
Abstract
Background:
Some institutions and insurance companies mandate a preoperative weight loss regimen prior to bariatric surgery. Previous studies suggest little to no correlation between preoperative and postoperative weight loss for laparoscopic Roux-en-Y gastric bypass (RNYGB). This study examined the impact of preoperative weight change for patients undergoing laparoscopic sleeve gastrectomy (LSG).
Materials and Methods:
A retrospective analysis was performed on patients undergoing LSG at the authors' institution from 2010 to 2012. Patients were grouped based on preoperative weight gain or loss. The correlation between preoperative BMI change and postoperative BMI change was studied, as well as length of surgery.
Results:
Of 141 patients with 1-year follow-up, 72 lost, six maintained, and 64 gained weight preoperatively. Percentage of excess BMI loss at 1 year was not statistically different between those who lost weight and those who gained weight. Percent change in BMI from initial visit to surgery does not correlate with change in BMI at 1 year postoperatively or with length of surgery.
Conclusions:
Preoperative weight loss is not a reliable predictor of postoperative weight loss or shorter operative time after LSG. Potential patients who otherwise meet indications for LSG should not be denied based on inability to lose weight.
Introduction
T
The 1991 National Institutes of Health (NIH) Consensus Development Conference panel recommended that bariatric surgery be considered for well-informed and motivated individuals with acceptable operative risks who have a body mass index (BMI) >40 kg/m2, or >35 kg/m2 with associated medical comorbidities (e.g., diabetes mellitus, hypertension, obstructive sleep apnea). 9 Most insurance providers in the United States cover the cost of bariatric surgery but require a physician-supervised weight loss regimen, 10 despite the lack of conclusive data to support the idea that preoperative weight loss actually improves results and the possibility that this requirement increases dropout rates in patients considering bariatric surgery. 11 The effect of preoperative weight loss on postoperative outcomes is inconclusive, as there are studies reporting a positive relationship,12–14 no relationship,15–17 and a negative relationship11,18 between preoperative and postoperative weight loss in patients who have undergone laparoscopic RNYGB. A Medline search revealed no studies reporting the effect in patients who have undergone LSG. Thus, there is still a need for data on the effectiveness of preoperative weight loss requirements and the relationship between preoperative and postoperative weight change, especially in patients who have undergone LSG.
Materials and Methods
After obtaining Institutional Review Board approval, a retrospective analysis was performed on patients undergoing LSG at the authors' institution between 2010 and 2012. All of these patients were required to complete a multidisciplinary bariatric surgery pathway prior to undergoing the procedure. Initially, the patients had to attend a group meeting and information session where initial weight and BMI were obtained. This was followed by psychological evaluation, nutritional evaluation and teaching, and esophagogastroduodenoscopy (EGD) to evaluate for Helicobacter pylori infection or other notable pathology. Some patients underwent right upper quadrant ultrasound to investigate for gallstones, depending on the surgeon's preference.
The 141 identified patients were first grouped based on preoperative weight gain or loss. Preoperative weight change was defined as the difference in weight upon entering the multidisciplinary bariatric surgery pathway and weight at the time of surgery. Student's t-test was performed to evaluate for any differences in these groups. Preoperative factors evaluated were age, percentage of patients who were female, BMI at the time of entering the bariatric surgery pathway, BMI at the time of surgery, and length of time from initial weigh-in to time of surgery (duration of bariatric pathway). The primary outcome evaluated was percentage of excess BMI loss (%EBMIL) at 1 year follow-up. The secondary outcome investigated was length of surgery.
To investigate further for differences in those who gained or lost the most weight, patients were divided into groups based on percentage of BMI change preoperatively: > –5%, –2 to –5%, –0.1 to –2%, 0%, 0.1 to 2%, 2–5%, and >5%. Analysis of variance (ANOVA) was used to evaluate any differences in these groups using the same preoperative factors and outcomes. Linear regression analysis was used to study the correlation between preoperative BMI change and amount of postoperative BMI change in these patients.
