
Abstract
Background:
Treatment of gastrogastric fistula (GGF) has not been consensual. The aim of this study is to evaluate the efficacy of a stepwise approach of GGF in the long term.
Methods:
This is a retrospective case-series study. Thirty-one patients underwent open (71%) or laparoscopic (29%) Roux-en-Y gastric bypass (RYGB), where 20 (64.5%) had a banded pouch. Those 31 cases were referred to the authors' clinic for GGF treatment. The mean time between the primary surgery and GGF diagnosis by endoscopy or radiography was 31 months. Outcomes were evaluated after conservative, endoscopic, and surgical treatment. Mean follow-up was 39.7 months (10–97 months).
Results:
Patients were referred presenting weight regain (100%), epigastric pain (51.6%), and upper digestive hemorrhage (9.6%) due to marginal ulcer (35.5%). GGF was located at the angle of His (51.6%) and two other sites (gastric body and close to the gastrojejunal anastomosis). Etiology was defined in 27 (87%) due to previous acute gastric leak (54.8%) and band erosion (32.3%). Treatment for GGF was conservative (n=11; healing=2, 18.2%) and endoscopic (n=6; healing=4, 66.7%). In the surgical group (n=14), fistula transection by laparoscopy (n=6) and by laparotomy (n=8) were carried out. In this last group, a remnant gastrectomy was done (n=5). Fistula closure was achieved in 13 (92.9%) patients in the surgical group, which had two cases of acute fistula treated by endoscopy. Overall outcomes were symptom control and weight loss.
Conclusions:
GGF has been effectively treated by revisional surgery. Endoscopic management in selected situation has a relatively high success rate.
Introduction
G
GGF treatment has been based on clinical evidence, with scarce data available in the literature. Conservative, endoscopic, and surgical approaches have been described. Conservative management involves noninvasive procedures and the use of proton pump inhibitors (PPI) and sucralfate to heal the ulcers.4,5 Such an approach may lead to resolution of the symptoms and closure of the GGF in cases in the early stages, but it is difficult to determine which patients would benefit from it. 6 D'Hondt et al. reported that in some cases, surgery is not needed. 7 Endoscopic approaches, such as biological glue, clips, and suture have been described. However, Fernández-Esparrach et al. showed that direct attempts to close the fistula utilizing endoscopic clipping and suturing do not have satisfactory long-term results, despite being a minimally invasive treatment. 5 Thus, surgical treatment has been advocated,8,9 also involving specific procedures: fistulous tract resection or remnant gastrectomy.
Due to the low GGF frequency and lack of comparative studies, no consensus has been reached on the best treatment or the group most benefited by each available therapeutic option. Thus, the aim of this study was to evaluate the efficacy of a stepwise approach of GGF in the long term through endoscopic, conservative, and surgical management. The study also analyzed possible etiologic factors and clinical presentations of this complication.
Materials and Methods
This is a retrospective review of a consecutive post-RYGB GGF case series treated at the General Surgery Department of the Hospital das Clínicas (HC), Universidade Federal de Pernambuco (UFPE), Brazil, from 2004 to 2013.
Thirty-one patients (19 female; Mage=37.2 years), who underwent either open (n=22) or laparoscopic (n=9) RYGB took part in this study, where 20 (64.5%) had a banded (ring) pouch. Those primary surgeries were done at HC-UFPE or other Brazilian bariatric surgery institutions before they were referred to the authors' team of surgeons to treat the GGF. The mean time between primary surgery and GGF diagnosis was 31 months (1–120 months); the mean range of body mass index (BMI) in the GGF diagnosis was 32 kg/m2 (Fig. 1 and Table 1).
