
Abstract
Introduction:
Little focus has been placed on improving the efficiency of robotic surgery. The aim of this study is to demonstrate areas of inefficiency between robotic (RSG) and laparoscopic sleeve gastrectomy (LSG) and show that the robot can be effectively integrated into a bariatric surgery practice.
Methods:
We retrospectively identified 25 consecutive LSG and RSG and compared preoperative (patient enters operating room (OR) to skin incision), operative (incision to skin closure), and postoperative (skin closure to out of OR) times. Analysis of variance comparing RSG versus LSG was performed, and turnover times for consecutive cases were analyzed.
Results:
The mean preoperative, operative, and postoperative times for LSG versus RSG are 42±8 versus 46±1, 88±19 versus 119±32, and 13±7.6 versus 11±5 minutes respectively. There is a statistically significant difference between LSG and RSG operative times (p<0.001), but there was no significance between preoperative (p=0.164) and postoperative (p=0.395) times.
Conclusion:
The primary contributor to longer duration of a robotic case is the operative time, not preoperative or postoperative times. RSG with a dedicated robotic team can be efficiently performed so that three consecutive RSG can be completed by 3:30 p.m. in a day.
Introduction
M
Currently, the most common bariatric procedures performed in the United States are the laparoscopic Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy (LSG), adjustable gastric band (LAGB), and duodenal switch (LDS). 3 The American Society for Metabolic and Bariatric Surgery (ASMBS) estimates that around 160,000 bariatric procedures are performed every year, a significant increase from only 16,000 a year in the early 1990s. 5 Robotic surgery has had a similar surge in use over the last 10 years. Intuitive Surgical (Sunnyvale, CA) estimates there are now 2,585 da Vinci® systems currently in use and about 450,000 robotic operations performed yearly worldwide. 6 With promises of better visualization, improved range of movement, and better ergonomics, bariatric surgeons have attempted to investigate the practicality of integrating the robot into their practice. Ironically, the introduction of an expensive technology may threaten the proposed healthcare cost savings of weight loss surgery unless it can be used with similar or better efficacy and outcomes.