Results
The 141 patients with at least 1 year follow-up were predominately female with a wide range of ages and BMIs represented (see Table 1). Of these patients, 72 lost weight preoperatively (mean BMI decrease = 2.8%), six maintained weight, and 64 gained weight preoperatively (mean BMI increase = 1.8%). A comparison between those who lost weight preoperatively and those who gained weight preoperatively showed no statistical difference in the percentage of patients who were female, initial BMI, BMI at time of surgery, or duration of bariatric pathway. Patients who lost weight preoperatively were, on average, 5 years older than those who gained weight preoperatively. Though this was a statistically significant difference, this difference was no longer present when patients who remained the same weight were included. %EBMIL at 1 year was not statistically different between those who lost weight and those who gained weight preoperatively (74.2% vs. 73.4%, respectively, p = 0.848; Table 2).
N = 141; 89% female.
BMI, body mass index.
Statistically significant, p<0.05.
%EBMIL, percentage of excess BMI loss.
When patients were divided into groups based on percentage of BMI change preoperatively, there were no statistical differences identified (see Table 3). A linear regression analysis demonstrated that percent change in BMI from initial visit to surgery does not correlate with change in BMI at 1 year postoperatively (p = 0.77; Fig. 1) Mean operative times were 96.9 min and 95.6 min for those who lost weight and those who gained weight, respectively. Preoperative BMI change did not correlate with length of surgery (p = 0.87; Fig. 2).
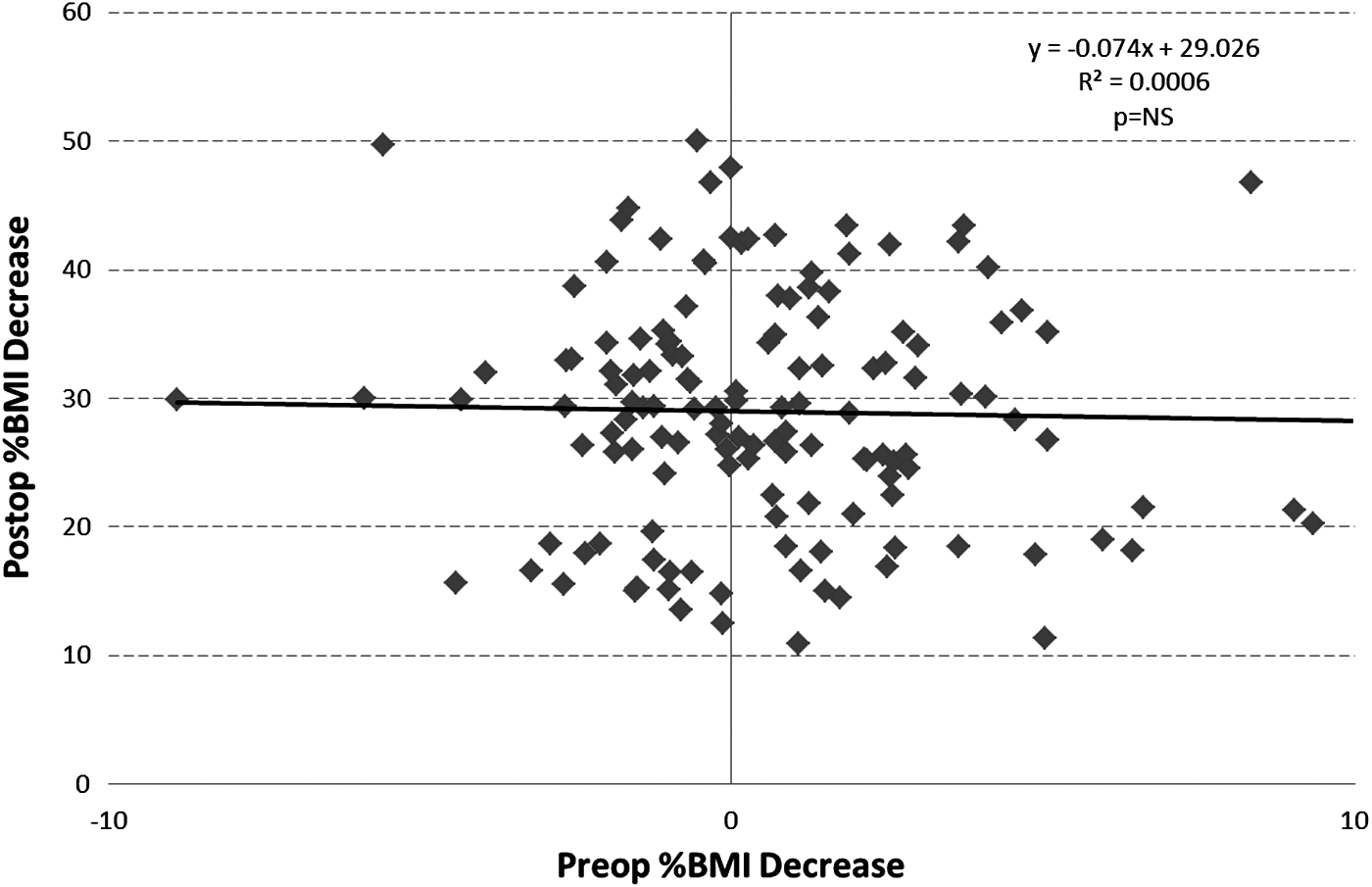