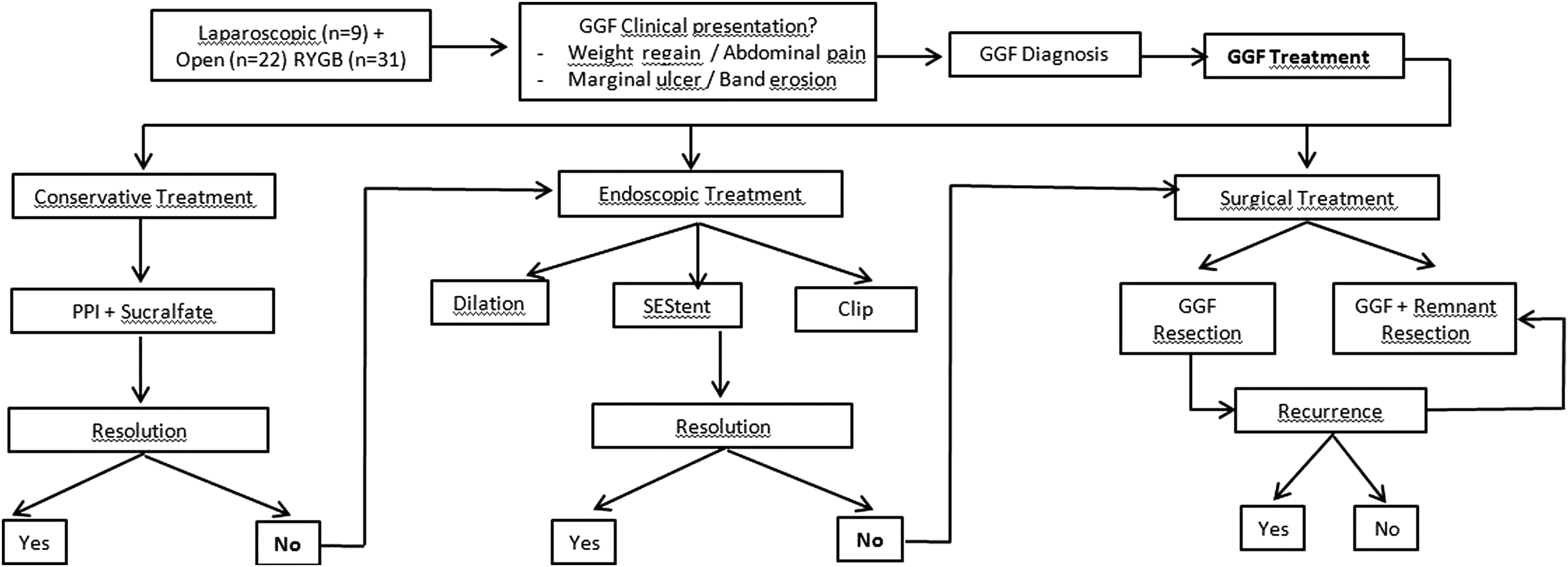
Clinical algorithm for the management of gastrogastric fistula.
p-Value of ratio test comparison (if p<0.05, the ratios are different).
RYGB, Roux-en-Y gastic bypass; GGF, gastrogastric fistula; BMI, body mass index.
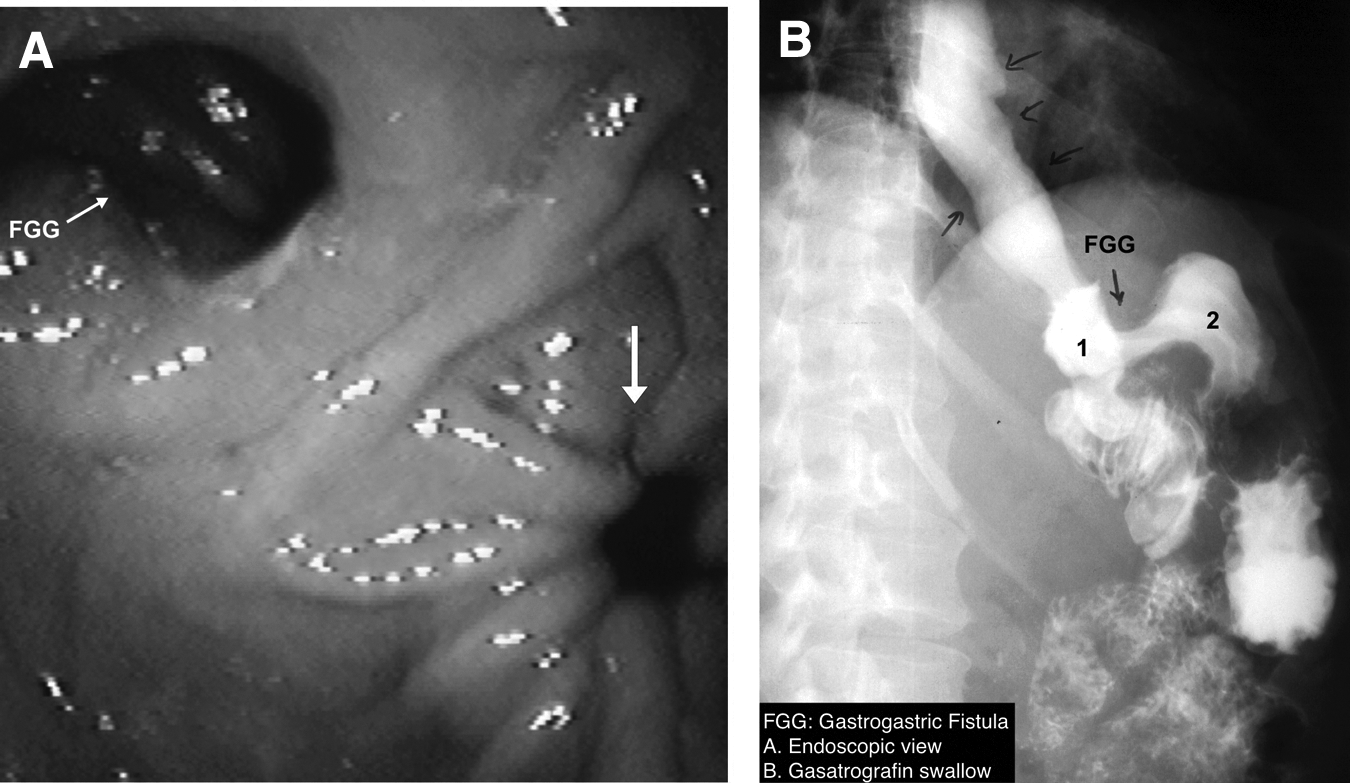
Inclusion criteria were previous RYGB and diagnosis of the GGF by upper gastric endoscopy (UGE) or contrast radiography (Fig. 2).
