
Abstract
Background:
Older autistic people in the United Kingdom are facing a social care crisis. Autistic people are more likely to need social care as they age, but little is known about the architectural needs of autistic people, meaning current residential care facility design makes this form of social care inaccessible to them. Older autistic people often have to rely on fragile informal care or are placed in unsuitable social care situations such as long-stay hospital wards. In contrast, there are established gerontological best practices for designing residential care for older people. This article discusses how the residential architectural needs of autistic people and gerontological residential care design best practices may conflict.
Methods:
One hundred and five autistic people answered an online questionnaire asking about their architectural needs and preferences. Qualitative results were analyzed using reflective thematic analysis with an inductive approach, and quantitative results were described and tested for statistical significance where appropriate.
Results:
The research identified three themes where there may be conflict between the architectural needs of autistic people and gerontological residential care design practices: sensory challenges, interactions with others, and day-to-day life. Elements within these themes could make buildings inaccessible to autistic people, cause sensory overload, cause distress, or negatively impact their executive function and ability to complete daily tasks.
Conclusions:
Certain aspects of residential care design that may positively influence older people’s well-being and quality of life may cause autistic people distress and discomfort and inhibit their ability to undertake daily tasks. Some of the elements that may cause this dichotomy are the building location and connectivity, building and spatial size, navigation and wayfinding, open plan flexible spaces or distinct separate spaces, spatial interconnectivity, the extent of the private domain, and social space design. Further research is needed on how to overcome these conflicts.
Community Brief
Why is this an important issue?
Older autistic people are more likely to need social care than older non-autistic people. We don’t know much about the best way to design buildings for autistic people. The design of residential care buildings might stop autistic people moving into them. This could stop autistic people accessing social care when they need it.
What was the purpose of this study?
We looked at whether the best way to design buildings for autistic people may be different from designing buildings for older people. Understanding those differences may help us design better residential buildings for autistic people.
What did the researcher do?
The researcher wrote a questionnaire and asked autistic people to answer it. The questionnaire was about what autistic people like or dislike about the buildings they live in. We looked for patterns in the answers. We compared those patterns with research on the best way to design residential care buildings for older people.
What were the results?
The autistic people who answered the questionnaire wrote about how they wanted to live somewhere quiet. They said that they didn’t want to live near other people. They did not want to live with other people who had different lifestyles and needs. They also said too many other people and sensory discomfort may stop them being able to enter a space. They did not like being forced to socialize. They need to be able to leave a space when there are too many people in it. They wanted there to be enough space between people. They said that having to use shared spaces may stop them being able to cook, eat, exercise, and wash. They said that they would find it hard to use rooms that had several different uses or where the layout could change. They said their home is their safe space.
What do these findings add to what was already known?
These findings help us know more about what autistic people like or dislike about the buildings they live in. They also help us know which parts of residential care building design autistic people dislike.
What are potential weaknesses in the study?
We did not know much about this topic before doing the research. This made it harder to know how to do the research. It would have been better if more autistic people had answered the questionnaire. It would have been better if more different types of people answered the questionnaire.
How will these findings help autistic adults now or in the future?
This research will help people design residential care buildings in a way that is better for autistic people. It helps us understand why they like or dislike parts of a building’s design.
Background
The United Kingdom is facing a social care crisis regarding the care of older autistic people. Autism has a similar prevalence across the lifespan, 1 but many older autistic people are part of a “lost generation” 2 (p13) who are undiagnosed. Autistic people are more likely to need social care 3 and have co-occurring conditions, such as mental ill health, cardiovascular disease, respiratory disease, and cancer,4–6 compared with neurotypical people.
In 2017, the main form of long-term care for older autistic people in the European Union (which at the time included the United Kingdom) was informal familial care, 7 (p15) including care from elderly parents who may be facing their own issues with aging. 6 (p329), 7 (p15) This creates a fragile system of care where “The potential for sudden breakdowns in caring arrangements is high” and autistic people may be “hurriedly placed in settings that may be expensive, distant, inappropriate, or all three.” 8 (p37) Autistic adults often get lost in the social care system, especially those without co-occurring intellectual disability or mental health issues. 9 (p34)
The needs of older autistic people
Only 3.5% 10 to 15% 11 of research on autism includes or focuses on autistic adults, and only 0.4% specifically focuses on the needs of older autistic adults, 12 (p164) meaning there is little information available to autistic people on their own aging trajectory. Michael 13 (p515) states, “We know virtually nothing about what happens to us, autistic people, physically, cognitively, emotionally and socially as we pass through middle and older age.” Autistic people are worried that, if they need to enter geriatric residential care, there will be no adjustments for their autism, no specially trained staff, and no understanding of autism in general. 14 There are theories that autism may protect from age-related decline, create a “double jeopardy” when combined with aging, or that autistic and non-autistic people’s aging trajectory is parallel, 15 (pp666–667),16–20 but the research is inconclusive as to which autistic characteristics follow which theory. The exact impact of external factors, such as smaller initial social circles, 21 (p76) higher rates of co-occurring conditions,4–6 and use of antipsychotic medication, 21 (p71) is also unknown.