The majority of research on robotic surgery has focused on feasibility, learning curves, and safety of robotic bariatric surgery.7,8 Many have also shown that operative time and cost have been considered the most prohibitive barriers to the acceptance of robotic bariatric surgery. 9 However, little focus has been placed on identifying or improving on the efficiency of robotic surgery. It is assumed that inefficient time management is mainly related to robot set-up and docking time rather than the actual operation.10,11 The goal of this paper is twofold: to determine potential areas of inefficiency in robotic bariatric surgery using the sleeve gastrectomy as the study case, and to compare robotic sleeve gastrectomy (RSG) to LSG to demonstrate that the robot can be effectively integrated into a bariatric surgery practice.
Methods
This study is a retrospective review of our initial experience with RSG in a newly instituted robotic bariatric program. The procedures were performed during a 15-month period at an academic institution. We identified 25 consecutive LSG and 25 consecutive RSG. Cases were excluded if additional procedures were noted on the operative report.
Surgical technique
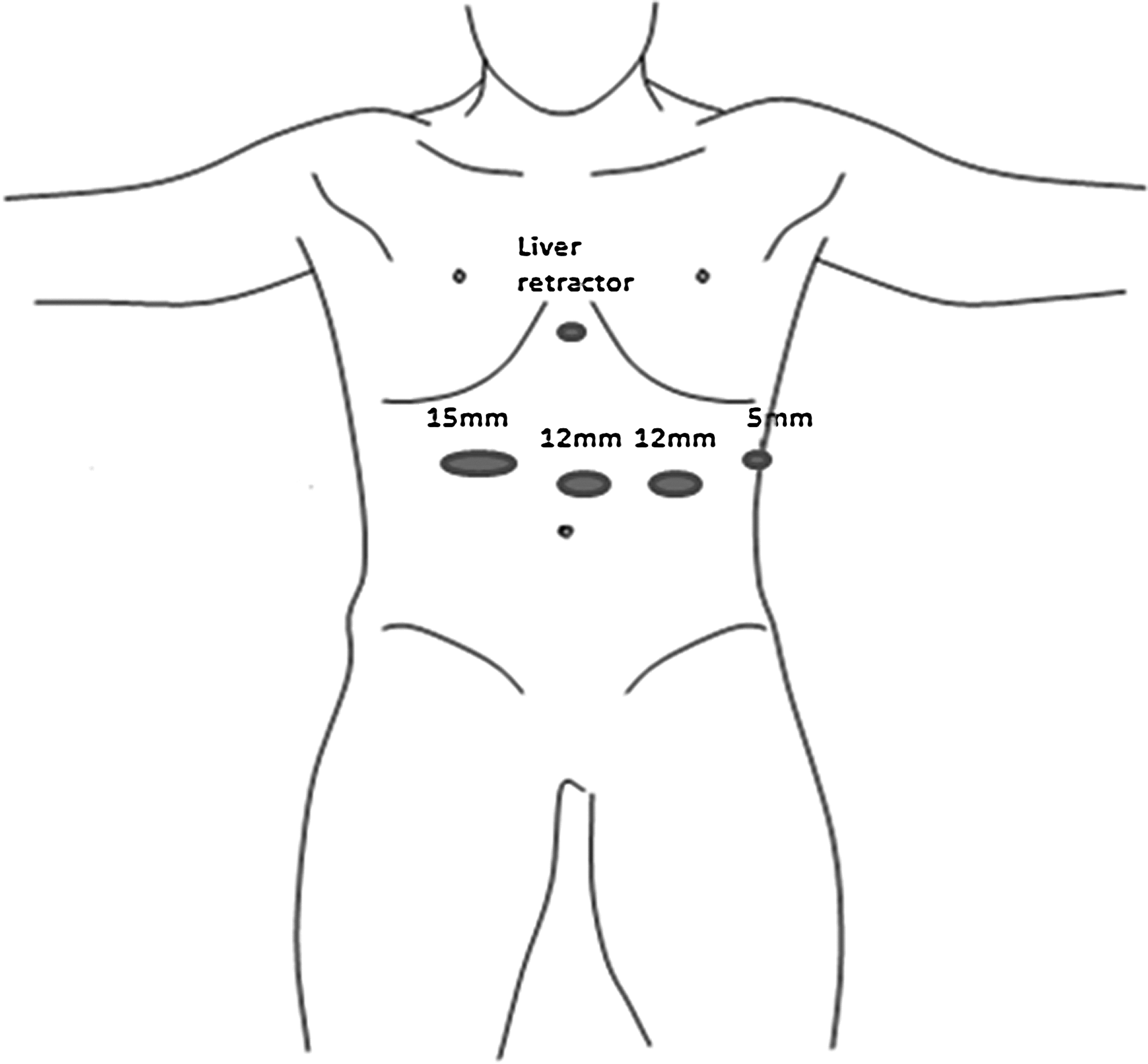
There was minimal variation in the surgical technique between RSG and LSG. The main differences are the number of ports used (five in RSG vs. four in LSG), port placement, and the use of a liver retractor in LSG (Figs 1 and 2). For the RSG, only three robot instruments are used: a Cadiere grasper, a double fenestrated grasper, and an Endowrist® vessel sealer. For the LSG, Hunter graspers and either a bipolar or an ultrasonic dividing device are used to enter the lesser sac and divide the short gastric vessels. An endoscope is used in both procedures as a sizing bougie and to evaluate for leaks upon completion of the operation. Finally, an Ethicon Echelon® motorized 60 mm stapler with staple line reinforcement (Bio-A; WL Gore, Newark, DE) is used in both LSG and RSG.
Laparoscopic sleeve gastrectomy port sites.

Robotic sleeve gastrectomy port sites.
Statistics
Based on the operative log, the case times were separated into preoperative time (time when patient enters operating room until skin incision), operative time (start of incision, docking time, console time, and surgery stop time), and postoperative time (surgery stop time to moment patient is out of the operating room; Fig. 3). Analysis of variance (ANOVA) comparing robotic to laparoscopic times was performed. Turnover time (time when the previous patient is out of the operating room to when the new patient enters the operating room) was also compared for days when consecutive RSG and LSG were performed.

Breakdown of case time.
