
Abstract
Background:
Weight bias and stigmatization may result in discrimination against obese individuals by healthcare professionals, decreasing the quality and quantity of healthcare to this at-risk population. The purpose of this program evaluation was to explore the impact of an educational Bariatric Sensitivity Educational Module on healthcare professionals.
Description:
An educational module was designed to address the many causes of obesity and to improve sensitivity through education and knowledge. The program evaluation materials included a demographic form, a pre-survey about attitudes, and an educational module. One month after completion of the module, the program evaluation participants received a post-survey to evaluate the effectiveness of the Bariatric Sensitivity Educational Module on respondents' attitudes toward bariatric patients.
Discussion:
In our sample, the educational module was effective in decreasing weight stigmatization in healthcare professionals one month after the completion of the intervention.
Conclusions:
Bariatric sensitivity educational modules are useful tools to help decrease stigmatization. These tools may be easily adapted to a web-based educational format in a variety of healthcare settings. The Bariatric Sensitivity Educational Module has been placed into our facility's web-based education system and has been completed by more than 700 members of our nursing staff.
Introduction
Data from the 2007–2008 National Health and Nutrition Examination Survey (NHANES) show that among adults aged 20–74 years, the overall prevalence of obesity is 33.8% in adult men and women in the United States. 6 In adolescents and teenagers, the 2007–2008 NHANES indicated the prevalence rates for obesity were 18%. 7 However, despite the increasing prevalence of obesity in the United States, weight discrimination and stigmatization remain problematic. Unlike race and gender, weight is not a protected category under U.S. federal law except in the state of Michigan. 8 Consequently, obesity discrimination prevalence rates among American women are close to reported prevalence rates of race discrimination. 9 Weight discrimination results in a negative impact on lifestyle, job availability, and provision of healthcare services. 1 Questions have been raised as to what extent obesity discrimination may be covered under the Americans with Disability Act (ADA) of 1990. However, the individual must prove in a court of law that they were discriminated against solely because of their weight, which is a difficult and time-consuming process. 10
Discrimination often begins with stereotypes. When a population is stereotyped, individual characteristics of people are overlooked and these characteristics are often replaced by images or traits that are negative in nature. The overwhelming negative stereotypes attributed to obese individuals include laziness, sloppiness, overindulgence, poor hygiene, and lack of self-discipline.2,11–13 A more personal or overt form of stereotyping occurs when this population is not only spoken about in a negative manner, but when the individual person is also stigmatized. The obese individual is now personally branded, described, or identified in terms that signify disgrace or reproach. 14
The impact of stigmatization of obese individuals is present not only in television, newsprint, and cartoons, but also in the medical profession. Research has demonstrated that weight bias is present not only among nurses and doctors in general, but also among researchers and healthcare professionals specializing in obesity.2,15,16 This obesity stigmatization may adversely affect patient care in terms of poor clinical outcomes. The consequences of negative interactions with HCPs may result in obese individuals' reluctance to seek medical care, and potentially decrease early detection and treatment of illness and disease.16–18 This is of great concern when contemplating the high morbidity and mortality rates associated with obesity.
Individuals in the highest obese categories are significantly more likely to report discrimination than normal weight persons.3,9 Obese individuals report stigmatization by nurses, physicians, dieticians, and other healthcare professionals.10,11,19–21 When receiving medical care, experiences of humiliation, embarrassment, insults, and blatant verbal abuse regarding their weight from their treating physicians are often described. 22 Obese patients not only experience negative attitudes, but also challenging physical environments not suited for their physical needs. 23 This complexity of consequences of bias and stigmatization not only impacts patient care, but also results in decreased patient satisfaction.