Postoperative body mass index (BMI) change correlated with preoperative BMI change.
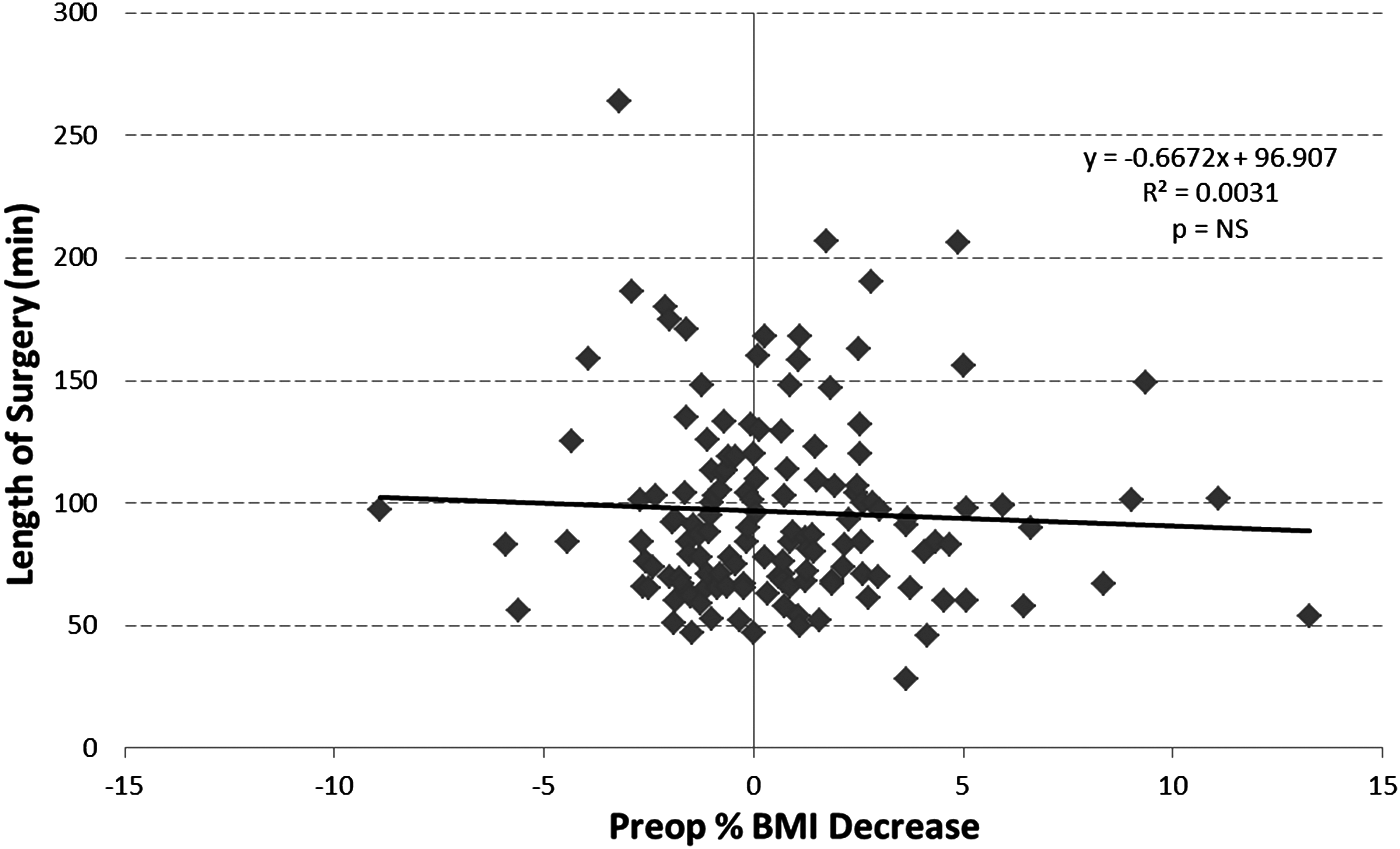
Length of surgery correlated with preoperative BMI change.
Discussion
LSG is an effective method of weight loss and improvement of comorbidities of obesity. Many insurance providers and surgical practices require weight loss prior to undergoing bariatric surgery, often suggesting that preoperative weight loss demonstrates the appropriate motivation required for postoperative success. At the authors' institution, surgical candidates must complete a bariatric pathway prior to approval for surgery. This includes mandatory informational meetings, nutritional teaching and evaluation including a quiz, and psychological evaluation. Preoperative weight loss is not a requisite for surgery. Nonetheless, a significant number of surgical candidates lost weight preoperatively. The present findings suggest that preoperative weight change, whether loss or gain of weight, is not predictive of postoperative change in BMI in those who undergo LSG.
Previous studies of patients undergoing RNYGB suggest that preoperative weight loss decreases operative time and potentially morbidity of the procedure. In patients undergoing LSG in the present study, preoperative weight change did not correlate to longer or shorter operative time, despite a wide range of BMI in the patient population. As others have noted, two large insurance companies state that they require supervised weight loss regimens to minimize morbidity and mortality and to improve surgical outcomes. This is despite evidence that these requirements may be ineffective in actually promoting preoperative weight loss. 19 This study suggests that preoperative weight gain may not increase morbidity or decrease surgical outcomes in patients undergoing LSG.
The results of this study apply to candidates for LSG but are also in agreement with some previous studies of patients undergoing laparoscopic RNYGB and, before that, studies of patients undergoing open RNYGB or vertical banded gastroplasty.14,16 A priori power analysis was not performed given the difficulty in finding standard deviations for length of surgery, %EBMIL, and %BMI decrease in prior studies of LSG, as well as a predetermined sample size based on available subjects. Sensitivity power analysis does suggest a small minimal detectable effect (d = 0.34), even at only 50% power. Relatively narrow confidence intervals also suggest adequate sample size. Admittedly, this study only includes short-term follow-up and does not investigate the effect of preoperative weight change on postoperative improvement of comorbidities. A larger prospective study with longer follow-up and analysis of improvement of comorbidities may be helpful in answering this question.
Conclusions
The results of this study suggest that preoperative weight loss is not a reliable predictor of postoperative weight loss after LSG. Losing weight preoperatively also did not predict shorter operative time. Thus, potential patients who otherwise meet indications for bariatric surgery should not be denied this procedure based on inability to lose weight preoperatively.
Footnotes
Author Disclosure Statement
No competing financial interests exist. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Army, DOD, or the U.S. Government.