Variables were collected from paper chart review: BMI at primary surgery, at diagnosis, and after GGF treatment; time elapsed between surgery and GGF diagnosis; presence of gastric band (ring) and its erosion; reference of acute post-RYGB leak; GGF symptoms; and GGF treatment and its results. This study was approved by the local Institutional Review Board.
Diagnostic protocol
Patients with symptoms such as weight regain or epigastric pain underwent UGE to investigate the underlying cause. Upper GI contrast radiography was performed after endoscopic diagnosis of GGF to provide more information on the correlation between surgical and radiologic anatomy.
Once the diagnosis was made, the size of the fistula was classified as <10 mm or >10 mm. The reference was the standard endoscope, which measures 9.8 mm.
Conservative treatment
This therapy was based on a PPI (80 mg/day) regimen, which was applied to all patients; sucralfate (6 g/day) was added to those with marginal ulcer. This approach was indicated for small GGF (<10 mm) in which the diagnosis was made during surveillance endoscopy. Patients were re-evaluated by means of another UGE after 1–2 months. Conservative management was also chosen when patients refused endoscopic or surgical treatment.
Endoscopic treatment
This approach was indicated when GGF was associated with distal stenosis in order to optimize the flow and reduce pressure on the fistula site or when it was <10 mm. The type of procedure was chosen according to the type of narrowing (banded RYGB or stenosis of the gastrojejunostomy) and the anatomical characteristics of the gastric pouch and fistula.
The following techniques were used: self-expandable stent, stricturotomy, clips, and balloon dilation. Thirty-millimeter balloon dilation (Rigiflex®; Boston Scientific, Natick, MA) was performed in patients who had been submitted to silicon banded RYGB. TTS balloon dilation (12–20 mm; Boston Scientific) was performed on those who had been submitted to nonbanded RYGB.
Procedures were done at an endoscopic suite in an outpatient setting under deep sedation in the presence of a consulting anesthesiologist. A standard single-channel gastroscope was used in all procedures (Pentax Medical, Montvale, NJ).
Surgical treatment
Surgery was reserved for patients with weight regain, since previous treatments had failed, and for fistulas >10 mm. It was performed by either laparoscopy or laparotomy, depending on the best choice of two teams of surgeons. The choice of one of them was the resection of the fistulous tract by laparoscopy, and the other team opted for remnant gastrectomy when the patient had been submitted to open RYGB.
Some patients who did not achieve healing of the fistula after conservative or endoscopic treatment were referred for surgical treatment but refused it.
In this approach, gastric pouch and remnant stomach were freed from adhesions and the fistula tract identified. Intra-operative endoscopy was used to spot the fistula tract in those more difficult cases.
In resection of the fistulous tract by laparoscopy, the fistula was resected using a stapler (Ethicon Endosurgery, Cincinnati, OH), with a green load after complete identification of its tract. Section lines were reinforced with an absorbable running suture. Neither glue nor omentum was applied to the staple line. The integrity of the staple line was confirmed with a methylene blue test.
Remnant gastrectomy was done in five cases that had been submitted to open RYGB. This procedure began by duodenum sectioning just below the pylori using a linear stapler. Afterwards, the great curvature was released by ultracision Harmonic® scalpel (Ethicon Endosurgery) until the fistula tract could be found. Finally, this tract was transected by a linear cutter stapler (Fig. 3), and the remnant stomach was fully resected.
