
Abstract
Background:
Although regular exercise is a significant predictor of weight loss and weight loss maintenance, bariatric surgery patients are mostly sedentary/ low active presurgery, and up to 44% of these patients do not engage in regular exercise at 1 year postsurgery. Furthermore, of all postsurgical behavioral recommendations, exercise is the most likely area of nonadherence. The goal of this study was to evaluate adherence to a structured, postsurgical exercise program and to explore the preliminary efficacy of this program on trends in exercise frequency, duration, and intensity.
Methods:
Data on exercise behaviors during group exercise sessions and at home were collected from all 46 patients participating in a 12-week, structured, postsurgical exercise program. Linear regression was used to determine whether exercise behaviors changed over time.
Results:
The frequency and duration of at-home exercise increased from 3.3 (1.9) times per week for 37.4 (18.3) min/session at week 1 to 4.3 (1.7) times per week for 50.8 (23.3) min/session at week 12 (p < 0.01 for increase in both frequency and duration). The level of exercise intensity during the weekly group exercise classes increased from 3.5 (0.9) METs (metabolic equivalents; equivalent to a moderate walking pace) at week 1 to 6.3 (2.9) METs (equivalent to a very brisk walking/slow jogging pace) at week 12 (p < 0.01).
Conclusions:
The significant improvements in exercise behaviors observed during this group exercise program suggest that such programs are feasible, and may be effective in helping bariatric surgery patients meet the postsurgical exercise recommendations associated with improved weight loss and overall health.
Introduction
An important shift in nonsurgical obesity treatment research is the focus on weight loss maintenance. 6 This research has shown that habitual daily exercise (defined as activity that is planned, structured, repetitive, and purposeful with the aim of improving aspects of physical fitness) is a significant predictor of weight loss and weight loss maintenance. Although there is limited research related to exercise programs in MO populations, these patients are mostly low active/sedentary in terms of daily physical activity level presurgery.1,7,8 Furthermore, up to 44% of bariatric surgery patients do not engage in regular exercise at 1 year postsurgery, and of all postsurgical behavioral recommendations (e.g., diet plan, fluid intake, supplement use) exercise is the most likely area of nonadherence.1,9 Given the problems of weight regain following surgery,4,5 bariatric surgical patients provide an excellent target group to apply medically safe exercise strategies for weight loss and maintenance.
Although research on physical activity and exercise in bariatric surgery patients is limited, several recent studies based on patient self-report suggest that weight loss is improved at higher levels of physical activity.1,10–12 While patients are typically advised by the surgical team at scheduled follow-up visits to increase physical activity to improve postsurgical recovery and weight loss, a structured exercise program is not standard practice in weight loss surgery clinics in the United States. 13 To date, no research has been published to determine whether such programs would be feasible or if they would be effective in increasing exercise behaviors in postsurgical bariatric patients.
Methods
A descriptive study design based on a single patient cohort was used to examine the study aims. Specifically, we aimed to: (1) evaluate adherence to a structured, postsurgical exercise program; and (2) explore the preliminary efficacy of this program on trends in exercise frequency, duration, and intensity in both group exercise sessions and exercise completed at home (i.e., outside of the group sessions) over the course of the 12-week program.
Study setting and population
North Shore Medical Center (NSMC) in Salem, MA, provides the only structured exercise program for bariatric surgery patients that we are aware of nationally. NSMC has operated this unique postsurgical program since 1999, and has an annual pool of approximately 200 patients referred by three bariatric surgeons. The exercise program is part of the Comprehensive Surgical Weight Loss Program (CSWLP), which also includes nutrition and stress management components, and is run by a team comprised of bariatric surgeons, exercise physiologists (EP), dieticians, bariatric nurses, and administrative staff. All bariatric surgery patients at NSMC are required to sign up for the CSWLP. Program costs not covered by insurance are paid by the patient.
Patients begin attending CSWLP group exercise sessions at approximately 1–2 months postsurgery and participate in these weekly 2-h sessions for 12 weeks, such that sessions include both newly enrolled and “ongoing” participants. Exercise sessions begin with a group warm-up, followed by individually tailored programs using cardio equipment (e.g., treadmills, recumbent exercise bicycles, elliptical machines) during which patients are given an appropriate exercise goal by the EPs (e.g., use the treadmill for 15 min at 3.5 mph on setting 5, then move to the recumbent bike for 20 min at setting 4). The cardio session is followed by a group weight-lifting session led by an EP, which focuses on teaching patients about appropriate exercises for all the major muscle groups. The session ends with stretching.
