
Abstract
Background:
Bariatric surgery is a field in rapid evolution with continuous attempts by surgeons to offer procedures that achieve patients' objectives. The idea came out of a new combined bariatric procedure. The procedure is a hybrid of sleeve gastrectomy and gastric bypass, in which a sleeve gastrectomy is followed by a side to side gastrojejunal anastomosis combining advantages of both procedures: achieving restriction and malabsorption.
Materials and Methods:
Forty morbidly obese patients were randomly divided into two groups. Hybrid group: Twenty patients underwent the hybrid operation, which is a combined laparoscopic antrum preserving sleeve gastrectomy with loop gastrojejunostomy. Laparoscopic sleeve gastrectomy (LSG) group: Twenty patients underwent laparoscopic sleeve gastrectomy. The two groups were followed and assessed in several criteria (operative time, pressure measurement, duration of hospital stay, postoperative complications, weight loss, prevalence of gastroesophageal reflux disease (GERD), and food tolerance).
Results:
The hybrid procedure achieved higher %EWL compared with LSG. The study also showed that the intragastric pressure was lower in the hybrid group compared with the LSG group. It also showed a positive correlation between intragastric pressure and GERD score and a negative one between intragastric pressure and Suter's food tolerance score.
Conclusion:
The hybrid procedure achieved higher %EWL, lower intragastric pressure, and higher food tolerance scores compared with LSG. In addition, preservation of antrum carries the advantage of maintaining the access to the biliary tree through endoscopic retrograde cholangiopancreatography, an advantage over gastric bypass.
Aim of Work:
To assess the added value obtained by adding gastrojejunostomy to sleeve gastrectomy regarding excess weight loss, reflux symptoms, and food tolerance.
Introduction
O
Metabolic and bariatric surgery is the only intervention that has been shown to have consistent, long-term weight loss results and significant improvements for comorbid conditions in the severely obese population. 2
Surgical solutions are rapidly increasing, and recent approaches start to replace the already established operations. Distinguished from other procedures, sleeve gastrectomy seems to be the leading procedure in the near future. This is attributed to many factors, including relative simplicity of the procedure, lower cost, reasonable outcome in terms of weight loss and improvement of the associated comorbidities, and the available conversion options in case of unsatisfactory outcome. 3
Another procedure is the mini gastric bypass, which can be applied either as a primary procedure or as a secondary solution after a failed sleeve gastrectomy. 4
Several studies discussed the combination of sleeve gastrectomy (as a restrictive element), with malabsorptive elements, to augment its metabolic and/or weight loss effects.
In 2010, Sánchez-Pernaute et al. published the 3-year postoperative results of their innovative single anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S technique). This operation entails transection of the first part of the duodenum after construction of a sleeve-like stomach. The transected duodenum is then anastomosed to an ileal loop, with the anastomosis lying 200 cm proximal to the ileocecal junction. 5
In 2014, Lee et al. 6 published results of 50 morbidly obese patients who underwent a similar procedure called single-anastomosis duodenal–jejunal bypass with sleeve gastrectomy (SADJB-SG). They referred to it also as a short or mini duodenal switch. It entails a duodenojejunal rather than the duodenoileal bypass performed by Sánchez-Pernaute et al.
In the same year, Mui et al. published 1-year follow-up results of a case report for a novel technique, involving a loop gastroileostomy, with the anastomosis constructed at 250 cm from the ileocecal junction. They claim that tailoring of this anastomosis will reduce the sleeve tube pressure, which plays a central role in postsleeve gastrectomy leakage. 7
So, a combination of both procedures (sleeve gastrectomy and mini gastric bypass) might provide a better control in two separate endocrine hormonal systems, which are important in the control of glucose and weight loss after bariatric procedure. 8
Patients and Methods
Study design and sample size
In this prospective randomized controlled study, 40 morbidly obese patients were selected in the Cairo University Teaching Hospital between March 2016 and January 2017 after failure of conservative therapy.
They were randomly divided into two groups.
Hybrid group: Twenty patients underwent the test operation, which is a combined laparoscopic sleeve gastrectomy with loop gastrojejunostomy.
Laparoscopic sleeve gastrectomy (LSG) group (control group): Twenty patients underwent the standard laparoscopic sleeve gastrectomy.
Inclusion criteria
All the participants with body mass index (BMI) ≥40 or 35–40 kg/m2 with comorbidity in which surgically induced weight loss is expected to improve the disorder, with no specifications of age or gender, were included.
Exclusion criteria
Candidates with previous gastric surgery and patients suffering from any severe psychiatric illness were excluded from the study.
Data collection and consent
Conflict of interest disclosure, ethical statement, and consent statement
“Conflict of Interest: The authors declare that they have no conflict of interest.”
“Informed consent was obtained from all individual participants included in the study.”
Ethical Approval “All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.”
All patients were subjected to full clinical preoperative evaluation as well as investigations. Patient demographics, including age, gender, and BMI were recorded. Clinical evaluation aimed at the assessment of degree of obesity and detection of associated comorbidities like hypertension and diabetes mellitus. Informed consent was obtained from all individual participants included in the study. The gastroesophageal reflux disease (GERD) symptoms were recorded before the operation using the GERD score questionnaire shown in Table 1.
Severity scale: 0 = not at all; 1 = mild; 2 = moderate; 3 = severe.