Results
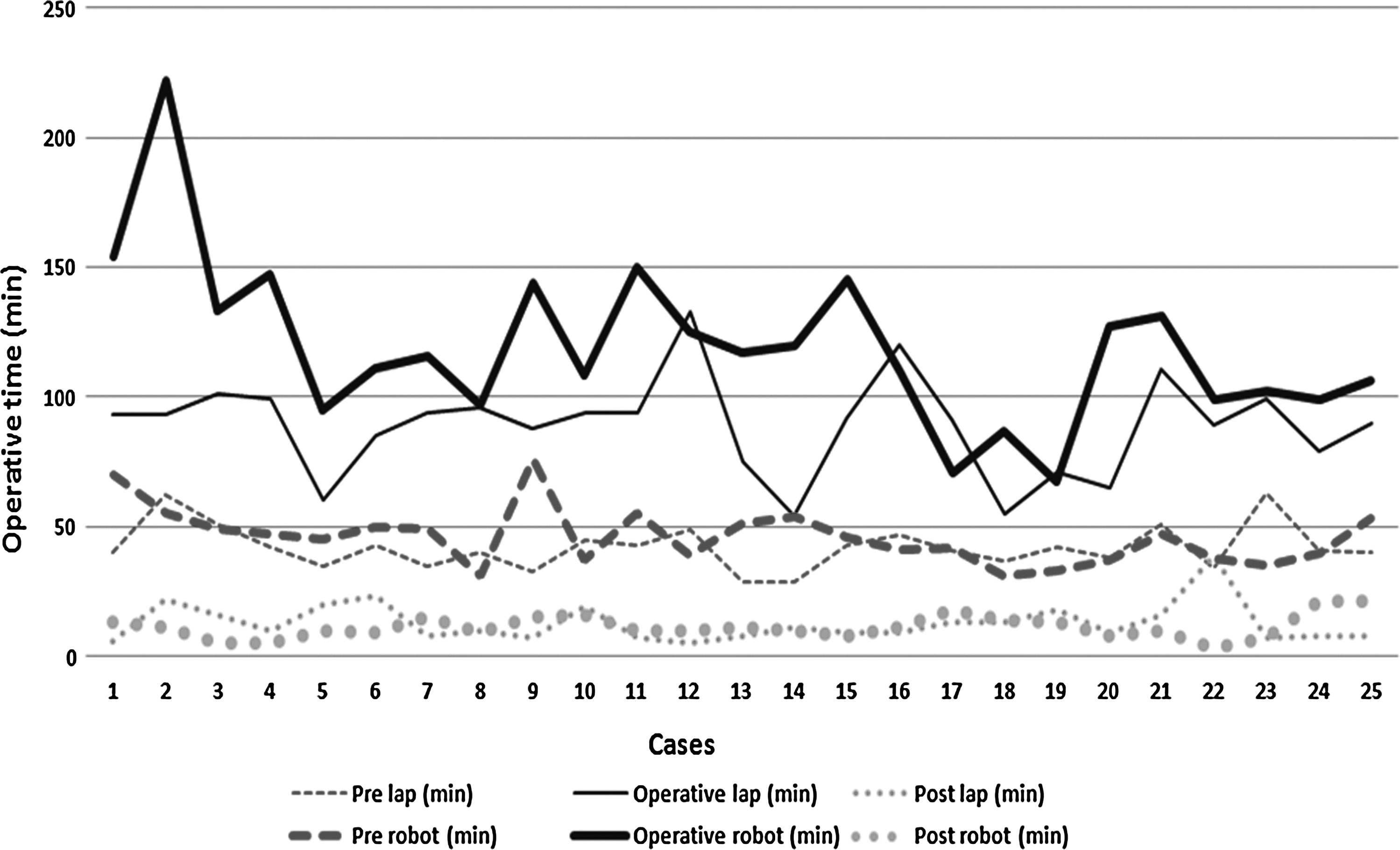
The mean preoperative and postoperative times for LSG versus RSG were 42±8.5 versus 46±1 minutes and 13±7.57 versus 11±4.6 minutes respectively (Table 1). There was no statistical significance between preoperative (p=0.16) and postoperative (p=0.40) times. In fact, the preoperative and postoperative times were nearly identical in both cases and demonstrated minimal variability. However, there was a statistically significant difference between LSG and RSG operative times (p≤0.001). The mean operative time between LSG and RSG was 88±18.6 minutes versus 119±31.6 minutes. The mean time difference was 30 minutes. When analyzing the last 10 robotic cases, the RSG operative time was 99.9 minutes, and the mean time difference narrowed to only 12 minutes. The resulting mean time difference was not statistically significant (p=0.20; Fig. 4).
Robotic versus laparoscopic sleeve gastrectomy case times. min, minutes; pre, preoperative; post, postoperative.
min, minutes; SD, standard deviation.
Robotic set-up time also did not seem to affect surgery start times or turnover times. For both RSG and LSG, there were three operative days where consecutive cases were performed. For 7:30 a.m. start times, robotic cases on average began at 7:31 a.m. in comparison to 7:27 a.m. for laparoscopic cases. Average turnover times between consecutive LSG and consecutive RSG was 33 and 36 minutes respectively.
Discussion
Adoption of the robotic surgery platform has been increasing across different subspecialties, including general and, more recently, bariatric surgery. As in these specialties, the utility of the robotic platform has been questioned. The major deterrents to the use of the robot have been the perceived increased operative times and increased costs. By determining the areas of least adeptness, strategies to create an effective and cost efficient robotic bariatric program can be implemented.
In this study, we chose to focus on RSG as opposed to robotic RYGB because our volumes of sleeve gastrectomies are much higher. Additionally, there is very little literature concerning RSG despite the fact that the procedure represents 38% of the bariatric procedures performed in the United States. 6 In fact, in more than 60 papers written about robotic bariatric surgery, only four papers have focused on RSG. In addition, there is little variation in technique between RSG and LSG allowing us to identify better the areas that require improvements.