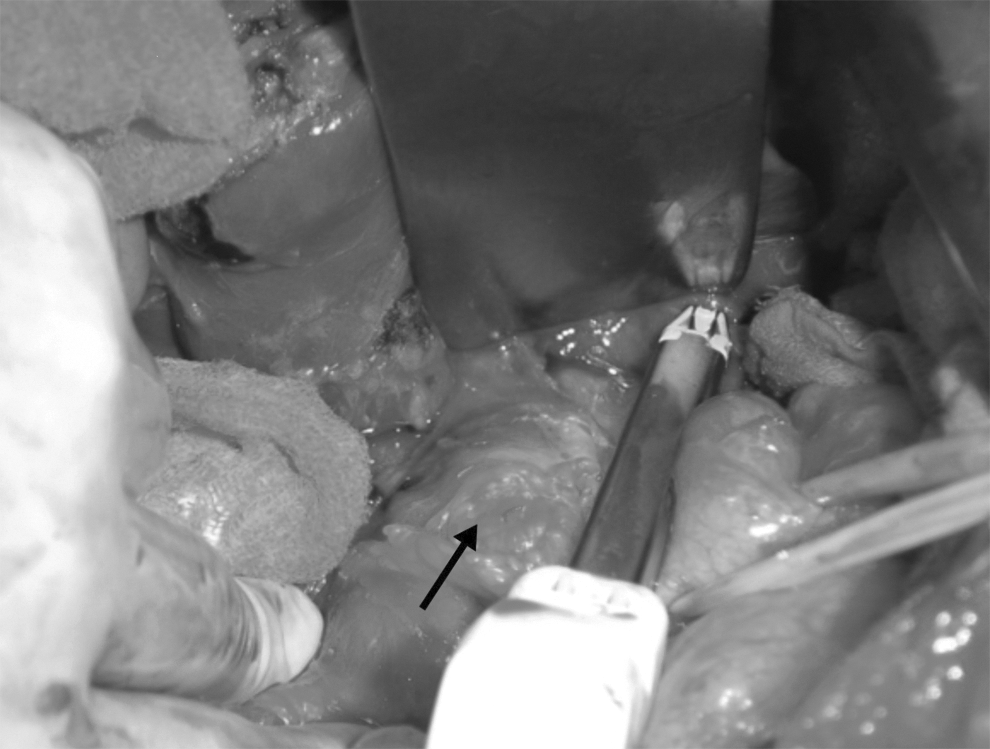
Surgical view of an open resection of a gastrogastric fistula.
The decision to perform only resection of the fistulous tract or perform the remnant gastrectomy as well was down to the choice of surgeon, since the patients were operated by two different teams. All patients with a ring had the device removed.
The fistula was considered healed or closed when leaks were not detected in the esophagus on stomach contrast examination immediately after the treatment and/or 6 months later.
Statistical analysis
SPSS Statistics for Windows was used to analyze the data. The percentage frequencies were calculated from their frequency distributions. Means and ranges were calculated for continuous variables.
Quantitative variables were minimum, maximum, mean, and standard deviation. The chi-square test was used for comparison of proportions. Wilcoxon's test was applied to compare the distribution of BMI in the different phases of the study. A significance level of 5% for all statistical tests was adopted.
Results
By the time they were referred to the authors' team, all 31 patients presented weight regain. In addition, other symptoms were reported, such as epigastric pain (51.6%) and upper digestive hemorrhage (9.6%) due to marginal ulcer (35.5%). The GGF was located at the angle of His (16/51.6%) and two other sites (gastric body and gastrojejunal anastomosis). In 27 patients (87%), the etiology of the GGF was defined: previous acute gastric leak occurred in 17 patients (54.8%), and band erosion in 10 (32.3%; Table 2).
Treatment was conservative in 11 patients, with healing occurring in two patients (18.2%). Treatment was effective at controlling symptoms in five patients (45.5%). Endoscopic therapy was applied in six patients (19.3%), with the following procedures: gastric stent placement (two patients), balloon dilation (two patients), and clip placement (two patients). Fistula closure was achieved in four patients (Table 3).
Twenty-five of the unhealed cases by the other two approaches were referred for revisional surgery in order to close the fistula, of which 11 opted for a nonsurgical approach. In the surgical group (n=14), the following procedures were carried out: fistula transection by laparoscopy (six patients) and by laparotomy (eight patients). In this last group, a remnant gastrectomy was performed in five cases. Fistula closure was achieved in 13 patients (92.8%; Table 3).
Regarding redo surgery complications, two patients developed acute gastric fistula, which was treated by endoscopy, using a stent, with no mortality rate. The first patient underwent an open fistula transection, and the other a remnant gastrectomy.
