
Abstract
Purpose:
Changes in weight and body composition, and rates of parameter change within and between genders, were studied preoperatively and serially within the first postoperative year after Roux-en-Y Gastric Bypass (RYGB). Analysis included 146 patients (115 women and 31 men) who were compliant with all visits. Preoperative variables included weight (Wt), body mass index (BMI), and body composition evaluated using ElectroLipoGraphy. Postoperatively, changes in those variables, percent excess weight loss (%EWL), and %Lean Lost (lean mass lost/weight loss) were evaluated.
Main Findings:
Both genders demonstrated significantly favorable Wt, BMI, %EWL, and body composition changes. %Lean Lost was the only parameter that did not significantly change for both genders. Between-gender changes were significant for all variables except BMI, %EWL, fat mass, and lean mass lost. No slopes of changes differed significantly between genders.
Principal Conclusions:
RYGB effectively accomplishes favorable weight and body compositions for both genders during the first postoperative year. Findings were used to suggest gender-specific, evidence-based clinical practice guidelines to assess body composition changes. Monitoring changes can help both genders achieve a healthier body weight primarily from fat mass loss while sparing lean mass.
Introduction
O
Obesity itself is recognized as a chronic disease associated with increased mortality rates and significant psychological and medical comorbidities. 4 The spectrum of treatment options includes reduced caloric intake coupled with exercise, pharmacologic therapy, and bariatric surgery. Bariatric surgery is recognized as the most successful and durable treatment for patients with severe obesity. 4 Despite the global downward trend of Roux-en-Y Gastric Bypass (RYGB) from 2003 to 2008 to 2011, globally it remained the most commonly performed metabolic/bariatric surgical procedure in 2011 at 46.6%. 5
It has been recognized that weight loss (WL) after bariatric surgery should ideally be from fat mass (FM) and that analyzing body composition serially following bariatric surgery is essential.6,7 The role of fat tissue's endocrine influence in the pathogenesis of obesity, insulin resistance, and cardiovascular disease has been discussed. 8 RYGB has been recognized to produce a positive effect on reduction of total and trunk adiposity, and FM reduction following RYGB has been correlated to improved insulin sensitivity.9,10 By contrast, lean body mass (LM) comprises the majority of the body's metabolically active tissue and has been noted to be the best predictor of basal metabolic rate (BMR). 11 Following RYGB, LM was found to be the best predictor of BMR, and changes in LM correlated with changes in BMR presurgery to 12 months following surgery.12,13
Body composition assessment recognizes that men are leaner than women, defining obesity in terms of percent body fat (%BF) as ≥25% for men and ≥32% for women—a 7% difference. 14 Some studies, which examined weight and body composition changes in exclusively RYGB populations, included only a single gender10,15,16 and one of these tracked changes in FM and LM for women by site serially 1 year following RYGB. 16 Other RYGB studies combined genders in the populations studied despite inherent gender difference in body composition.9,17–19 Some RYGB studies examined gender influence on WL.6,7,20,21 One of them reported 1-year gender-specific weight and body composition changes, but did not report serial changes throughout that 1 year. 7 Two RYGB studies did examine gender-specific serial weight and body composition changes. Of these two studies, one reported and compared changes for both genders serially for 12 months. 13 The other also compared serial rates of change between genders, but only through 6 months following surgery. 12
The purpose of this study is twofold. First, this study seeks to examine and compare weight and body composition changes and their rates of change, within and between genders preoperatively and serially within the first postoperative year following RYGB. The second purpose of this study is not only to examine those changes but also to apply findings to create evidence-based practice guidelines with which to evaluate body composition following RYGB in the interest of both losing BF and sparing LM. Such information has not yet been offered within existing guidelines to manage nutrition following bariatric surgery.4,22,23
Materials and Methods
This study was approved by the hospital institutional research review board, and a waiver of informed consent or authorization for use of patient information necessary to conduct the study was granted. All patients were legal adults above the age of 18. Data were prospectively collected from outcome measures routinely captured by the dietitian. Only records of patients who had undergone RYGB and who were compliant with 3-, 6-, and 12-month postoperative visits were included in the study. The time frame encompassed May 2007, when the dietitian began to perform body composition assessment, to February 2015, when data were submitted for analysis. All cases were performed by a single surgeon at our institution.
