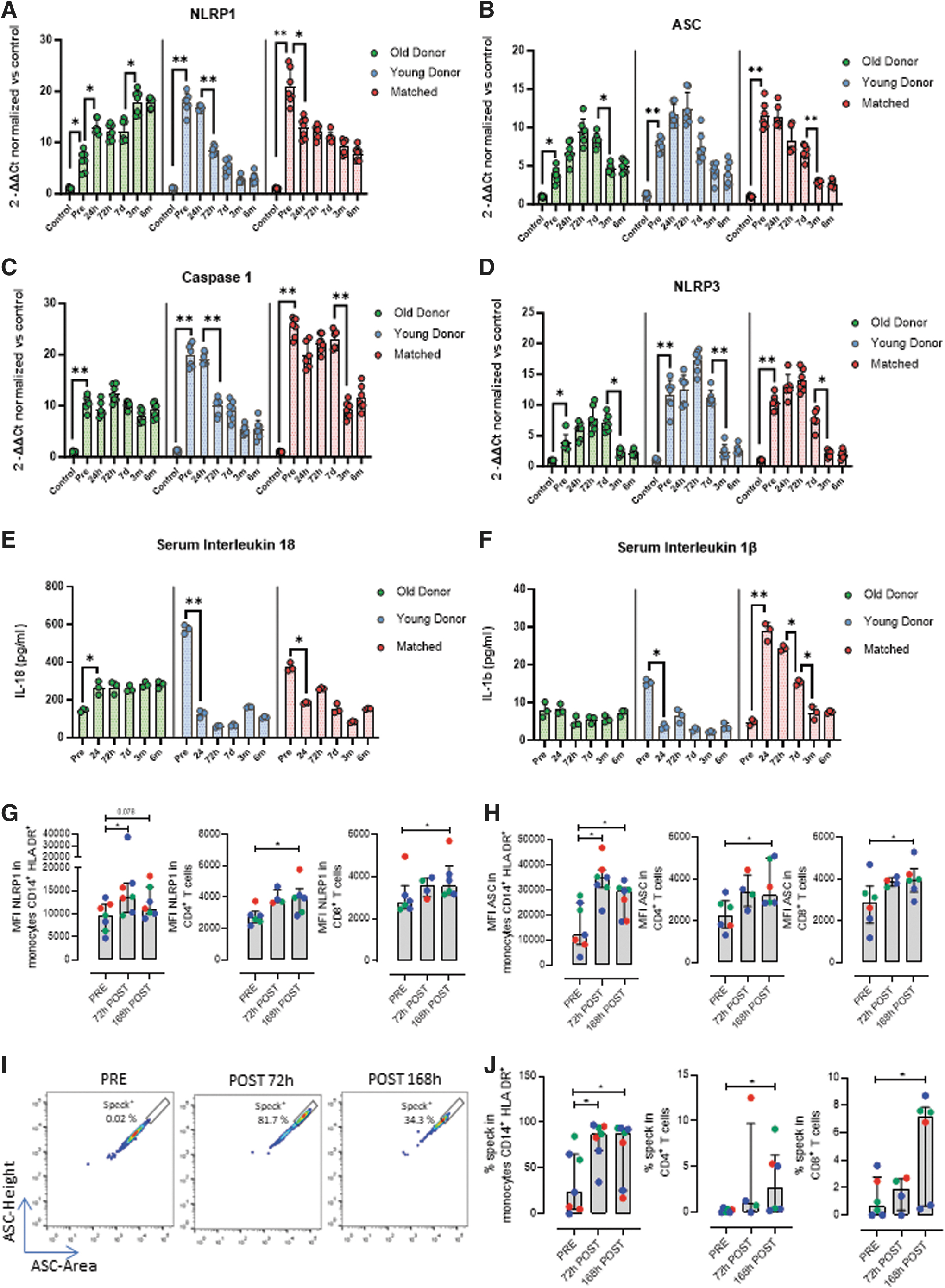
To test whether the inflammasome was active in patients, we checked for canonical IL-18 and IL-1β release in patient serum at the same time points when gene expression was measured. IL-18 remained stable over time, except in patients receiving younger kidneys, where it was reduced (Fig. 2E). IL-1β followed the same pattern as IL-18, but patients in a similar age group had high levels of IL-1β (Fig. 2F). This is possibly because of the higher mean age of this group of patients. This finding suggests that patients may benefit from a younger kidney.