Patients describe hearing negative comments by HCPs such as: “She has short arm syndrome and can never help herself,” “They always need more assistance than everyone else,” “I need less patients when I have to take care of people like her,” and “They didn't take care of themselves and now they expect us to be miracle workers.” This situation worsens when HCPs use disparaging terms and statements when conversing with other professionals about the patient. These comments place negative inferences in patient care providers prior to introduction to the patient. As a result, healthcare disparity may occur related to patient fears of discrimination by HCPs and the corresponding attitudes and medical treatments provided by HCPs.16,18,24
It is important that HCPs evaluate their perceptions of obese individuals to prevent this disparity in healthcare.24,25 Obesity in and of itself increases morbidity and mortality, let alone the increased risk for illness due to obesity-related disorders that require timely and appropriate care by HCPs. Ostracization due to body size is evidenced by negative attitudes and remarks, discriminatory behaviors, and challenging physical environments. This may create a fear in obese individuals which could result in a reluctance to seek needed healthcare.16,20,26 To decrease bariatric stigmatization and bias, which negatively affects patient care, HCPs may benefit from a bariatric sensitivity program.2,11,27,28 To address the issue of bariatric sensitivity in healthcare professionals, a program was designed, implemented, and evaluated at a large metropolitan academic medical center.
Program Description
The program was developed to determine if a bariatric sensitivity educational module could decrease stigmatization among healthcare professionals. The program included the Bariatric Sensitivity Educational Module designed to address the many causes of obesity and to promote sensitivity through improved knowledge and understanding about obesity. The module was driven by the concept that education and knowledge improves empathy and decreases stigmas toward obese individuals.27–29
The educational self-learning module, in a written format, began by introducing the concept that we are all more alike than different; that we all want to be treated with respect and dignity. The 44-page module also included information about common bariatric stereotypes, causes of obesity, discriminatory actions, negative attitudes, and improper responses by HCPs. Each page (Appendices A and B) focused on one concept to encourage the reader to contemplate the written material fully. Experts in the field of diversity training and education analyzed the Bariatric Sensitivity Module for content validity and verified its usefulness as a potential educational tool to help improve bariatric sensitivity and decrease stigmatization. The Bariatric Sensitivity Program and its evaluation received approval from the medical center's Institutional Review Board.
Sample
Recruitment information for the Bariatric Sensitivity Program was presented in multiple organizational meetings including: Patient Care Leadership, Clinical Practice Council, and staff meetings. Patient Care Leadership memberships include the Vice-President of Nursing, hospital directors, clinical managers, advanced practice nurses, and charge nurses. The Clinical Practice Council is comprised of chairpersons from each unit practice committee within the hospital. Information regarding the Bariatric Sensitivity Program was also presented at monthly staff meetings.
Requests for participation in the program was presented at each of the organizational meetings. There was great interest in the program, and 14 hospital units agreed to be recruitment sites. Recruitment flyers were posted throughout the 14 units describing the purpose and requirements of the program. Approximately 600 staff members were exposed to the recruitment materials. Of those, 101 responses were submitted with 30 staff members completing both the pre- and post-surveys.
Method
The program evaluation involved distributing the bariatric sensitivity informational materials including the Bariatric Sensitivity Self-Learning Module, a demographic form, and the “Care of the Bariatric Patient Nursing Survey.” The demographic information included gender, years in nursing, height, and weight (see Table 1). The “Care of the Bariatric Patient Nursing Survey” was developed to measure how likely a staff member would have stereotypical attitudes toward obese patients before and after sensitivity training. Although surveys regarding attitudes toward obese patients were reviewed, they did not measure the concepts of interest for this program. The newly developed survey targeted staff's knowledge and sensitivity toward obese patients. The survey was created using the author's clinical expertise and information gathered from the literature review on bariatric patients. The survey included eight statements, utilizing a 4-point Likert scale. Responses to the statements ranged from 1 = “Strongly Agree” to 4 = “Strongly Disagree.” Examples of the survey statements included: “I am sensitive to the physical needs of my bariatric patients,” “I am aware of how my attitude affects the care I provide to bariatric patients,” and “I am sensitive to the psychological concerns of my bariatric patients.” A lower score indicated a more sensitive response.