All patients complete an exercise treadmill test (ETT) prior to surgery, which the EPs use in tailoring a safe baseline exercise prescription for each patient. This exercise prescription is based on the resting and maximal vital signs of pulse and blood pressure, determined in the ETT, and includes a target heart rate and a target exertion level for each patient to achieve at their first group exercise session. This exercise prescription is designed to educate patients about appropriate baseline exercise levels, and is used as a starting point for the first group exercise session. EPs then encourage patients to increase their exercise intensity, frequency, and duration over the course of the 12-week program, as appropriate. The EPs have found this to be a safe postsurgical strategy for these bariatric patients.
In addition to the weekly group exercise sessions, all patients are also encouraged to participate in regular exercise outside of the program. Patients are encouraged to apply what they learn about appropriate exercise type, intensity, and duration in the group classes to their at-home exercise program. This at-home program is largely focused on regular walking sessions, and patients are encouraged to use a pedometer to track their progress.
Data collection and statistical analysis plan
Data on exercise frequency, duration, and intensity during both group exercise sessions and exercise completed outside of the group sessions were collected from all patients who had participated in the CSWLP by March 23, 2010, and who had bariatric surgery (i.e., laparoscopic adjustable gastric banding [LAGB] or gastric bypass surgery [GBS]) between October 1, 2009, and February 28, 2010. Patients began the CSWLP at different times. For the purposes of this analysis, patient data were sorted by week in program rather than by calendar date; therefore week 1 data represent each patient's first day in the program.
Data collected at group exercise sessions included demographic information, clinical information, and exercise-related information. Data on exercise completed during the group exercise sessions were collected by the EPs, and data on exercise completed outside of the group sessions were self-reported by patients in weekly exercise logs provided by the EPs. Data collected during the group sessions included type of exercise, duration of each type of exercise, metabolic equivalent (MET) level during exercise, and perceived exertion level during exercise assessed using the Borg Scale. The Borg Scale ranges from 6, representing no exertion at all, to 20, representing maximal exertion. 14 Self-reported data collected on exercise completed outside of the group sessions included number of exercise sessions per week, duration of exercise, type of exercise, and average Borg level during exercise. Data on exercise frequency, duration, METs, and Borg levels were summarized using means and standard deviations (SD). Linear regression was used to determine whether these exercise variables changed over time.
Pedometer use data were collected from patient exercise logs for the period from February 9, 2010, through March 23, 2010. Among those using pedometers each week, means and SDs were calculated for days per week of pedometer use and pedometer steps per day. Linear regression was used to determine whether pedometer use changed over time.
Results
For the period from October 1, 2009, through February 28, 2010, 59 patients had bariatric surgery at NSMC. Of these, 46 (LAGB: n = 15; GBS: n = 31) attended at least one weekly CSWLP group exercise session by March 23, 2010. For the 46 patients included in this analysis, mean (SD) age at surgery was 43.2 (12.2) years and 80.4% were female (Table 1). Mean preoperative body mass index (BMI) was 44.7 (6.3) kg/m2, which corresponded to a percent excess weight of 49.0% (7.0%). Percent excess weight loss (%EWL) from surgery to the first group session was 19.7% (8.3%).
SD, standard deviation; BMI, body mass index.
Of the 46 who began the program, six (13%) dropped out (defined as continued absence from group exercise sessions for ≥4 weeks), 13 completed the 12-week program, and 27 were still enrolled in the program as of March 23, 2010 (Table 2). For the 13 patients who completed the 12-week program, %EWL increased to 38.8% (12.0%) by the final group session. GBS patients (n = 10) had a larger %EWL at 12 weeks compared to LAGB patients (n = 3), 43.0% and 24.9% respectively. Using the Kruskal–Wallis test, this difference was found to be statistically significant (p = 0.03).