Patient height (Ht) was measured in centimeters (cm) without shoes during initial patient visit using a wall-mounted stadiometer. Weight (Wt) was measured in kilograms (kg) without shoes or outerwear on one of three office scales calibrated annually for accuracy. When surgery was scheduled, preoperative weight value was recorded.
The team dietitian completed all body composition evaluations. %BF was measured using ElectroLipoGraphy®, a form of bioimpedance analysis (BIA), according to manufacturer instructions using with patients standing. ElectroLipoGraphy has been validated against hydrostatic weighing for persons weighing up to and including 227.3 kg. 24 This weight qualification did not exclude any patients from the study population. FM was then calculated as: FM = Wt × (%BF/100) and lean mass (LM) as: LM = Wt−FM. Excess body weight (EBW) was calculated as the difference between preoperative weight and the midpoint of the medium frame range of ideal body weight (IBW) for height and gender from 1983 Metropolitan Life Tables 25 : EBW = preoperative Wt−IBW. Midpoints of IBW ranges were calculated from the table, adjusting for the fact that the tables present IBW ranges assuming 1-inch heels. BMI was calculated as: BMI = Wt (kg)/Ht (m2).
Postoperative variables evaluated at 3, 6, and 12 months included Wt, absolute WL, BMI, percent excess weight loss (%EWL), %BF, FM, fat mass loss (FML), LM, lean mass loss (LML), and the percentage of WL contributed by LML (%Lean Lost). WL was calculated as the difference between preoperative and postoperative weight. Percent excess weight loss was calculated as: %EWL = (WL/EBW) × 100. Fat mass loss was calculated as: FML = preoperative FM−postoperative FM, and lean mass loss as: LML = preoperative LM−postoperative LM. Percent Lean Lost (%Lean Lost) was calculated as: %Lean Lost = (LML/WL) × 100.
ANOVA one-way analysis with repeated measures was used to compare changes in the measured parameters over time for each gender. ANOVA two-way analysis was applied to analyze the changes in time between genders by regression analysis. Evaluation of Y-intercepts and plots of regression lines were used to compare postoperative rates of change of the parameters within and between genders. All statistical analyses were performed using SPSS software, and results were considered significant with a p < 0.05.
Results
In total, 146 patients (115 women and 31 men) of the 279 laparoscopic RYGB procedures completed as the primary procedure in this time frame were included in the analysis. Mean preoperative age (years), EBW (kg), and BMI (kg/m2) was 46.7, 65.4, and 47.4 for women and 49.4, 81.5, and 48.3 for men, respectively. Table 1 describes preoperative and postoperative outcomes for all recorded and calculated variables.
%BF, percent body fat; BMI, body mass index; %EWL, percent excess weight loss; FM, fat mass; FML, fat mass loss; LM, lean mass; LML, lean mass loss; %Lean Lost, percent Lean Lost; M, men; Wt, weight; WL, weight loss; W, women.
Examining changes within genders, both genders experienced significant downward trends (p < 0.001) in Wt, BMI, %BF (Fig. 1), FM, and LM. Review of information presented in Table 1 reveals that while %BF results for both genders initially qualified for obesity classification, neither gender met those qualifications at 12 months after surgery. 14 Both genders also experienced a significant upward trend for WL (Fig. 2), %EWL, and FML (p < 0.004 for FML for men and p < 0.001 for FML for women; p < 0.001 for WL and %EWL for both genders). Results for LML were significant for women, but not for men (p < 0.001 and p < 0.270, respectively). Percent Lean Lost (Fig. 3) was the single parameter that failed to change significantly over time for both genders (p < 0.990 for women and p < 0.714 for men).

%Body fat.