Building design and autistic people’s well-being
Building design can have a direct impact on autistic people’s quality of life and well-being, 22 (p6),23(p64) with natural light, sound proofing, appropriate ceiling heights, and quiet but efficient air conditioning and ventilation, all having a positive influence. 24 Autistic people’s heterogeneous sensory differences affect how they process the indoor environment,25,26(p14) and personalized designs in response to these needs could help. 26 (p15) However, autistic people are “usually ignored in design,”27(p3) as architects and social care providers are typically unaware of autistic people’s architectural needs and the affect different architectural elements can have.28(p21),29 This means that autistic people often inhabit environments that are “designed exclusively to meet the needs of neurotypical populations”30(p1904) where sensory needs are ignored,31(p4) which places constraints on autistic people32(p1) and may negatively impact their mental health and well-being.33(pvii)
Existing architectural design recommendations for autistic people
Most existing research on the architectural needs of autistic people focuses on autistic children’s schools
26
and/or residential care environments, stating that autistic people need:
To live in quiet, supportive, well-connected neighborhoods that offer social opportunities22 (pp15–16),28(p27),34(p16),35(p179),36(p35) Private single bedrooms with ensuites and communal living/functional spaces27(p141),28(p36),34(p30),37(p43) in dwellings shared with two to eight other residents22(p11),28(p24),34(p21) Flexible spaces to enable different uses and meet the needs of different residents and staff22(pp26,27,28,30,31(p33),34(p23) Sensory cues to aid navigation and spatial intelligibility22(pp17),19,27(pp102–104),29,34(p25),37(p44) Opportunities for socialization,22(pp11,30),27(pp104,108),28(p24),34(p6),38(p8) including finding ways to force the “least social to interact at least once a day”28(p33) Sensory rooms, escape spaces, and “sensory neutral” or “sensory calm” environments, 22,27(pp110,168),28(p31),29,31(p32),32,34(p23),37(pp43–44) or environments that force autistic people to “build tolerance” to sensory to sensory discomfort26(p8),39,40 Either open plan27(p108),29 or single-use separate spaces24(p5),27(p183),34(p22),37(p43) or a mixture of open plan and separate spaces35(p184)
Building design and older people’s well-being
Residential care facilities that are homelike and enable personalization likely result in a higher quality of life.41–43 Other recommendations include design that promotes socialization,41,42,44–49 a well-connected location,42(pp240–242),50(p681),51(p90),52(p631),53,54 a single-story building with a variety of spaces,42(pp242,251)55(p14),56(pp667,674) flexible multiuse communal spaces,57,58 distinctive sensory cues,41,42,51,52,58,59 good lighting and access to daylight,41(p781),42(pp250–251),43(p114),60 open plan layouts,42,51 green outdoor space,41(p782),42(p251),61,62(p115),63,64 and privacy and enablement.41(pp782–784),44(p22),45(p255),46(p12),57(p196) Design for older people must consider the needs of those with cognitive differences, such as those with Alzheimer’s, who would specifically benefit from rich sensory environments,41(pp781–782),62(p114),65 spatial cues that help remind residents of where and who they are,41(pp780–781),66(p725) clear boundaries between public and private spaces,58(p143) visually uniform floor surfaces,63,67 easy-to-navigate environments with no dead ends,42(p240),46(p9),59(p38) large windows,68(p1258) and access to gardens.54(p53)
This article discusses how the architectural needs of autistic people living in the United Kingdom may conflict with gerontological residential care facility design best practices, which may stop autistic people accessing age-related residential social care.
For this project, older autistic people are defined as an autistic person over the age of 50, due to International Society for Autism Research’s 69 recommendation that autism and aging research should focus on adults over the age of 50, and the reduced life expectancy of autistic people, 70 meaning that they are less likely to reach existing thresholds for old age.
This article was written as part of a larger PhD research project, asking “How can the architectural design of residential care facilities in the UK be improved to make them more suitable for older autistic people?”, and will only report results that are relevant to this discussion.
Methods
The researcher created a pilot study online questionnaire and a main study online questionnaire, with a grounded theory (generating theories from data) 71 (p329) approach. The researcher used this approach due to the limited existing theories regarding autistic people’s architectural needs and preferences and due to autistic voices often being absent in autism research.72,73 The original design of this project included a card-sorting activity for use with autistic participants already living in residential care; however, due to post-pandemic staffing issues, the research partner organization that would enable this had to withdraw from the project. The pilot study questionnaire was global, and responses had statistically significant differences based on geographic location; therefore, the main study questionnaire was limited to UK participants.
Questionnaire development