To further confirm our findings about the activation of the inflammasomes after kidney transplantation, we studied by flow cytometry the expression of their components. For that, we built a panel to assess the expression of the proteins NLRP1, NLRP3, and ASC in different immune populations, including CD4+ cells, CD8+ cells, and monocytes. We found that NLRP1 was expressed in nearly all monocytes, CD4+ and CD8+ T lymphocytes. The expression of NLRP1 increased after transplantation, with higher mean fluorescence intensity (MFI) signal in CD14+HLA-DR+ monocytes, CD4+ and CD8+ T cells, 72 h and 7 days (168 h) after transplantation, respectively (Fig. 2G). A similar pattern was observed for the expression of ASC, slightly increasing the frequency (%) of positive cells after transplantation, and also significant changes in the content of this molecule (MFI) in the different immune populations studied at all time points (Fig. 2H). Remarkably, these analyses showed a strong activation of the inflammasome after transplantation, as a measure of a higher pulse height to area (H:A).
Moreover, we assessed the inflammasome formation by flow cytometry. The adapter molecule ASC can recruit caspases when oligomerized and forming the reported speck inflammasome structure. The accumulation of ASC in the speck can be detected using the time of flight signal of ASC for studying this in the different immune cells. Remarkably, these analyses showed a strong activation of the inflammasome after transplantation, this was more evident for monocytes, but also detected in CD4+ and CD8+ cells 168 h after transplantation (Fig. 2J). Overall, our data show higher levels of NLRP1 protein induced after transplantation as well as evidence for ASC oligomerization, supporting the idea that the NLRP1 inflammasome is active after kidney transplantation.
Discussion
Although there have been advancements in the short-term success of organ transplantation, the long-term survival of the grafts continues to be a challenge in kidney transplantation. In this article, we demonstrate a persistent activation of the NLRP1 inflammasome in renal transplanted patients. Of note, young patients who receive older organs exhibit increased NLRP1 inflammasome activity and expression at the cellular level. This phenomenon could be related to inflammaging. This condition is defined as a basal state of inflammation that rises with age, may be transferred through organ transplantation. NLRP1 expression displayed the most notable differences and a relation with donor age, although NLRP3 is the most extensively studied inflammasome. Traditionally, NLRP1 has been recognized as a sensor for pathogen detection, such as bacterial toxins (Chavarria-Smith and Vance, 2015). Our findings reveal a new potential role of the NLRP1 inflammasome in organ rejection.
Immunosuppression may mask the NLRP1 activity in immune cells, but it may still occur in other cells, ultimately leading to damage to the new organ and related processes over time. Conversely, old patients who receive a younger organ showed a progressive decrease in their inflammasome expression levels. A better renal function and immunosuppressive treatments may delay inflammaging. Patients who receive kidneys of similar age also exhibited similar improvement and stabilization, but do not reach the parameters seen in patients who receive younger organs. Our findings revealed that all patients exhibited increased expression of inflammasome-related proteins before the transplant. These results suggest that the anti-inflammatory effect of immunosuppressants is primarily achieved through immune system suppression rather than direct inflammasome inhibition. This has potential implications in the long-term failure of the transplantation process. This pretransplant condition is particularly noticeable when considering the age of the patients.
Young recipients (22–44 years old) displayed lower baseline inflammation compared with older patients (60–78 years old), which may be attributed to the aging process. However, after transplantation, younger patients who received an older organ showed progressive increases in proinflammatory markers, whereas the opposite effect was observed in older patients who received a younger organ. In the Matched group, where the donor and recipient were of similar age (∼60 years old), inflammatory markers remained stable, likely because the organ itself was already aged. Therefore, considering these perspectives, the conventional immunosuppressant treatment may not effectively inhibit the overall proinflammatory processes in the organism.
Multiple immunosuppressive agents are given in large doses after kidney transplantation to reduce the incidence of acute rejection to near zero. For instance, tacrolimus, a macrolide antibiotic produced by the soil fungus Streptomyces tsukubaensis, inhibits T-lymphocyte signal transduction and IL-2 transcription. Because macrolides can be perceived as toxins, tacrolimus may activate NLRP1, which would trigger its proper inflammasome. Unfortunately, there is no literature on the relationship between NLRP1 and tacrolimus.
In general, the availability of inflammasome inhibitor molecules is limited, and the extensive involvement of the NLRP3 inflammasome in a wide range of diseases makes it therapeutic target. The most widely recognized inflammasome inhibitor is MCC950, which operates by blocking the caspase-1–dependent processing of IL-1β. It also hampers both canonical and noncanonical activation of the NLRP3 inflammasome. In relation to kidney transplant, MCC950 reduces allograft damage in rat kidney transplants by mitigating the consequences triggered by prolonged ischemia, such as tubular damage (Zou et al., 2020). However, this study solely focused on the initial hours after transplant, during which NLRP3 activity was also observed. Unfortunately, MCC950 exclusively targets the NLRP3 inflammasome and does not inhibit the activation of NLRP1 inflammasomes (Wu et al., 2020).