The mean follow-up after intervention was 39.7 months (10–97 months). Fistula closure was achieved in 19 (61.3%) cases after all three procedures. One patient who underwent GGF resection without gastrectomy experienced recurrence 3 years after revisional surgery.
After conservative and endoscopic management, patients exhibited a small but insignificant weight loss (Fig. 4).

Weight loss before and during RYGB follow-up.
Discussion
Bariatric surgery has been growing over the last 20 years, with satisfactory results. However, some complications, such as a GGF, might occur. 4
In its early years, the RYGB technique did not include gastric division, 10 which was related to GGF in up to 50% of cases. Nowadays, in order to minimize such risk, stapling and section technique is used in all patients. Therefore, in this current study, there were no instances of GGF caused by an undivided gastric wall.
In the present study, the most frequent site of GGF was the angle of His, followed by the gastric pouch and gastrojejunostomy. According to the literature, the proximal segment of the gastric pouch is the most common location (49%), and the gastrojejunostomy is the least common (10%) location of GGF. 5
Leakage secondary to staple line dehiscence is one of the pathogenic mechanisms of GGF.2,4 The percentage of patients with a previous leak was similar to that found in the literature. 11 Intragastric band (ring) erosion seemed to be associated with GGF, being diagnosed in 50% of cases. This process may be due to the inflammatory reaction and stenosis, which was identified in 19.3% of cases.4,12 Marginal ulcer was observed in 35.5% of the sample, and it has been cited as a risk factor because of the contact of gastric acid with the gastric pouch. 13
UGE, gastrointestinal contrast series, and computed tomography are specific examinations for the diagnosis of GGF.4,8,14 The symptoms reported by patients are often inconsistent or unspecific. It was found that nearly half of the cases in this series reported only epigastric pain, usually associated with others symptoms such as weight regain. Symptoms that may suggest marginal ulcers have been reported.4,5,9,10
This fact may imply that diagnosis is often late, resulting in a fistula that has become more difficult to treat. In this series, GGF was identified on average 31 months after primary surgery, earlier than other series.5,15 As the follow-up protocol demands routine sequential postoperative UGE for all patients, it may have led to an earlier diagnosis. Although it might be expensive to recommend routine UGE in the postoperative period, centers that apply this protocol might have earlier identification of postoperative complications.
On a review of the literature, neither the best therapy nor the standard of care is defined. A series of conservative,4,6,7,11,16 endoscopic,5,6,15 and surgical management studies4,6,8,15,16 was analyzed, with different success rates.
Conservative management may lead to resolution of the symptoms and closure of the GGF in cases found early, 6 but it is difficult to determine which patients would benefit from this approach. D'Hondt et al. reported that in some cases, surgery is not needed. 7
Regarding endoscopic treatment, Fernández-Esparrach et al. 5 showed that direct attempts to close the fistula utilizing endoscopic clipping and suturing do not have satisfactory long-term results. On the other hand, Donatelli et al. 17 published a case report of a giant GGF treated by clipping the fistula orifice, with the clip positioned through a colonoscope. In the current series, UGE was used to treat complications related to gastric pouch stenosis; endoscopic dilation and stent placement were performed in two cases, with fistula closure being achieved in both of them. According to these results, endoscopic treatment for GGF should be limited to patients with stenosis as the cause of the fistula (in selected patients).
Shaikh et al. 18 published a review of the several therapeutic modalities for the management of fistula after RYGB. The best results of endoscopic treatment came from the use of a stent, despite a relatively high migration rate. Nevertheless, other available resources are still in the early stages, needing further long-term analysis. Maybe in the future, new endoscopic full-thickness suturing devices may play a better role in the closure of GGF.
When weight regain is the main symptom of GGF, a conservative approach is prone to fail according to a published consensus.4,6 The current debate involves deciding whether GGF resection, as a single approach, is sufficient and appropriate.
Salimath et al. 8 treated 22 patients by laparoscopic fistula tract section associated with remnant gastrectomy, without evidence of recurrence of the fistula or marginal ulcer after a short follow-up of 4 months. No difference in efficacy was reported between the remnant gastrectomy and GGF section, with a lower morbidity for the GGF. 6 Lessons learned from the GGF treatment in vertical banded gastroplasty include the requirement of some kind of gastrectomy in order to improve results and avoid recurrence of the fistula associated with GGF section. 19
Conclusion
GGF can be effectively treated by revisional surgery. Endoscopic management in selected situations has a relatively high success rate.
Footnotes
Author Disclosure Statement
No competing financial interests exist.