The researcher used an iterative design process with feedback from autistic and non-autistic volunteers, to ensure the questions were written in an accessible and nontechnical manner. The main study questions were written in the easy-read style outlined by the Autistic Self Advocacy Network, 74 such as “one idea per line,” using short sentences, and defining any uncommon words. The researcher provided participant information and consent in full-text and easy-read formats. Two extensive literature reviews informed question content and format, and pilot study responses were used to refine the main study content. The main study questionnaire investigated the architectural needs and preferences of autistic people regarding their home and residential care environments. The questions were separated into six categories, based on themes identified from pilot study responses as priorities for autistic people: Sensory preferences; Daily Activities; Socializing; Special Interests and Hobbies; Accessibility and Ideal Dwelling; and Communal Living. Figure 1 summarizes these question categories and their content. Participants were given the following definition of communal living within the questionnaire:
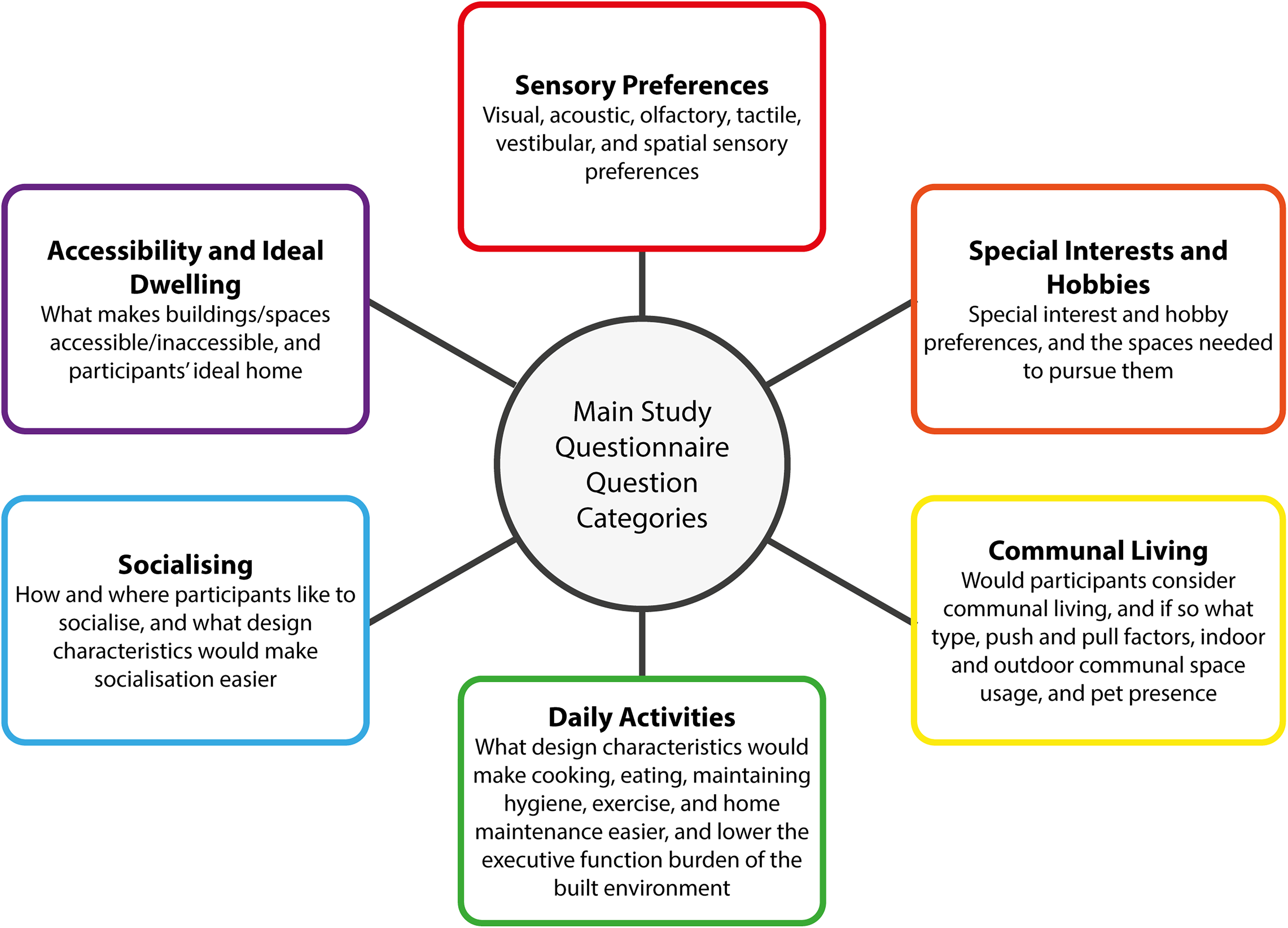
The main study question categories and category content summary.
Communal living is when you live with a group of people.
You may live in the same building or different buildings.
You may or may not know these people before deciding to live with them.
You may share a house with other people.
You might have communal spaces that you share with these other people, such as an exercise space or a cafeteria.
Recruitment and participant demographics
The researcher recruited participants through convenience [participants most conveniently available71(p396)] and snowball sampling [participants help recruit subsequent participants71(p406)] methods via social media, academic institutions, and autism charities and organizations. One hundred and five autistic participants who lived in the United Kingdom responded, but not all participants answered every question. Eighty participants were formally diagnosed, and 25 were self-diagnosed. Self-diagnosed participants were included in this research project, as there are known gender, financial, and racial barriers to autism diagnosis,75–77 as well as research that indicates there are no significant differences with regard to autism identity, stigma, quality of life, and self-esteem between the self-diagnosed and the formally diagnosed. 2 Due to disagreements regarding the academic validity of including self-diagnosed people in autism research, the researcher tested for statistically significant differences between the self-diagnosed and the formally diagnosed datasets. Statistically significant difference was only found in 10 out of 192 variables (5.2%), suggesting it is valid to include self-diagnosed autistic people in research addressing the architectural needs of autistic people. Full demographic data can be found in Supplementary Appendix SA1.
The researcher received ethical approval from the Cardiff School of Art and Design Research Ethics Committee.
Quantitative questions and analysis
Quantitative (information that can be represented by numbers) questions presented participants with a range of variables, such as different surface textures, or different things that may help with daily activities. Three answer sets were offered:
Yes, maybe, or no; or I like, I don’t mind, or I dislike; or Would help, wouldn’t make a difference, or would make it harder
It was hoped that using a narrow range of selectable choices, in a format that repeated throughout the questionnaire, would reduce the chance of decision fatigue for participants.
The researcher described quantitative data and, where appropriate, tested it for statistical significance using chi-square tests,78(p86) Fischer’s exact test,78(p88) and the Fisher–Freeman–Halton Exact test. 79 The researcher used statistical significance testing to check the validity of including self-diagnosed people in autism research, as discussed above, and to ascertain whether younger respondents could be used as a reliable source of information on the architectural needs and preferences of autistic people aged 50 years and over. Statistically significant differences were found in only 6.25% of all variables, meaning it is likely that younger autistic people are reliable sources of information on the architectural needs and preferences of older autistic people.
Qualitative questions and analysis
Most quantitative questions were followed by an optional qualitative (information and concepts not represented by numbers), free-text question to allow participants to expand on their answers.
The researcher used reflexive thematic analysis (a flexible, systematic approach to analysis that critically values the researcher’s subjectivity) 80 with an inductive (constructing theories from the data)71(p22) approach. The researcher coded data at a semantic level, as autistic people often prefer more literal methods of communication, through the lens of critical realism (an acknowledgment of the existence of realities that cannot be observed). 81 Critical realism is vital in autism research as the heterogeneity of autism likely means there cannot be universal truths regarding the lived experience of autistic people. The approach to the thematic analysis was iterative and involved familiarization with the data, initial coding, and then a cyclical process of revision and refinement before arriving at the final themes, similar to the method outlined by Nowell et al. 82
Question example
A question example is shown in Figure 2, where participants were asked, “What kind of space do you like to socialize in?” and were then given a range of options to which they could respond “I like,” “I don’t mind,” or “I dislike.” The free-text qualitative question shown afterward allowed participants to discuss their preferences further.