Our results, showing a significant role of NLRP1 at later stages of kidney transplantation, are tempting to speculate that targeting this inflammasome represents a promising approach to increase the long-term success of organ transplantation. Unfortunately, there are currently no efficacious inhibitors for the NLRP1 inflammasome. The identification of a potential NLRP1 inflammasome inhibitor could introduce a new dimension of treatments not only for kidney transplant but also for numerous other diseases.
We also suggest that immunosuppressants alone may not be sufficient to prevent graft rejection long term. Accumulation of proinflammatory conditions in immune and nonimmune cells could lead to serious consequences. Although NLRP1 activation was predominant in our assays, no clinical trials have tested NLRP1 inhibitors that could work for organ transplantation patients. Further research into the inflammasome and its role in inflammaging will help us develop new drugs and treatments for organ transplantation patients.
Limitations of the study
Despite the relevance and novelty of our results, we recognize some limitations of our study. First, many of our results are derived from the blood of the transplanted patients. Thus, most likely, more notable results would be obtained in case of having the possibility to study the immune environment and inflammation in other tissues. Second, the confirmation of our results in larger cohorts is also desirable. We are trying to increase the repository of these precious samples. Third, the study of the inflammasome components and its activation at longer times after transplantation would be very informative, also studies about its association with other pathologies related to age or persistent inflammation. Thus, further research on this topic is warranted.
Notes
Biological samples
Ethical statements
Approval of the ethical committee of the Hospital Puerta del Mar was obtained, according to the principles of the Declaration of Helsinki and all the International Conferences on Harmonization and Good Clinical Practice Guidelines. All the participants in the study gave their written informed consent before initiating it.
Kidney transplanted patients were recollected from Puerta del Mar Hospital between January 1, 2021 and January 9, 2022 who received a kidney transplantation from young (mean age: 45 years) and old donors (mean age: 60 years). We performed a preimplantation biopsy in all kidney grafts. All patients had a minimum follow-up of 1-year after kidney transplant.
An immunosuppression regimen was administered to kidney transplant recipients to prevent rejection episodes and loss of the renal allograft. The components were tacrolimus, myphenolate mofetil, steroids, and basiliximab/thymoglobulin.
Kidney biopsy samples of the upper pole of the kidney graft were taken by expert nephrologists using the 16-gauge biopsy under ultrasound guide. All kidney biopsies were processed by standard techniques for light microscopy and immunofluorescence. Renal tissues were fixed in 10% neutral-buffered formalin and embedded in paraffin. The processed sections were 5 μm each.
Blood samples were collected at various time points: before transplantation, as well as at 24 h, 72 h, 7 days, 3 months, and 6 months post-transplantation. Peripheral blood mononuclear cells (PBMCs) were obtained from patients' blood using Histopaque 1077 (Sigma-Aldrich, San Lois, MO). Protein and RNA were obtained from patient PBMCs using the AllPrep RNA/Protein Kit (Qiagen, Hilden, Germany).
Selected patients
See Table 1.
Selected Patients
DBD, Donation after Circulatory Death; DCD, Donation after Brainstem Death.
Reagents
Bovine serum albumin (BSA; A7030) and Triton X-100 (X100-100ML) were purchased from MERCK (Darmstadt, Germany). The following reagents were obtained from Thermo Fisher Scientific (Waltham, MA): Secondary Alexa Fluor 488 goat anti-rabbit antibody (A-21424), QuantumRNA™ Classic 18S Internal Standard (AM1716), and secondary Alexa Fluor 555 goat anti-mouse antibody (A-21424).
Anti NLRP1 antibody was purchased from Abclonal (A16212; Woburn, MA).
Flow cytometry antibodies: The following antibodies were obtained from Becton Dickinson (Franklin Lakes, NJ): anti-CD56-FITC (B159, 562794), anti-CD3-PE-Cy7 (SK7, 557851), anti-CD14-APC-H7 (M5E2, 561384), and anti-CD4-BV605 (RPA-T4, 562658). Anti-HLA-DR-PE-Da594 (L243, 562617) and anti-ASC-PE (HASC-71, 653904) were purchased from Biolegend (San Diego, CA). Anti-NLRP3-AF700 (768319, IC7578N) was from Bio-Techne (Minneapolis, MI), and anti-NLRP1-AF647 (B-2 sc-166368) was from Santa Cruz Biotechnology (Santa Cruz, CA).
Cell phenotyping by flow cytometry
PBMCs were stained with LIVE/DEAD fixable aqua dead cell stain (L34966; Thermo Fisher Scientific) for 20 min at room temperature (RT). After washing once with phosphate-buffered saline (PBS), cells were fixed and permeabilized with fixation/permeabilization solution (554714; Becton Dickinson) for 20 min at 4°C and washed with BD Perm/Wash buffer. Then, cells were stained with antibodies for 20 min at RT. Finally, cells were washed with BD Perm/Wash buffer. Samples were acquired on a BD FACSCelesta flow cytometer and data were analyzed using FlowJo V10 software. Gating was performed according to the different fluorescence minus one controls.