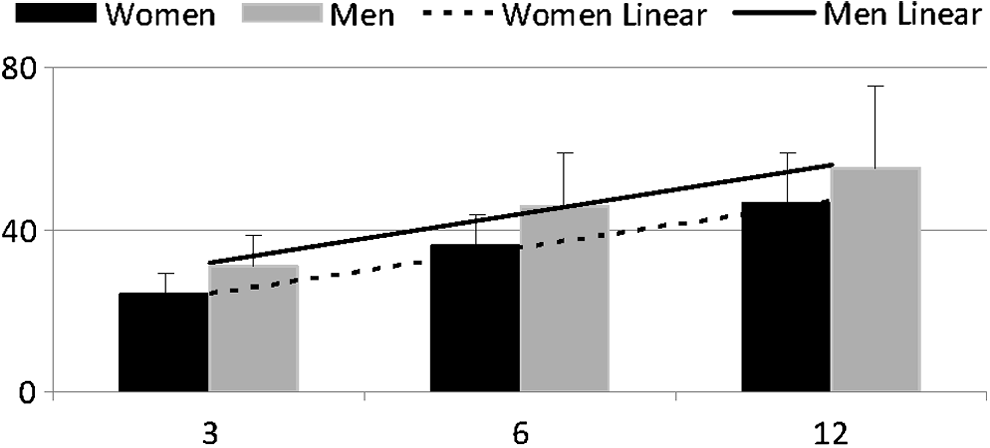
Weight loss (kg).
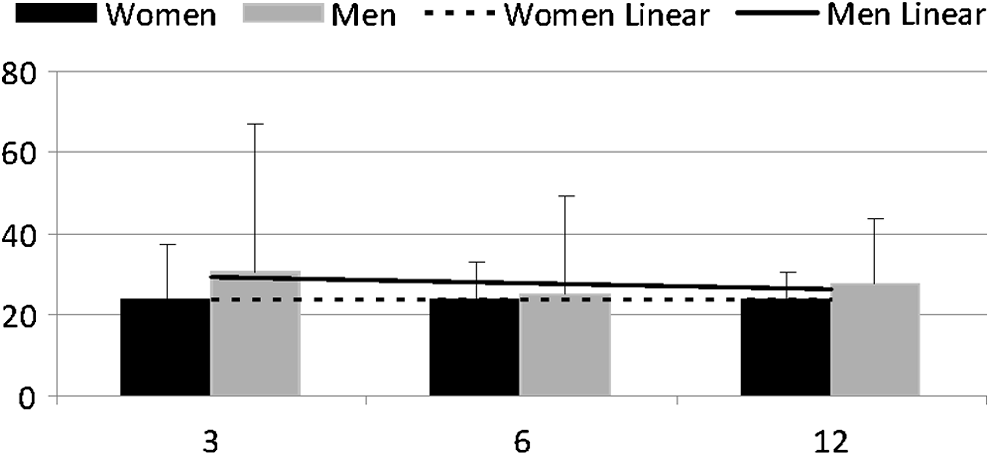
%Lean Lost.
Comparing results between rather than within genders, differences over time were significant (p < 0.001) for Wt, %BF (Fig. 1), LM, WL (Fig. 2), and FML. Among these changes, male outcomes were higher than female outcomes for Wt, LM, WL, and FML. %BF (Fig. 1) was the single outcome which was higher for women than for men. Differences between genders compared over time were not significant for BMI (p < 0.520), FM (p < 0.142), %EWL (p < 0.435), and LML (p < 0.077). An unexpected finding was that between-gender comparison of %Lean Lost over time also reached statistical significance (Fig. 3, p < 0.032).
Table 2 shows that the Y-intercepts for women and men were significantly different (p < 0.001) for all parameters except BMI (p < 0.304). While the starting points, as well as the between-gender changes over time, were significantly different for Wt, %BF, LM, WL, and FML, none of the slopes of parameter changes over time differed significantly (Table 2).
Discussion
Unique to this study are the comparisons of weight and body composition changes, and their rates of parameter change, within and between genders for a full year following RYGB. Comparison between genders of parameter rates of change over time was previously examined for only 6 months following RYGB. 12 Also unique is the application of this study's findings to the formulation of gender-specific guidelines with which to evaluate body composition following RYGB. A third unique aspect of this study is the identification of the %Lean Lost parameter, the ratio of LML to overall WL, as the singular parameter that failed to change significantly over time for both genders. This observation can be utilized to formulate a research-based method to monitor sparing of LM following RYGB.