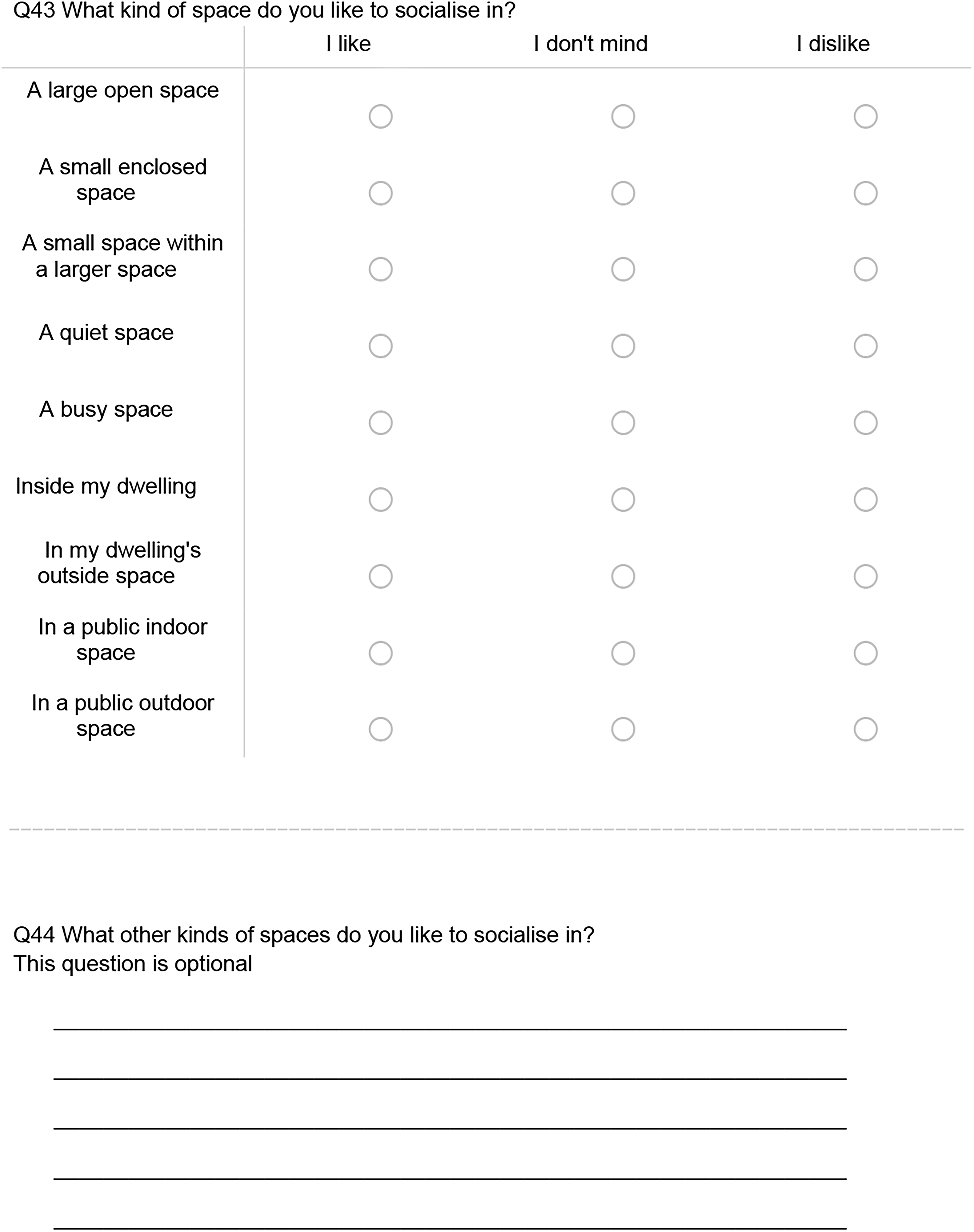
An example of the question format used throughout the questionnaire.
A full list of questions is reported in Supplementary Appendix SA2.
Results
The researcher identified questionnaire response themes and compared them with existing gerontological residential care design best practices. Conflicts were found in three areas: sensory challenges, interaction with others, and day-to-day life. The results relevant to these themes are reported below.
Sensory challenges
Quiet and calm location
Participants wanted their homes to be “in the middle of nowhere” or “in a field away from everyone” and highlighted the importance of their dwelling’s proximity to nature, they also wanted to live “somewhere surrounded by woodland, a small stream” or with “just wildlife around me,” enabling “views out to natural areas.” A key factor in this desire for a rural or remote location is the need for quiet. Participants wanted their dwelling to be located somewhere “peaceful,” “away from main roads or nighttime activity spots,” and for there to be “no sirens.” Participants repeatedly discussed disliking man-made sensory stimuli, including stimuli caused by neighbors who had “bonfires and barbecues all the time” or who could be heard from participants’ private space. The sensory and social distance of a quiet and calm location could improve autistic people’s well-being by preventing causes of discomfort.
Sensory inaccessibility
Participants reported that sensory discomfort would make a space inaccessible to them.
Participants reported needing the environment to be “not visually cluttered” and not “busy” with furniture and pictures, as “cluttered spaces make it not accessible.” This included not wanting “busy artificial patterns.” Seventy-five percent of participants (n = 88) reported that plain and simple decorations and colors would help make a building accessible to them and be “neutral and calming,” whereas “bright” or “harsh” colors would make a space inaccessible. There also needed to be “no fluorescent lighting,” and lighting needed to be adjustable and “not too bright”—when asked, 90.2% of participants (out of n = 102) disliked bright lights. Some found colored lights soothing, whereas they made others “feel nauseous.” This is supported by the quantitative data: out of n = 102 responses, 41 (40.2%) said they would like colored lights, 32 (31.4%) said they don’t mind colored lights, and 33 (32.4%) said they disliked colored lights. The visual aspect of signposting also affected accessibility. While “good quality signage helps,” “too many signs” or “heavily signed intersections” made spaces inaccessible, and picture-based signage was “often hard to interpret.” Spaces with a limited number of muted visual inputs were reported to be most accessible.