At the weekly group exercise class sessions, the average duration of exercise increased from 33.7 (8.8) min to 42.9 (7.4) min (r2 = 0.08, p < 0.01; Fig. 1a). Level of exercise intensity increased from 3.5 (0.9) METs (equivalent to a moderate walking pace) at week 1 to 6.3 (2.9) METs (equivalent to a very brisk walking/slow jogging pace) at week 12 (r2 = 0.20, p < 0.01; Fig. 1b), and perceived level of exertion measured using the Borg Scale increased from level 12.0 (1.4) (defined as “fairly light” to “somewhat hard”) at week 1 to level 14.3 (1.7) (defined as “hard”) at week 12 (r2 = 0.14, p < 0.01; Fig. 1c).

Trends for exercise completed during group exercise sessions:
All 46 patients also reported the frequency and duration of exercise completed outside of the group exercise sessions. At week 1, patients exercised an average of 3.3 (1.9) times per week for 37.4 (18.3) min/session, and this increased to 4.3 (1.7) times per week for 50.8 (23.3) min/session at week 12 (p < 0.01 for increase in both frequency and duration; Fig. 2a). Perceived level of exertion also increased steadily, from a Borg level of 11.9 (1.4) at week 1 to 15.2 (1.7) by week 12 (r2 = 0.21, p < 0.01; Fig. 2b). Mean pedometer steps per day increased significantly across the 12-week program, from a low of 7,600 steps/day at week 3 to a high of 12,750 steps/day at week 11 (r2 = 0.14, p < 0.01; Fig. 2c).
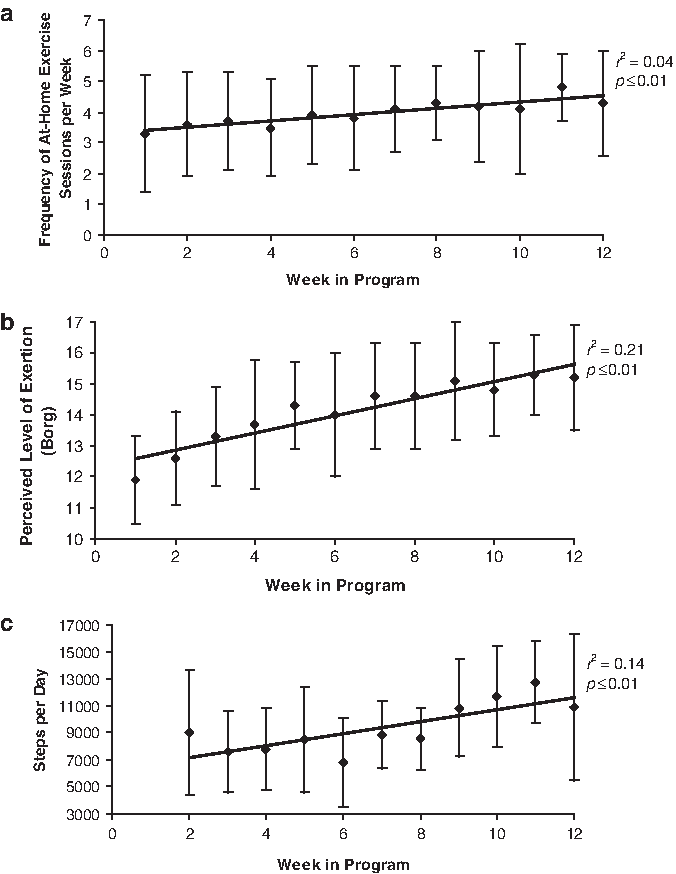
Trends for exercise completed during at-home exercise sessions:
Discussion
This analysis of a structured, postoperative exercise program for bariatric surgery patients showed that exercise behaviors improved significantly over the course of the 12-week CSWLP. Specifically, the frequency, duration, and intensity of exercise increased, as did perceived exertion during exercise and pedometer steps per day. Enrollment among patients eligible for the CSWLP was high (78%) and the dropout rate during our data collection period among patients who began the program was low (13%), indicating good adherence to the program. These results highlight the feasibility of a structured exercise program following bariatric surgery.