While this study was unique in its comparison of weight and body composition results, and their rates of parameter change, within and between genders for a full year following RYGB, results of other studies generally corroborated with those of this study. The gender-specific study which examined outcomes only at 12 months following RYGB also found that each gender experienced significant changes in Wt, BMI, FM, LM, and %EWL. 7 This study and another 6-month RYGB study showed that not only did each gender demonstrate significant losses for the parameters of Wt and LM over time, but also there was a significant decline for the parameter of %BF over time. 12 It was also true in that study and in this study that while Y-intercepts differed significantly between genders for those same parameters of Wt, LM, and %BF, there were no significant differences between genders in the rate of these parameter changes. 12
Significant downward-trending results over time for Wt, %BF, and FM were generally recognized in many other studies.7,9,10,15,16,18 This study's findings that men weighed significantly more than women preoperatively and at all postoperative points of measure and lost significantly more weight over the study period was corroborated in other studies.7,13,20
The Y-intercepts for FM were significantly different between genders in this study, but not so in a RYGB study of 6 months. 12 Unique to this study, although, was the lack of significant difference between genders for changes in FM over time.
The findings of this study can also be used to suggest the 12-month postoperative %BF goal of <25% for men and <32% for women. These suggested gender-specific guidelines are based on four points. One is the recognition that healthy body composition is defined differently for men and women. Obesity has been defined as ≥32% for women and ≥25% for men. 14 Second is the recognition that in both this study (Table 2) and in the Carey et al. study, 12 %BF Y-intercepts differed significantly between genders following RYGB. Third, this study contributed the additional finding that the %BF parameter differed significantly between genders over the 12-month study period (Fig. 1). So, although %BF rates of change can be expected to be similar for both genders after RYGB, guidelines to evaluate preoperative and postoperative %BF should be gender specific. Finally is the recognition that these goals can be achieved. Body composition criteria qualified both men and women as obese initially in this study, but neither fell within that category at 12 months after surgery. In another study, %BF for men and women transitioned similarly in 12 months time. 7 The significant decline in %BF was achieved for each gender in this study (Table 1), and in other studies.12,18
Also unique to this study was the identification of %Lean Lost as the single parameter that did not significantly change for both genders when followed serially in the year following RYGB and the recognition that monitoring it can be useful to ensure sparing of LM. Based on this study's results (Table 1) and the recognition that both the Y-intercept (Table 2) and between-gender comparison over time for %Lean Lost were significantly different, a gender-specific guideline of reaching <25% for women (so ¼ of WL attributed from LM) and <33% for men (so <1/3 of WL attributed from LM) can be considered as achievable. It was an unexpected finding in this study that, despite high standards of deviation (Table 1), the gender comparison of the %Lean Lost variable reached statistical significance. Examination of LML raw data shows greater variability for men, ranging from one value of LML of 30.0 kg at 12 months to another value of an actual 32.7 kg LM gain at 6 months. This variability could have contributed to the unexpected finding that the %Lean Lost variable differed significantly between genders. Repeat analysis in the future with additional data would help to clarify whether or not %Lean Lost outcomes significantly vary between genders over time.
Other studies did recognize the predominance of FM contributing to overall WL, but none identified the %Lean Lost variable, nor tracked it serially following RYGB. One RYGB 12-month study reported the nongender-specific result that 75.2% of WL was primarily from FM. 13 Another 6-month study, which combined genders in the population, noted that BF corresponded to 77.1% of total WL. 17 Two other RYGB studies, which did examine gender-specific parameters, recognized simply that WL was primarily from FM.6,7
Reported LM changes following RYGB have been variable. Unique to this study were the findings that men and women had significantly different Y-intercepts for LM, that each gender showed significant changes in LM over time, that the difference in LM between genders over time was significant, and that the difference in the rate of LM between genders lacked significance. In a RYGB study that evaluated outcomes at 12 months, LM changes for both genders reached statistical significance. 7 In two studies with female populations, changes in LM reached significance from preoperative measurement through 6 months, but not from 6 to 12 months.15,16 In another study examining a female population, LM moderately decreased preoperatively to 3 months, but stabilized thereafter through the 24-month study period. 10 In two studies, which reported combined gender results, changes in LM were significant through 6 months.13,18 One of these studies continued the study period through 12 months and found a slight LM gain from 6 to 12 months. 13
Only this study examined the parameters of FML, LML, and WL. In this study, men and women had significantly different Y-intercepts for all variables. Changes in FML and WL over time were significant for both genders; both the variables of FML and WL differed significantly between genders over time, but the rates of parameter change for both variables did not differ significantly over time between genders. Changes in LML over time reached statistical significance only for women in this study, yet there was no significant difference in LML between genders over time. The inability for this study's upward trend in LML for men to reach significance over time could have been related to small sample size.