Certain sounds could also make spaces inaccessible: 90.9% of participants (out of n = 88) said that stopping noise and echoes travelling around the building would make it more accessible to them. Participants discussed specific noises, such as high-pitched noises, loud noises, unexpected noises, beeping, background music, and doors slamming; 78.4% of participants (out of n = 102) said they disliked household electronic noises, and one described them as “awful.” These sounds had a negative mental and physical impact: “negative sounds can make my heart race, disturb thought patterns, communication, my ability to stay calm.” Participants need the sound in their built environment to be well managed.
Some participants mentioned the need for “odour reduction aids” and how “windows that don’t open enough to get a flow of air to remove smells” would make a space inaccessible. The type of smells also seems important, with “artificial smells” being disliked as they smell chemical, with one person stating that artificial flora smells were like “chemically laced flowers.”
Spaces that are too warm can be inaccessible to autistic people: “I really struggle with temperature and ventilation—warm enclosed spaces sometimes make me anxious enough that I can’t get in at all.” This can be improved with “windows you can open” and “temperature control.”
Spaces could be made more accessible to autistic people with good sensory control of a limited number of muted sensory inputs.
Sensory challenges of social spaces
Participants were specifically asked about what kind of building design could help them socialize. The most common concern was a sensory one. Participants stated that social spaces needed to be quiet and “prevent echoing noises. That is the biggest blocker to talking in some environments.” Others stated there needed to be “no background noise” and the space needed to “try and minimise the distance sound travels” with “sound absorbent surfaces.” This is supported by the quantitative results, where 83.9% of participants (n = 93) reported liking quiet spaces to socialize in.
Visual concerns included the space being “light, but not bright” and using natural lighting to “prevent the space feeling too cramped.” Participants discussed avoiding “repetitive patterns in furniture or fabrics” and having “plain floor colouring.” One person said social spaces should “avoid strong colour contrasts in general, prefer pastel tones if you need to use colours; but prefer hearty, natural materials over colours (wood, whites, beiges, stone, concrete).”
Some participants wanted a “consistent and comfortable temperature” with “good ventilation” and an environment that is “non-draughty.”
Participants stated that these sensory considerations could help create a calmer/comforting/homely space, with natural materials providing a “relaxing atmosphere”, and that “lots of comfy sofas and beanbags” would help the space feel “homely and welcoming.” The added sensory input that socializing creates requires social spaces to offer sensory calm.
Sensory challenges of open plan and shared spacesv
Open plan or multiuse spaces also pose a sensory barrier and make it hard for autistic people to use them. Spaces that have “lots of overlapping noises” create sensory issues: “A large open space can be nice but if you want to simply move a chair and it makes a huge echoing scraping noise that would be uncomfortable.” For buildings to be accessible, they need to have “enough separate spaces that they could get away from the sensory input created by others when necessary.” Shared spaces also brought additional sensory challenges. One participant said “that too many voices in a space have all necessitated me leaving places”; and another said, “People actually irritate me, the noises they make and not having patience to deal with it.” Another said they would be “disturbed by other people’s noise and smells.”
Interaction with others
Isolated location
Participants discussed how they would like to have a limited number of neighbors or “no neighbors” at all. Participants wanted their dwelling to be isolated to act as a “safe haven from the world” and to be “far enough from others so that they don’t disturb me and I don’t disturb them.” This would help prevent other people “dropping by unexpectedly,” which would, in turn, stop there being “pressure to do things with other people.” Participants wanted to be unperceived and have “the ability to arrive or leave unseen.” Some participants felt unsafe around other people, including neighbors, and a lack of isolation from neighbors made them “fear bullying or angry people.”
However, participants also mentioned the need for their dwellings to be “conveniently located for work and hobbies.” This would include provision for those who cannot drive: “being on regularly serviced bus routes matters.” Participants’ desire for remoteness was to limit uncontrolled interaction with other people; however, they still desired practical connectivity.
Other people making spaces inaccessible
The presence of other people creates an accessibility issue for autistic people. Several participants reported that a space being too “busy” or having “too many people” would make a building inaccessible to them. Too many people can be “intimidating.” For some, regarding accessibility, “mostly it’s about the other people in the building not the space itself. People tend to be inconsiderate and selfish.” When asked, 31.8% of respondents would not want their communal living facility to be open to the public, with one person saying, “Non autistic people treat us like animals to be stared at like an amusing attraction that enamours their deepest curiosities, without recognising the inhumanity of ‘othering’ us as lesser beings … I don’t want to have to deal with that should I want a pot of peppermint tea on a Tuesday.”
Other people can also negatively affect spatial navigation; the space is inaccessible if the person must “squeeze around large groups of people,” “interact with people to be able to access things,” is “too crowded to see signs,” or if routes to toilets are “blocked by groups.” “Quiet spaces away from large groups” and enough space so that two people can “pass at the same time without touching each other” can make spaces where there are other people more accessible. Spaces are more accessible if there is limited or no forced interaction with other people and enough space to enable comfortable distance between people. This is supported by the quantitative results, where 68.9% of participants (n = 103) say they liked larger rooms.
Differing lifestyles and needs
Respondents reported concerns about sharing space with “people with needs potentially extremely different” than their own, such as mess and disorganization, as other people’s mess “makes them stressed.” Other people were concerned about differing schedules, such as “being up late at night when other people are asleep,” if the environment is “super loud all the time” and “not having anything in common with the other people.” Another person would not want to live in a communal living situation where the other residents “wanted to socialise a lot.” Forced proximity to others with different needs and lifestyles would distress autistic people.