Although nonstructured physical activity has been shown to improve postsurgical weight loss in bariatric surgery patients,1,10–12 the CSWLP at NSMC is the only structured, postsurgical exercise program of its kind that we are aware of nationally. While there was no comparison group for this analysis, the significant improvements in exercise behaviors observed over the course of this program suggest that such programs may be effective in helping patients meet the exercise goals set forward in weight loss guidelines. The U.S. Department of Health and Human Services recommends 150 to 300 min of moderate, medically appropriate exercise per week for adults, 15 a level achieved by all patients in the present analysis. By comparison, our previous 2-year follow-up study of bariatric surgery patients found only that 51.4% of patients self-reported exercising to this guideline. 1
While we were unable to compare directly weight loss in CSWLP participants to a control group, %EWL in CSWLP participants was high relative to national averages. Nationally, GBS patients lose an average of 25% to 40% of their excess weight by 3 to 6 months, 16 while GBS patients in the CSWLP lost an average of 43% of their excess weight by the end of the program, which corresponds to 4 to 5 months postsurgery.
Limitations
The current analysis is based on a comprehensive postsurgical program, which includes nutrition and stress management components. Thus it is possible that other aspects of the program, and not just the exercise component, contributed to our positive results. Conversely, it is also possible that these nonexercise components of the CSWLP contributed to patient dropout and/or reduced compliance. Of these, the first scenario seems more likely given that improved exercise behaviors may encourage good nutritional choices and vice versa. 17
Data on exercise completed outside of the group sessions were self-reported by patients, and as such may be less accurate than data collected by the EPs during the group sessions. However, patients were given weekly exercise logbooks to use for tracking their at-home exercise, and were shown how to complete the logbooks by the EPs. In addition, trends in self-reported at-home exercise intensity and duration were similar to those measured by the EPs during the group sessions, suggesting that patients were reporting the information accurately.
Despite the small sample size at week 12 (n = 13), we were able to observe significant trends in exercise behaviors over the 12-week period. However, it is possible that the 13 patients who completed the program during our data collection period differed from general CSWLP patient population, and that a larger sample would reveal a more accurate picture of exercise trends. Repeating this analysis in a larger population would be useful in determining the extent to which the observed results will generalize to other populations.
Conclusion
Changing lifelong sedentary behavioral patterns is difficult and it is unknown whether the short-term exercise improvements shown in this study will be maintained over time. Up to 44% of bariatric surgery patients do not engage in regular exercise at one year post-surgery, and of all behavioral recommendations exercise is the most likely area of non-adherence.1,9 A recent study by Bond et al. of patients successfully maintaining weight loss found that patients who lost weight via surgical methods reported less exercise and dietary restraint than those who lost weight using non-surgical methods. 18 This Bond et al. study supports our current findings that morbidly obese patients can successfully improve exercise behaviors, but also suggests that bariatric surgery patients may focus on the surgical control of hunger and food intake to achieve weight loss and may not be realizing their weight loss potential due to their lack of behavioral changes. Thus, a structured exercise program may be of great benefit in helping post-surgical patients achieve greater weight loss.
There are many theories and models of behavior change, such as Social Cognitive theory and Prochaska's Transtheoretical Model,19,20 that have improved our understanding of how individuals change behaviors. However, we currently lack behavioral, theory-based exercise interventions for bariatric surgery patients. In obese patients, effective behavioral interventions have included self-monitoring, reducing eating cues, responding to social pressures, pre-planning and relapse prevention techniques. 21 The intervention examined in this observational study applied these strategies, although we did not formally assess the behavioral mechanisms used. Further study is needed to clarify the nature and effectiveness of these behavioral strategies over time.
This study examined the feasibility and effectiveness of a structured post-operative group exercise program for bariatric surgery patients and showed that participants significantly increased exercise frequency, duration, and intensity during the 12-week program. Novel strategies to improve weight loss and medical outcomes for bariatric surgery patients are needed to tackle weight variability, weight plateaus, and weight regain. The positive findings reported here suggest that post-surgical exercise programs are feasible and are effective in improving exercise behaviors, at least in the short term, and support the need for a systematic program of clinical research in this area.
Footnotes
Acknowledgments
We would like to thank the CSWLP staff for sharing their time and expertise, and especially Jo-Anne Gibley, CPT, for her assistance with data collection. The Comprehensive Surgical Weight Loss Program at North Shore Medical Center is funded in part by the Norman H. Read Charitable Trust.
Disclosure Statement
No competing financial interests exist.