BMI trended significantly downward in this and in other studies.9,10,12,13,16 In a RYGB study that reported gender-specific changes at 12 months, BMI changed significantly over time for each gender, which was also a finding in this study. 7 The finding that there were no significant differences between genders in regard to either the Y-intercept or the changes in BMI over time was singular to this study.
%EWL comparisons have been variably reported. Changes over time for both genders were significant in this study and in another RY study, which examined 12-month outcomes. 7 This study showed no significant difference between genders for changes in %EWL over time. However, in two studies, which examined 12-month RYGB results, male gender was associated with suboptimal %EWL in one study, 21 while another found male gender to be a predictor of higher %EWL. 20
Monitoring body composition changes following bariatric surgery is a more specific outcome measure than is monitoring weight, BMI, or %EWL, yet routine body composition evaluation requires practicality. One study found body composition changes following RYGB to be comparable between magnetic resonance imaging and BIA, while another recognized BIA as comparable in accuracy to dual-energy X-ray absorptiometry following nonsurgical WL.19,26 BIA, and specifically ElectroLipoGraphy, has been elsewhere used to evaluate body composition following RYGB.6,7
This study's strength lies in its unique examination and comparison of weight and body composition changes, and their rates of change within and between genders, preoperatively and serially for a full 12 months following RYGB. A valuable outcome of the study was the identification of the %Lean Lost variable, which has not been previously evaluated. Yet another benefit was utilization of the %Lean Lost outcome, together with %BF outcomes, to suggest evidence-based guidelines with which to evaluate body composition changes following RYGB. These guidelines can be utilized to monitor WL in favor of losing primarily FM and sparing LM. Such guidelines have not been previously offered.
Of note, however, is that rates of parameter change in this study were examined over time rather than between specific intervals, which enabled trend identification, but did not identify specific rates of change between interval points, as was elsewhere examined.12,16 This study also measured overall body composition, but did not specify body sites, as was done elsewhere. 10 Although practical to use in the clinical setting, the instrument does not differentiate lean tissue as bone or muscle nor is the instrument validated past a body weight of 227.3 kg. Body composition evaluation, then, would be delayed should a patient enter the program at a higher body weight. Genders were also not equitably represented in this study, which was likely partially influenced by the observed tendency of men's failure to return for serial follow-up as consistently as did women.
Conclusions
RYGB is an effective tool to accomplish WL and favorable body composition changes for both genders in the first postoperative year. Both genders lose significant weight and fat at similar rates while adequately preserving LM. Identifying trends and outcomes enables formulation of a framework with which to assess weight and body composition changes following RYGB. That framework should include gender-specific 12-month and lifelong %BF and %Lean Lost goals.
Following RYGB, monitoring identified parameters will equip the practitioner to help guide patients who initially qualified for bariatric surgery toward a healthier weight and body composition. Monitoring these factors preoperatively, throughout the immediate postoperative year, and in the long term will help to sustain positive outcomes. Considering the global trend toward increased frequency, future research may consider similar outcome review and development of weight and body composition goals following SG. 5 Given the variation in reported changes in LM following RYGB, future research may help to identify factors, which will help to optimize postsurgical sparing of LM.
Footnotes
Acknowledgments
The authors thank P. Jeffrey Knopp for his support and technical assistance, Karen B. Holl for her editorial assistance and expertise, and Judy Knight, MLS, AHIP for her research expertise and encouragement. Please note that the authors obtained permission in writing from these people before article submission.
Author Disclosure Statement
No conflict of interest exists for any author of the submitted article, “Gender-Specific Weight and Body Composition Changes following Roux-en-Y Gastric Bypass.”