Pressures and challenges of forced interaction
Of those who would consider communal living (44 out of 88, 50%), 63.6% would not like to have a bedroom within a shared house. Participants disliked and feared forced socialization. Some participants reported that “too much sharing spaces,” “forced socialisation,” and “multiple people using facilities at once” would stop them moving into a communal living situation. Several people mentioned not wanting any kind of “forced interaction” or “forced socialisation”—they feared facing “pressure to socialise too much” and stated that “I would not want to be forced in to company when I need to be alone.” One person said, “I struggle with social interaction and need a lot of time to myself to process experiences and conversations, and to recharge. I find it difficult to balance those needs when I live with other people, and I get tired from masking at home.”
Some respondents disliked the social expectation that came with communal spaces; they “would not be able to relax as there would be an expectation to interact in the right way.” Some participants mentioned “pressure” or “obligation” to socialize, while others were concerned about rules around forced socialization. One participant said, “My anxiety would be awful, I would constantly be worrying if I was being fair, acceptable.”
Limit the number and proximity of people
Participants discussed needing there to be a limited number of people in their social spaces. Participants stated that it would be beneficial to have “private, separate spaces” and “designated rooms for only one/few groups to use at a time” that would help limit the number of other people in the immediate vicinity. Privacy was also raised: “tables in booths … so you can’t see other tables and they can’t see you easily.” Dividers or separation would also “split up the space to avoid large overwhelming crowds.” Some participants desired a space that had enough room to socialize and did not have “lots of tables squashed in” and instead had “enough seating indoors to allow for personal space.” Spaces that allowed for more privacy and greater distance between people were preferred.
Unpredictability and the need for escape
Some participants found other people’s unpredictability challenging and would not consider communal living as “communal living brings unpredictability” and other people’s “emotional volatility.” Participants discussed needing to be able to escape social situations: “easy escape spaces and places to go to feel safe and away from other people if I needed a break (kind of like priest holes in old buildings).” One participant said, “Breakout areas and quiet spaces would be brilliant,” and another stated they would like “cubby holes to escape.” The unpredictable nature of other people requires easy to access escape routes and escape spaces.
Day-to-day life
Daily activities
Participants reported that having to rely on shared or communal spaces for daily activities such as cooking, eating, exercise, or hygiene activities would make those activities harder or prevent them from undertaking them. One participant stated, “Other people get in the way and don’t do things the way I prefer them to be done,” and another said they needed their built environment to have “specific places for specific people, where I can organise a space in a way that helps me” to aid their executive function. Participants reported that having to share functional spaces with other people negatively impacted their executive function and that “no forced socialising through shared space with other households” and “control over whether other people are in the space or whether I enter a shared space” would help.
Several participants stated that having someone to cook for them would be of benefit, but, when the autistic person themselves had to cook and eat, they often would not want other people around. Other people brought sensory challenges, felt like “intruders,” and caused “pressure to clean up when I’m burnt out.” Other people also could make the kitchen dirty, and some found it “harder to cook when the kitchen isn’t clean.” For some, eating around other people was an issue: “I have made an advance statement that specifically says if I go into a care home, I can’t manage shared mealtimes. I can’t eat with the smells and sounds of others eating.” Another said, “Sounds other people make are sometimes okay except chewing.”
Exercise spaces were often “too full of people,” and strangers being able to see them exercise made them feel judged or self-conscious: “I am also very uncoordinated, so I do not like anyone seeing me exercise as it is potentially humiliating.” This is supported by quantitative data, in which 52.6% of participants (n = 97) stated that exercising with others would make it harder for them to exercise. However, for some, it depends on the day. One person said, “I enjoy the atmosphere of people at the gym although sometimes I wish they weren’t there.” One person enjoyed exercise more when “the space is how I want it, the music is the music I want and I can wear what I want without anyone seeing.”
Regarding hygiene, some autistic people “dislike anyone else using their bathroom” and reported that “other people being around” made hygiene maintenance harder and having to share bathrooms and would stop them entering communal living.
Having to use shared spaces for daily activities would make it harder for participants to undertake those activities, due to the greater executive function burden and sensory complexity of shared spaces, as well as not wanting to be perceived.
Challenges posed by open plan/multiuse spaces
Participants reported that using open plan or multiuse spaces would be “very hard” for them. Spaces that are “full of different functions” can create executive function issues and “separate areas for study, eating, relaxing etc. are helpful for focus.” One person stated, “I would never have a flat where the bedroom was also the living room.” Others wanted “clear functions for rooms” and said that to use multifunction rooms would stop them entering communal living.
Open plan and multiuse spaces risk layout changes, which can cause issues with predictability. Some autistic people need their environment to “remain the same layout” so that they can “do things mostly automatically.” One person said that being forced to use a space for multiple functions would be a barrier to them. Open plan and multiuse spaces pose sensory, executive function, and predictability challenges.
Home as a sanctuary
Several participants mentioned a need for their home to be their sanctuary, “a safe haven” where they “don’t let any ‘outsiders’ in” and they “feel safest from the vagaries of the world.” One participant said, “My home is my safe place … I won’t answer the door if not expecting anyone.” Others needed their home to be calm and offer sensory control. Participants’ feeling of sanctuary was dependent on sensory control, being able to control who is allowed in their home, and exclude the outside world, which allowed them to “be themselves fully” and meant “no masking.”
Discussion
The researcher compared findings from the study questionnaire with themes identified in the literature review on the needs of older people living in residential care, as well as existing research on autism and architectural design, identifying where the needs of the two demographics might conflict. The comparison suggests there are existing gerontological residential care architectural design practices that may negatively impact the day-to-day life of autistic people by creating sensory, social, and executive function challenges. Specific conflicts between the results of this research and existing gerontological residential care design best practices are summarized in Table 1.