Operative time inefficiency
Operative time, from skin incision to skin closure, is one of the most important factors in RSG efficiency. Operative times of RSG in the literature ranges from 89 to 135 minutes while the operative times for LSG ranges from 94 to 114 minutes.7,11–13 Therefore, the reported mean time difference between RSG and LSG is 21 minutes. The majority of these studies have between 19 and 31 cases, except for Romero et al., which had 134 reported RSG cases. 5 Our mean operative time for RSG is comparable at 119 minutes. The mean time difference between our RSG and LSG is slightly higher at 30 minutes. This time difference can partly be explained by our mean operative time for LSG of 88 minutes, which is approximately 10 minutes faster than reported in the literature.7,11–13
There are two other factors that seem to affect the length of the operative time and thus the efficiency of RSG: the learning curve and the docking time. The learning curve is an inevitable rite of passage when initiating a robotic program or performing a new procedure with the robot. It has been demonstrated by Panait that laparoscopic skills transfer to the robot more readily than for laparoscopic naïve surgeons. 14 This in theory should make the transition from laparoscopic to robotic bariatrics smoother and quicker. In our observation, it took our team approximately five cases to reach comparable times with LSG. Incidentally, this is similar to the learning curve needed to obtain proficiency on a robotic simulator. 15 After surpassing our learning curve, as demonstrated by our last 10 cases, the time difference is only 12 minutes between RSG and LSG (Fig. 5).

Robotic sleeve gastrectomy learning curve. min, minute; log, logarithm best fit line.
Docking time is one aspect of RSG that is an additional step to surgery that is not needed in LSG. Docking time is the time from placement of the last port until the time the surgeon is able to begin operating at the console. Docking times have been reported to range from 6.6 minutes to 30 minutes.11,16 In Villalonga's RSG study, the docking times were initially 9.1 minutes but decreased to 6.6 minutes in their second cohort. Unfortunately, we did not accurately record our docking times and therefore cannot comment on its contribution to our cases. Regardless, this is still extra time that is spent during a RSG and can potentially prolong the case.
Cost inefficiency
There have been several studies that have addressed the cost of robotic surgery. A meta-analysis demonstrated that in 9 of 11 published papers, the robot is more expensive than laparoscopic surgery. 7 There are several factors that produce this extra cost. As noted above, robotic procedures in general have longer operative times and thus increased charges for room utilization. Robotic instruments also add significant cost per case because each docked instrument is charged per patient use with a limit of 10 uses. Additionally, the cost of the robot can nearly be double that of traditional laparoscopic surgery when initial purchase and maintenance costs are factored in. 9
Despite this high cost, there are several ways to reduce the cost of robotic surgery. The use of dedicated robotic teams, limiting use of robotic instruments, and efficient utilization of the robot can decrease the overall cost.17,18 Lasser demonstrated that after training a dedicated robotic team, preoperative set-up times could be decreased by an average of 15 minutes. 17 At our institution a dedicated robotic team was already in place when we initiated our robotic bariatric program. This may have contributed to the consistency of our preoperative and postoperative times for RSG, as they were nearly the same from the first five cases to the last five cases. As a result, no difference was noted in the preoperative and postoperative times between RSG and LSG. Robotic set-up time also did not seem to affect first start times or turnover times, as they were similar in both groups. Therefore, preoperative set-up, postoperative breakdown, and turnover time did not seem to affect RSG efficiency in comparison to LSG—a common misconception.
The use of multiple robotic instruments can greatly increase the cost of surgery. On average, the cost of a robotic instrument is $220. 19 Minimizing the amount of instruments used per procedure can significantly decrease the cost per case. In this study, only three instruments were used during the case: the vessel sealing device, the double fenestrated grasper, and the single fenestrated Cadiere grasper. In our last few cases, we were able to decrease this to two instruments by using a reusable laparoscopic triangle liver retractor instead of a robotic grasper. By combining this with a dedicated robotic team, a surgeon can operate more efficiently and perform more procedures in a day.
Limitations
One of the limitations of this study was the lack of docking times in our cases. As a result, we could not calculate its contribution to the operative time. The retrospective nature of the study and the small sample size also limit the conclusions of this study.
Conclusion
The main barrier to improving efficient use of RSG is the overall increased operative time of the case. After overcoming the learning curve, RSG is still slower than LSG by 12–30 minutes. Part of this inefficiency is likely due to the addition of docking the robot and instruments. However, RSG with a dedicated robotic team can be efficiently performed so that three consecutive RSG can be completed by 3:30 p.m. in a given operative day, which we have been able to accomplish for cases 17–19 performed on the same day. More importantly, our experience also demonstrates that the preoperative robot set-up and postoperative turnover does not increase the overall operative time, despite the additional patient preparation and positioning needed for the robotic platform.
Footnotes
Author Disclosure Statement
No competing financial interests exist.