Immunofluorescence
Immunofluorescent staining of paraffin-embedded sections was performed following standard methods. Paraffin sections were attached to superfrost plus slides (Menzel-Glaser, Braunschweig, Germany) at 60°C for 1 h. Deparaffinization was performed by pure xylol washes 3 times for 10′ each. Slides were rehydrated by ethanol solutions immersion (from 100% to 70%) for 5′ each and rinsed with deionized water. For the heat antigen retrieval, slides were immersed in sodium citrate 10 mM (unmasking solution) and microwaved at 800 W for 15′, and then samples were kept at RT until cool down. Slides were rinsed with PBS 1 × 3 times, and then blocking solution (2% BSA, 0.05% Triton X-100 in PBS 1 × ) was applied for 1 h. The samples were surrounded with a hydrophobic barrier using a barrier pen and primary antibody was applied at 1:100 concentration diluted in blocking solution overnight. The next day, slides were rinsed 3 times with PBS 1 × and secondary antibody was applied at 1:400 concentration diluted in blocking solution for 2 h. Again, slides were rinsed 3 times with PBS 1 × and 4′6-diamidino-2-phenylindole (sc-3598; Santa Cruz Biotechnology) staining (1 μg/mL) was applied for 10′. Finally, samples were mounted with coverslips in using Vectashield Mounting Medium (H1000; Vector Laboratories, Burlingame, CA).
IL measurement
ELISA kits IL-18 (ab215539) and IL-1β (ab214025) were purchased from Abcam (Cambridge, United Kingdom). Assays were performed using patient blood serum according to manufacturer protocol.
Gene expression
Expression of NLRP1, NLRP3, ASC, gasdermin, and caspase 1 were analyzed by SYBR Green (RR420W; Takara, Kusatsu, Japan) quantitative PCR (qPCR; Table 2). Complementary DNA was obtained from extracted messenger RNA using the iScript cDNA KIT (Bio-Rad, Hercules, CA). The qPCR was performed in a CFX96 Connect Real-Time PCR Detection System (Bio-Rad). Ribosomal 18S expression was used as reference gene. 2−ΔΔCT method was used as a relative quantification strategy for data analysis. This method is a convenient way to calculate relative gene expression levels between different samples in that it directly uses the threshold cycles generated by the qPCR system for calculation.
Gene Expression
Statistics
Nonparametric Student's t-test (Mann–Whitney) was used to compare data between two groups. The Mann–Whitney U test does not rely on the assumption of normal distribution in the data. It is particularly useful when dealing with ordinal or interval data that may not meet the normality assumption required by parametric tests. It can be applied to a wide range of data types, including ordinal, interval, and some ratio data. The test is robust against outliers and skewed data, making it a good choice when dealing with datasets that may have extreme values. The Mann–Whitney U test is sensitive to differences in both central tendency and shape of the distribution, making it versatile for various types of comparisons. The test assumes that the observations in one group are independent of the observations in the other group. If this assumption is violated, the results may be invalid. It assumes that the shapes of the distributions in the two groups are similar. If the shapes are substantially different, the Mann–Whitney U test may not provide an accurate assessment of differences. Finally, the test may be less accurate when there are ties in the data (i.e., multiple observations with the same value). Some adjustments or corrections may be necessary in such cases.
All results are expressed as mean ± standard deviation of three independent experiments and a p value <0.05 was considered as statistically significant. Level of significance is denoted by asterisks *p < 0.05, **p < 0.01.
Footnotes
Authors' Contributions
M.D.C. and A.M., designed the study. J.M.S.R., J.L.P., and I.M.Z. performed the experiments. A.A.G., performed flow cytometry experiments. R.V.M., A.A., T.G. A.N.D., and A.M. performed the patient selection and according to the protocol of transplant from the Hospital. J.M.S.R., J.L.P., A.M., and M.D.C. discussed and analyzed the data. M.D.C. and J.M.S.R. drafted the article. All the authors revised the article and approved the final version.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. All patients gave informed consent to use leftover blood for research purposes. Blood samples from healthy volunteers and patients were approved by the Ethical Committee of the Hospital Puerta del Mar.
Consent to Participate
The participants gave informed consent to participate in the study.
Consent for Publication
The participants gave informed consent for publication.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential competing interest.
Funding Information
This study was supported by PI21/01656 grant, Instituto de Salud Carlos III, Spain and SATOT fellowship, Spain. JMSR has the benefit of a Postdoctoral Fellowship (RH-0085-2021) from Consejería de Sanidad, Junta de Andalucía, Spain. AAG has the benefit of a Juan de la Cierva Fellowship (FJC2021-047304-I) from The Ministry of Education, Science and Sport.