Autistic People’s Architectural Needs and Preferences Versus Gerontological Design Recommendations
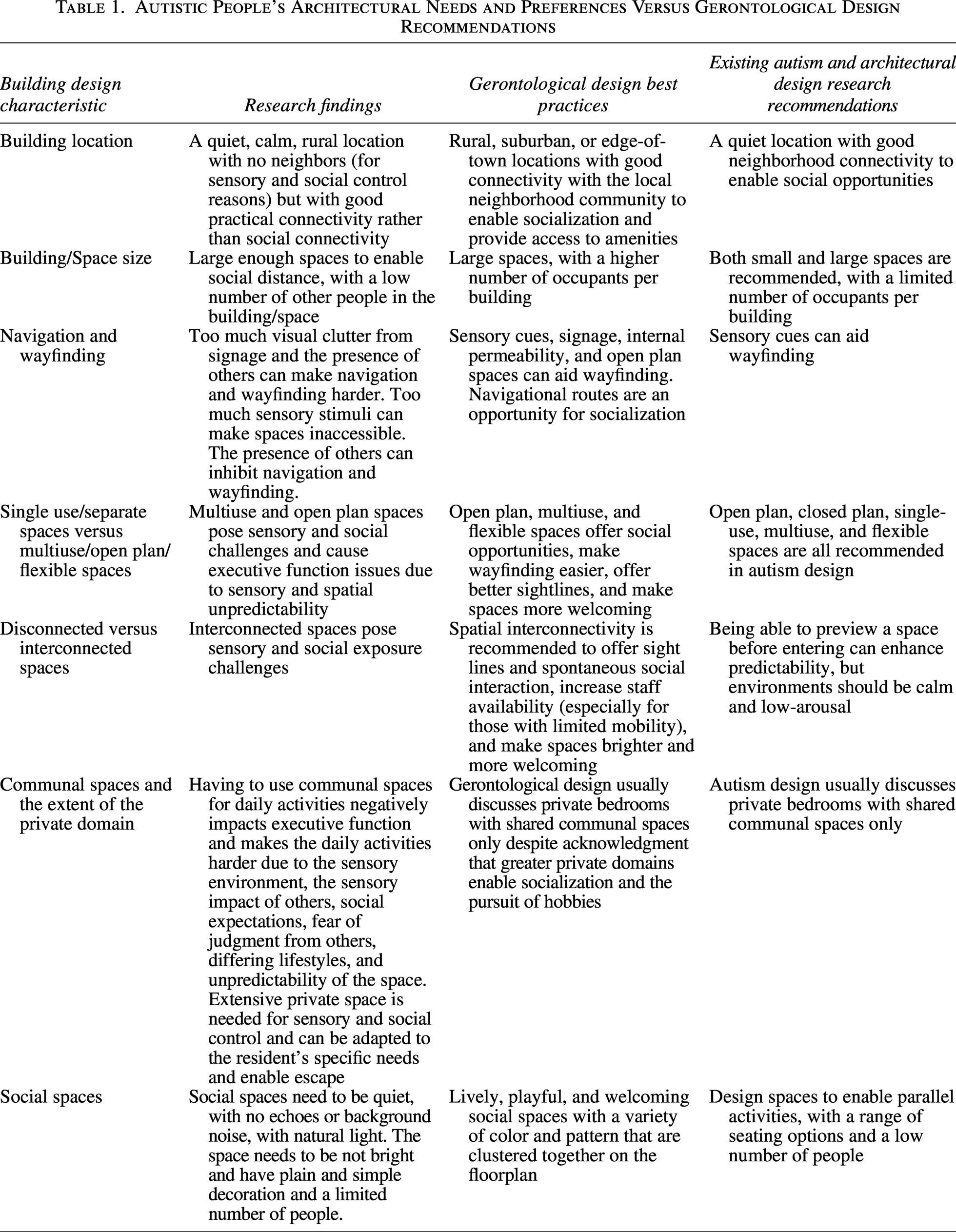
Building location
Older people seem to prefer rural, suburban, or edge-of-town locations.83(p9),84(p16) Good connectivity with the local neighborhood and amenities positively influences quality of life for older people50(p681),51(p90) and enables vital social connections for a demographic that often experiences loneliness. 85
Comparatively, these results suggest autistic people need limited or controllable social connectivity, facilitated by a rural location with few or no neighbors to allow sensory and social distance from others, and practical connectivity with the local neighborhood. This is partially supported by existing research of autistic people’s residential needs, which suggest that a quiet location with minimal external sound sources and good connectivity for social and practical reasons is best for autistic people.22(pp15–16),28(p27),30(p1909),34(p16),35(p179),36(p35) Some gerontological design research suggests connectivity extends to creating social opportunities by inviting the general public into the residential care facility,86(p61) but these results suggest this would negatively impact autistic people’s feels of sanctuary.
Building space/size
Geriatric residential care homes with as many as 30 57 to 75 86 residents are considered small, which could be overwhelming for autistic people and negatively impact their need for social distance, and these results suggest even autism design research recommendations of eight residents or less per dwelling unit22(p56),34(p21) might also be too many.
Autistic participants wanted large enough spaces to enable social distance. Gerontological design recommends large spaces,42(pp246–247),46(pp6,10,51(p89),52(p644) and autism design recommends both small37(p42) and large22(pp15),24,34(p22) spaces. Larger social spaces can stop autistic people feeling crowded.30(pp1907–1908) The high number of other residents in residential care for older people could mean that social distance is still hard to attain, even with large spaces.
Navigation and wayfinding
Older people and autistic people may struggle with navigation and wayfinding. Visual differentiation, color differentiations, visual distinctiveness, and other sensory changes22(p17),26,27(pp102–104),29,34(p25),41,42,51,52,58,59 can help. However, the results of this project suggest these recommendations may create a complex and overwhelming sensory environment with too many different sensory sources. Alternative wayfinding aids that do not contribute to the complexity of the sensory environment could be used to ensure both demographics’ needs are met.
Internal permeability is recommended to help older people with wayfinding,58(p142) but this may negatively impact autistic people who desire social distance and to be unperceived when doing daily tasks.