An informational sheet detailing the program evaluation was attached to the Bariatric Sensitivity Module. Submission of the demographic form and pretest by participants indicated their consent for participation in the program evaluation. To maintain confidentiality, the respondents were requested to label each form with the last two letters of their mother's maiden name and the last two digits of their social security number.
Participants in the program received initial instructions on the Bariatric Sensitivity Module requesting them to read the module thoughtfully and to contemplate the content presented. One month after completing the pre-survey, participants completed the post-survey. The completed forms were placed into a dedicated locked response box located on each hospital unit. The pre- and post-surveys were matched by the unique codes provided by the participants.
Program Evaluation
The Bariatric Sensitivity Module was open to all healthcare professionals on the 14 hospital units. Participants completed both pre- and post-survey materials. The respondents were comprised of registered nurses (80%), patient care technicians (17%), and unit secretaries (3%). The majority of the participants in this program evaluation had a Bachelors of Science degree in nursing or higher (n = 19). Female participants comprised 87% (n = 26) of the sample. Utilizing the Clinical Guideline for the Identification of Obesity, 30 17% of the program participants were overweight (n = 5), 37% were obese (n = 11), and 6% were extremely obese (n = 2). The prevalence of obesity in the program participants was 60% with an average BMI of 28.5. The pervasiveness of weight stigmatization is not limited to non-obese individuals. 31 Research indicates that a significant amount of weight bias is evident in even the most obese individuals toward other obese individuals (see Fig. 1).32,33
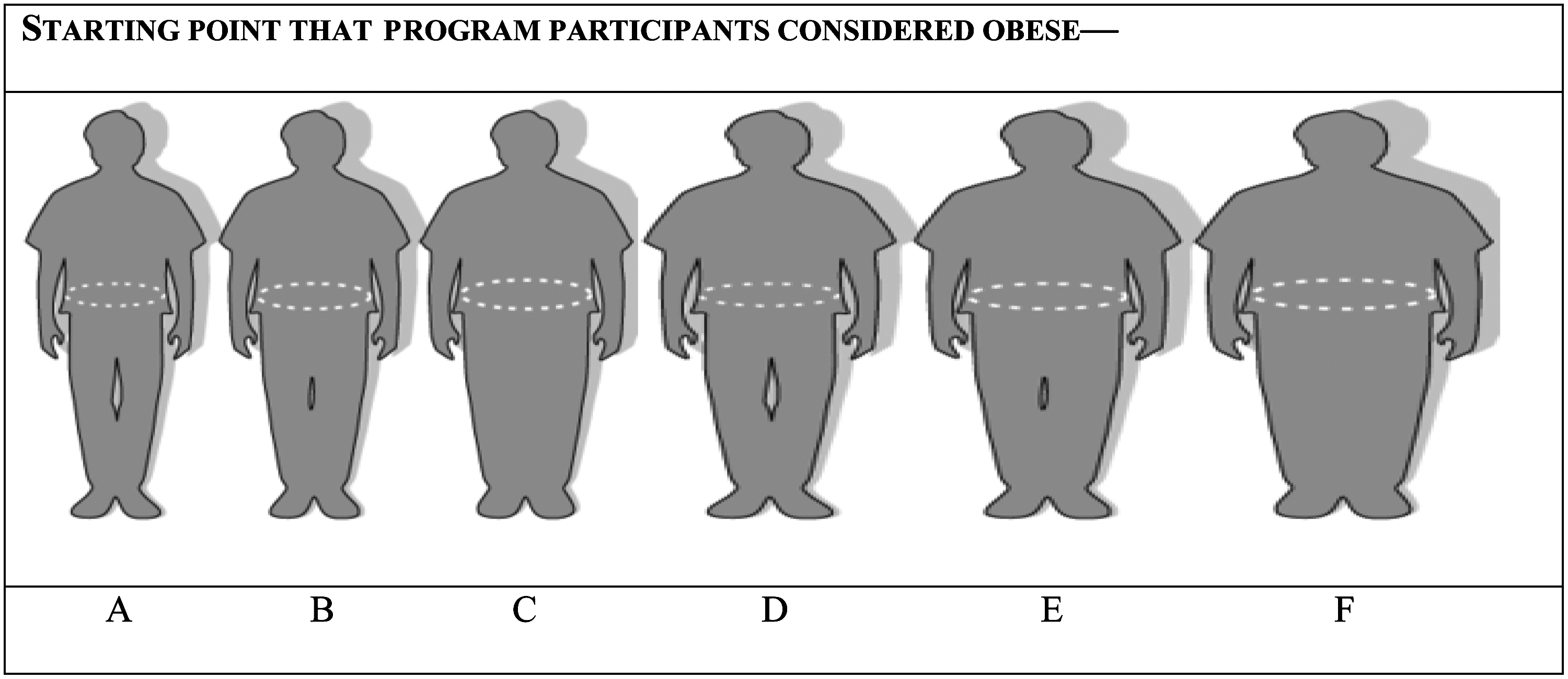
The silhouettes and waist circumferences (WC) represent perceptions of body size, such as, normal, overweight, and obese.
