
Abstract
Introduction:
In some bariatric services, patients have formed a support group, which is led exclusively by patients. Does attendance at such support groups influence outcomes?
Background:
Existing literature is from continental Europe and the United States and mainly focuses on single operation support groups. Most studies feature professional-led support groups. The success of a support group is difficult to measure, but hard outcome measures such as weight loss are available.
Methods:
At our institution in the United Kingdom, there is a complete prospectively compiled database of weight-loss outcomes from patients who have had the three types of surgery on offer: gastric bands, gastric bypasses, and sleeve gastrectomies. A total of 118 patients were contacted, and 100% took part in a telephone questionnaire survey. All patients were asked about attendance, frequency, and reasons for their answers. Preoperative body mass index (BMI), age, sex, and 12-month percentage excess weight loss (12m %EWL) was recorded from the database.
Results:
The 12m %EWL for band patients was 40.1% (attendees) and 46.4% (nonattendees). For bypass patients, it was 74.8% (attendees) and 75.6% (nonattendees). For sleeve patients, it was 51.3% (attendees) and 44.3% (nonattendees). Following gastric banding, the 12m %EWL was 28.1%, 42.7%, and 49.3% for patients attending either one, two to five, and more than five sessions respectively. For all surgical groups, the main reason cited for attendance was to be with like-minded people, and the main reason for nonattendance was being too busy to get to the group.
Conclusions:
For band patients, increasing frequency of attendance was associated with increasing 12m %EWL, in keeping with existing literature. For bypass and sleeve patients, there was no significant difference in weight-loss outcomes comparing attendees with nonattendees. This study, accepting the limitations of using 12m %EWL as a surrogate for success, appears to confer the psychosocial benefits of a support group but is not apparently required for absolute weight loss.
Introduction
Background and Literature Review
The patients at our institution follow a very clearly defined pathway (Fig. 1). They are all referred after completion of a community weight-management program in which a minimum of 5% weight loss is expected. If this is achieved, then they attend a group seminar led by the surgeons, dieticians, and nurse specialists. At this session, they learn about the realities of surgery and life after surgery, and are introduced to the support group representatives. The prospective patients are invited to attend the patient-led support group as little or as often as they desire. Successful patients will meet the strict dietary and psychological requirements before proceeding to an operation of choice that is determined by both the patient's desire and the surgeon's recommendation.
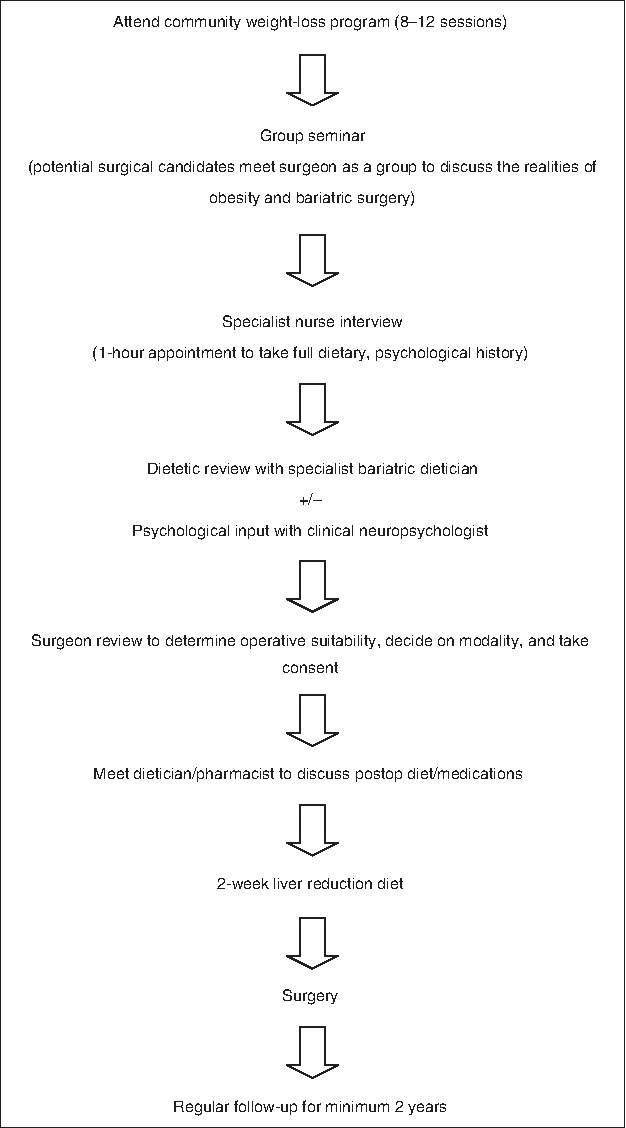
Patient pathway—a patient can attend the patient-led support group at any stage along this pathway.
The definition of “support group” in the existing literature is not consistent, and within this term, there are many variables such as group leadership, operation type, minimum attendance expected, and timing around surgery. This heterogeneity makes comparison between studies difficult. Song et al., for example, describe a support group for gastric bypass patients led by the surgeon, nurse practitioner, or dietician, 3 whereas Elakkary et al. describes a nurse-led gastric-band support group in which there was a mandatory attendance rate of >50%. 4 Notwithstanding this heterogeneity in the literature, the tentative conclusion from previous studies is that there is a positive association between support groups and degree of postoperative weight loss.1,4–6 One of these did not reach statistical significance, however. 6 The aim was to clarify this situation with our patient-led support group population.