The presence of others makes navigation harder for autistic people; therefore, they would likely be negatively impacted by gerontological recommendations of using open plan spaces to aid navigation and wayfinding.42(p242),51(p90) Additionally, gerontological design suggests social opportunities should be integrated into navigational routes, such as using seating at rest points42(p245) and converging routes.58(p153) These results suggest that this kind of unexpected or unavoidable social interaction would make navigating a residential care facility harder for autistic people.
Separate single-use spaces versus multiuse/open plan/flexible spaces
Older people prefer open plan spaces, as they appear more friendly, offer greater sight lines and intelligibility, and are easier to navigate.42,51 Gaines et al.27(p29) suggest open concept spaces provide social opportunities for autistic people, and others suggest these spaces can be subdivided using nooks, color, and physical dividers,22,28,34 though this visually cluttered style of design could pose issues for autistic people.30(p1912) The results of this research suggest open plan/multiuse spaces create sensory overwhelm, hinder executive function, interfere with routines and daily tasks, and are too populated and can’t be mitigated by subdividing the space in a non-insulated way. Brand and Gaudion31(p32) suggest communal spaces should be designed to accommodate the most sensory sensitive residents, which would preclude open plan spaces. Gerontological design suggests flexible spaces can accommodate differing needs and activities,57(p196),58(p149) but these results suggest flexibility creates unpredictability and executive function challenges for autistic people.
Disconnected spaces versus interconnected spaces
Spatial interconnectivity in geriatric residential care can enable rich spontaneous interaction, 58 make spaces brighter and more welcoming,42(p251) and improve spatial intelligibility 58 and is especially important for those who are bed bound.46(pp6–7)
These results suggest spatial interconnectivity increases the chance of unexpected social interaction and creates a more complex visual, auditory, and olfactory environment, which can cause autistic people distress and make spaces inaccessible. This might outweigh the benefit of visual connectivity allowing autistic people to preview spaces, therefore making them more predictable.27(p29),34(p22) Low-arousal environments should be prioritized when designing for autistic people,22,32,34(p17) which can be aided through good acoustic insulation and isolation,22(p15),27(p75),31(p34),34(p28),37(p42) which would not be possible with acoustically interconnected spaces.
Communal spaces and the extent of the private domain
Autistic people tend to prefer private, single-function separate spaces (such as kitchens or dining rooms). This enables control of the sensory environment,26(p8) spatial organization to best suit individual executive function needs, and the ability to undertake tasks without being observed, socializing, or experiencing social expectations, all of which makes it easier to undertake daily tasks. These results show that concern over interaction with others and the sensory stimuli created by them is one of autistic people’s biggest concerns, something that is supported by Noble et al., 25 which could be better managed with greater private space. Additionally, private functional spaces could help negate the negative impact of residents having differing lifestyles, such as different levels of organization or different waking hours, which participants raised concerns about.
However, both gerontological design practices and autism design research often only discuss the provision of private bedrooms with en suites27(p141),28(p36),34(p30),37(p44),42(pp6,10,51(p88) and communal living/functional spaces, which prevents residents socializing privately and pursing hobbies.46(pp10–11) This is perhaps due to the legacy of deficit or medical model approaches to design, where residential care is viewed as a place to accommodate physical care needs rather than as a home in which people live.
Social spaces
Spaces that enable socialization can improve older people’s well-being. 42 This can be done by designing lively, playful, and welcoming social spaces with a variety of color, texture, and patterns, which are clustered together on the floor plan. 49 These results suggest autistic needs directly oppose this; they prefer quieter, calmer spaces, with limited visual stimuli, and a low number of people. Patterns and visual clutter, in particular, are known to be inadvisable when designing for autistic people.26,30(p1910)
Ahrentzen and Steele28(p24) point out that autistic people’s threshold for too many people might be lower than expected, which should be accommodated when designing social spaces. Flexible seating may enable autistic socialization,22(p32),31(p33) though it could create unpredictability.
The architectural design needs of autistic people and of older people in residential care appear to have dichotomous elements that will make existing residential care facilities inaccessible to or distressing for autistic people. This will compound the social care crisis older autistic people in the United Kingdom are facing, making it harder for them to access the social care they may need.
Limitations
The lack of existing research on the architectural needs of older autistic people made it difficult to define the scope of the project and to contextualize the results. Additionally, the limited amount of existing relevant research with a social model of disability approach meant there were few established methodologies that could be referenced.
The study was also limited in terms of size and ethnic and gender diversity, meaning that the result may not be truly representative of autistic people’s architectural needs and preferences. The number of autistic participants aged over 50 is a limitation partially mitigated by few statistically significant differences between the responses of older and younger autistic people.
Implications
These findings show the built environment can cause sensory challenges for autistic people and affect their ability to undertake daily tasks and that they prefer architectural design that allows them to control their social interactions. It suggests the conflicts between the needs of autistic people and gerontological residential care design are the buildings’ location and connectivity with the local neighborhood, building size, open plan or distinct separate spaces, flexibility of space, spatial interconnectivity, design of navigational routes, and social space design. This challenges Shell’s 29 belief that “buildings for autistic people are better for everyone.” It might be more accurate to state that buildings for autistic people are better for those who do not have directly opposing needs.
It is unclear if there is a design gray area where both demographics’ needs might be met. The solution may lie somewhere in making private spaces as responsive and flexible to the needs of the individual as possible and offering a variety of shared spaces and navigational routes that enable residents to meet their own needs through choice. Further research is needed to find out whether there are ways for these two opposing sets of needs to be met within the same building, without negatively impacting one another. It can be argued that separate facilities would offer a solution, but this would not be aligned with the social model of disability.
Footnotes
Acknowledgment
Thank you to all the participants who answered the questionnaires.
Author Disclosure Statement
The author has no conflicts of interest to declare.
Funding Information
This research received no specific grant from any funding agency.
Authorship Confirmation Statement
E.P. conceived of the study and undertook the design, data collection, data analysis, and writing of the paper. This article has been submitted solely to this journal and is not published elsewhere.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.