The average number of years in healthcare practice of the participants was 8.2 (1–38) years. The respondents worked in a variety of specialty areas including trauma surgery, vascular surgery, medicine, gynecological oncology, operating room, colon/rectal surgery, transplant surgery, and the post-intensive care rehabilitation unit. Of the 30 respondents, only 6 (20%) had previously attended a program concerning obesity. Similarly, in a study conducted by Brown et al., they too noted that very few of the 564 nurses reported training in obesity management or organizational support in this area. 34
The survey findings indicate that a bariatric sensitivity educational module may decrease bariatric stigmatization in healthcare professionals. Descriptive statistics were used to evaluate the impact of the intervention on HCPs scores on the Care of the Bariatric Patient Nursing Survey. The Bariatric Sensitivity Educational Module includes information on the effect of staff attitude on the healthcare provided to bariatric patients. The module describes how the negative attitudes of HCPs may be reflected in verbal interactions, mannerisms, and care provided to the bariatric patient. In the survey, staff were asked if they were aware of the impact of their attitude on the care they provided to bariatric patients. Pre-survey responses (Table 2) indicated 40% of the staff strongly agreed with this statement prior to reading the module. There was a 20% increase in awareness in the post-survey (Table 2) results.
Lower scores indicate a more sensitive response.
Understanding the negative stereotypes commonly associated with bariatric patients may also help decrease bariatric stigmatization. It is imperative that HCPs do not automatically label patients and desensitize themselves to the healthcare needs of the patient. If HCPs believe all bariatric patients are lazy, slovenly, or difficult to care for, it is highly unlikely that they are providing quality patient care.11,13,16 In the survey, staff were asked if they knew the common stereotypes faced by bariatric patients. Results indicate that there was a considerable increase in the knowledge of the negative stereotypes faced by bariatric patients (pre-survey 30%, post-survey 50%). An increase in knowledge may help decrease stereotypical behavior among HCPs.
It is imperative that HCPs are sensitive to the physical needs of bariatric patients. Ordering proper equipment and gowns, providing excellent skin care, and safe handling practices are crucial in this specialized population. Understanding the physical needs of bariatric patients may help HCPs become more sensitive in their assessments and improve the quality of care they provide. In the survey, staff were asked if they were sensitive to the physical needs of the bariatric patient. Prior to reading the module, only 23% of staff expressed an awareness of patients' physical needs. However, post-survey results indicated 37% of staff had an increased awareness of the physical needs of the bariatric patient.
Discussion
It is well recognized that stigmatization of obese individuals by healthcare professionals is a major healthcare concern. Educational strategies that decrease negative stereotypes and increase accessibility to healthcare services may improve quality of care and increase patient satisfaction.2,23 Various methods of delivery of educational modules to decrease stigmatization have been noted in the literature. A program using a combined program of video, live instructors, and written materials has shown some success in decreasing obesity stigma in medical students. 28 In-service training with live instructors has also proven useful in improving sensitivity in nurses. 35 However, these methods of delivery are costly and difficult to carry out in the hospital setting due to the number of employees involved, the varied days and shifts worked, and the demands of patient care. Additionally, limited research has been done utilizing written materials as a method to evaluate bariatric stigmatization in HCPs. Therefore, the Bariatric Sensitivity Module was designed in a written format for healthcare professionals to complete when convenient for them.