Methods
A complete prospectively compiled database is available at our institution. A total of 118 patients, who were at least 12 months post-surgery, were contacted, dating back to 2009. This timeframe corresponded with the establishment of a dedicated patient-led support group. All included patients had a documented 12-month postoperative weight recorded, in addition to standard demographic data and preoperative weight statistics. A copy of the survey is included in Appendix 1. A chi-square test and a two-tailed t-test were used for categorical and continuous data respectively. A p-value of less than 0.05 was considered to be statistically significant.
Results
There was a 100% response rate from the patients who were contacted. There were 62 attendees, and 56 nonattendees. The attendees reported a variable number of attendances at the support group and could attend at any stage along their weight-loss journey (Fig. 1).
There was no significant difference between the two groups in terms of age, sex, or preoperative body mass index (Table 1).
Chi-square analysis of 2×2 contingency table; categorical data. **Two-tailed t-test for continuous data.
M, male; F, female; BMI, body mass index; Preop, preoperative.
In overall terms, the 12-month percentage excess weight loss (12m %EWL) was 68.4% for attendees and 64.4% for nonattendees. This did not reach statistical significance. Increasing frequency of attendance correlated with increasing weight-loss outcomes but again did not reach statistical significance (Table 2).
12m %EWL, 12-month percentage excess weight loss.
Table 3 breaks down the results into the respective operations. Similar results are found to the overall group data. The relationship between increasing frequency of attendance and improved outcomes seen in the overall data is replicated in the band population but not so for the sleeve or bypass subsets.
12m %EWL, 12-month percentage excess weight loss.
The patients were asked about the reasons for attending or otherwise, and read a list of reasons and were asked for their top reason. This is shown in Table 4.
Discussion
At our institution, the support group is exclusively patient led and is designed to be a forum in which patients can express themselves in a safe, secure environment without fear of retribution. Those who choose to attend can do so at any stage on their weight-loss journey (Fig. 1); attendance is purely voluntary, and there is no mandatory minimum requirement.
Reasons for this reported positive association might include personal motivation and perhaps a degree of self-selection. Those patients who are likely to be most engaged in the weight-loss pathway are most likely to attend a support group. However, the outcome from our study might suggest that the patient support group per se does not contribute to weight loss. There are many mandatory meetings for the patient in our particular pathway that are likely to have more influence on weight-loss outcome, such as the interview with the psychologists and meeting the dietician on at least two occasions.
Using 12m %EWL as a marker for success of a support group is not ideal, but it is the best measurable marker of surgical outcome that we have available. Support group attendance appears to confer psychosocial advantages to the patients, and perhaps validated quality of life/social questionnaires would be a better measure of “success.” Surgical success does not always equate to patient success, as poorly consented patients might develop depression from poor postoperative body image and regret the surgery despite excellent weight loss. 7 Previous studies have attempted to use existing quality of life measures including the general health perceptions (GHP) scale from Short Form 36 (SF-36). 8 New psychosocial questionnaires have been developed such as the Bariatric Surgery Self-Management Questionnaire, 8 but these currently lack formalized reliability and construct validity studies.
Patients' reasons for their choice to attend or otherwise were interesting, but it was perhaps artificial to ask them to categorize a top reason. Most patients had many personal reasons and welcomed the opportunity to talk at length about these. This result was included for interest rather than scientific rigor.
The overall conclusion that may be cautiously drawn is that attendance at the support group does not appear to influence short-term surgical outcome using 12m %EWL as the measurable end point. The modality of surgery does not appear to influence outcomes. For band patients specifically, an increased frequency of attendance is associated with increasing percentage excess weight loss, but this effect does not reach statistical significance.
Patient psychology and behavior is a complex area to understand and measure. To truly understand the value in patient support groups, there needs to be agreement of the precise definition of the support group, consistency in the approach of the group including topics discussed, and randomized prospective trials with appropriate outcome measures.
Footnotes
Acknowledgments
We would like to thank Steve Ward and Tracey-Jayne McDonald from the North Tyneside support group for their invaluable help, advice, and contact details.
Disclosure Statement
No competing financial interests exist.
Appendix 1: Patient Questionnaire
1. What is your date of birth? (dd/mm/yyyy)
2. What operation did you have?
□ Gastric Bypass
□ Sleeve Gastrectomy
□ Gastric Band
□ Gastric Balloon
□ Revisional surgery; e.g., band to bypass
Other (please specify
3. When was your operation?
□ pre-2010
□ 2010
□ 2011
□ 2012
□ not had surgery yet
4. Did you attend a patient support group at any time during your weight-loss journey?
□ Yes
□ No
5. If you did not attend, please explain why.
□ I did attend a support group
□ Lived too far from support group
□ Did not see the point or value in a group
□ Did not know one existed
□ Have attended a group before and did not like it
□ Felt intimidated
□ Did not want to share my story with others
□ Already had enough information from other sources
Other (please specify)
6. When did you attend the patient support group?
□ Did not attend
□ Before surgery
□ After surgery
□ Before and after surgery
7. How many times did you attend?
□ Did not attend
□ Once
□ Twice
□ 3–5 times
□ >5 times
8. Was the experience of the support group valuable?
□ Did not attend
□ Yes
□ No
□ Undecided
9. Please give reasons for your last answer? If did not attend, please move on to Q10.
10. Did you take prescribed medication prior to surgery?
□ Reflux medication
□ Arthritis medication
□ Blood pressure medication
□ Diabetes medication
□ Depression medication
□ No medication
□ Other medication