There were challenges to this program, even though the module was delivered in written format. Only 101 individuals completed the pre-surveys, with 30 individuals completing both the pre- and post-surveys. Given the variability of HCPs' work schedules and the demands of patient care, it may have been challenging for the HCPs to complete the pre- and post-surveys, resulting in a lower response rate. Although this project utilized a written format, the future goal of the Bariatric Sensitivity Module is for use as a web-based program for healthcare professionals. Therefore moving this module to a web-based program may increase the completion rate among HCPs.
Implications
In this program, a written Bariatric Sensitivity Educational Module provided to HCPs was effective in decreasing stigmatization toward the bariatric patient. Providing education to HCPs is often difficult because of staff shortages, 24-hour work schedules, conference room availability, and access to instructors. There has been a recent trend toward web-based educational modules because of the flexible access to content and instructional material. 36 Finklestein and Lapshin found that a web-based educational module directed towards HCPs caring for those with stigmatizing conditions, such as depression, was affective at decreasing bias with this patient population. 37
The Bariatric Sensitivity Educational Module was developed and distributed in paper format to program participants. Given the original format of the written educational module, it can be easily reformatted into a hospital wide web-based educational module. Furthermore, online web-based programs have the potential to be more cost-effective than written materials, class time, and instructor fees.
The ability to provide a bariatric sensitivity module that would be readily available online may have a major impact in decreasing bariatric stigmatization in HCPs and improve the healthcare of bariatric patients. Healthcare organizations would have the ability to place sensitivity modules in their online educational libraries and include them in new employee orientation or as annual competencies.
Additionally, recognizing a facility's commitment to decrease bariatric stigmatization should impress upon HCPs the importance of making positive changes in attitude and behavior toward the obese individual. The Theory of Planned Behavior assumes that if individuals, such as HCPs, make a conscious and determined effort to decrease their biases and stigmatizations, they are more likely to be successful in this effort.38,39 Subsequently, HCPs who recognize the impact of stigmatization upon the bariatric individual may make concentrated efforts to decrease their bias and stigmatization at the completion of a bariatric sensitivity module.2,17 Increased sensitivity and decreased stigmatization by HCPs toward bariatric patients may improve the quality of healthcare provided to this population and improve patient satisfaction.
Conclusion
The overwhelming number of stereotypes attributed to the bariatric patient may negatively impact the perception of HCPs and result in a disparity in healthcare practices. In a population that is at an increased risk for morbidity and mortality, it is imperative that HCPs provide unbiased care. In this program, the Bariatric Sensitivity Education Module had a positive effect in decreasing bariatric stigmatization. As a result, the written module was reformatted into a web-based educational module in our hospital.
This web-based Bariatric Sensitivity Education Module is now a required competency in several areas in our medical center and is a required competency for new hires. The long-term goal of our center is to make the Bariatric Sensitivity Education Module a required annual competency as a patient satisfaction initiative. To date, more than 700 nurses, patient care technicians, unit secretaries, and healthcare professionals in our facility have completed the web-based Bariatric Sensitivity Education Module. Although change in behavior takes time, there have been notable differences in how our HCPs interact with our bariatric patients, as well as with other staff members. We have noted less stereotyping and negative terminology used in reference to our bariatric patients. Over the course of this past year, our staff has become more attuned to the specialized needs of this population, which ultimately increases patient and staff satisfaction.
Footnotes
Acknowledgments
The authors wish to thank Margaret S. Ulione, Brenda Battle, and Barbara Bogomolov of Barnes-Jewish Hospital, St. Louis, Missouri.
Disclosure Statement
No competing financial interests exist.