Frequency scale: 0 = absent; 1 = symptoms occurred once a month; 2 = symptoms occurred once a week; 3 = symptoms occurred 2–4 times a week.
The scores for severity and frequency were multiplied together, resulting in scores from 0 to 12 for each symptom, with a total maximum score of 72 and a minimum score of 0. Higher scores indicated more severe symptoms.
Investigations
Laboratory investigations: CBC, FBS, ± (HBA1C), renal functions, liver functions, and coagulation profile.
Cardiac assessment: ECG and Echocardiography.
Abdominal ultrasound.
Respiratory function tests.
Patients were randomly divided into two groups (sealed envelope system), after obtaining informed consent and explaining the procedure to the patient.
Hybrid group: Twenty patients underwent the hybrid procedure of combined laparoscopic antrum preserving sleeve gastrectomy (preserving about 7 cm of antrum proximal to pylorus) with loop gastrojejunostomy (Figs. 1 and 2).
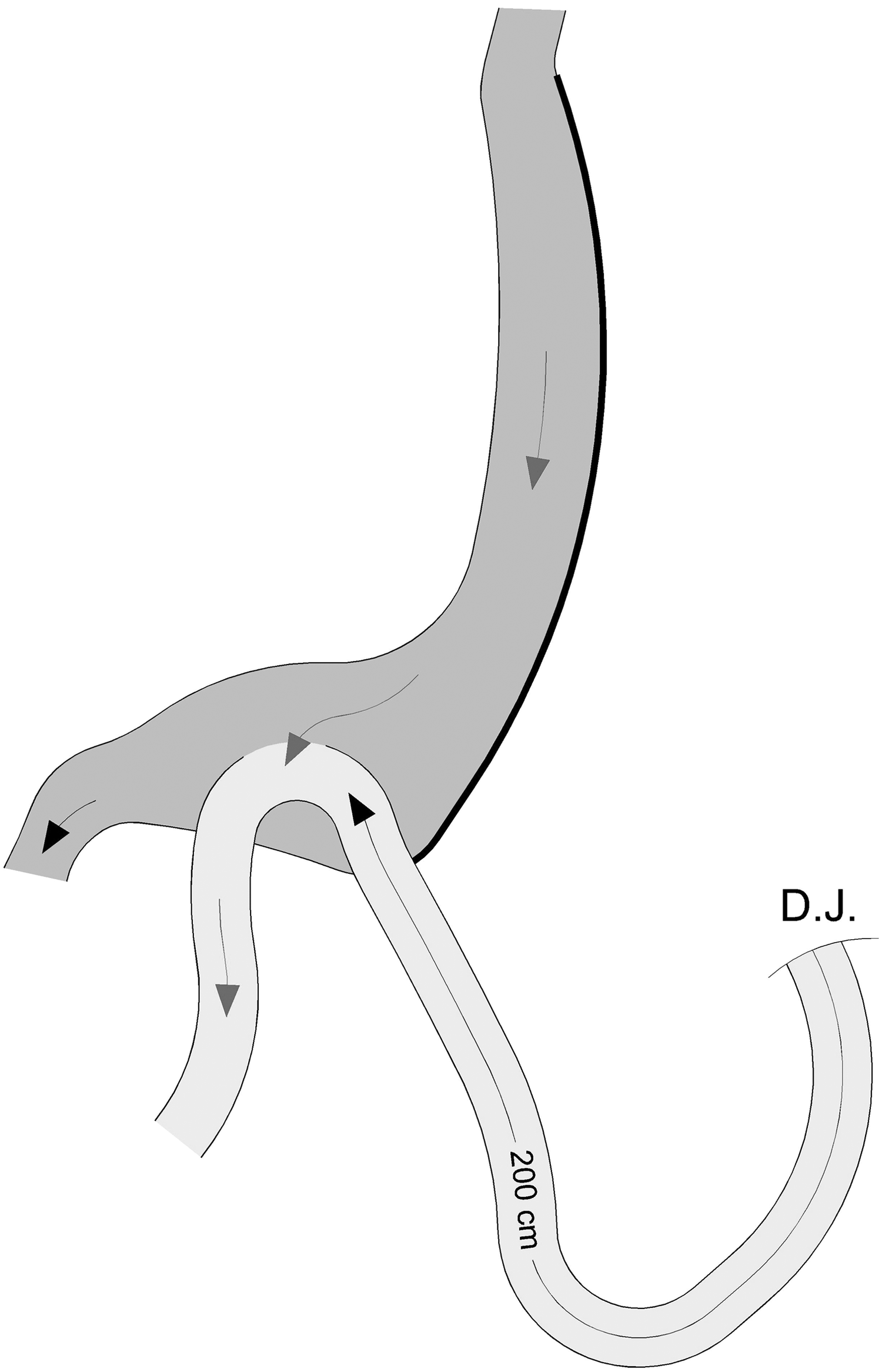
Diagram showing loop gastrojejunostomy between antrum and jejunum 200 cm from Treitz ligament.
Intraoperative view of hybrid technique.
The first portion of the small intestine was mobilized from Treitz ligament and then measured until 200 cm and used to create antecolic, isoperistaltic loop gastrojejunostomy anastomosed to preserved antrum. The procedure was performed by linear stapler of 45 mm in length, with blue cartridge, then closure of enterotomy and gastrostomy with two layers of Vicryl 3/0.
Pressure measurements
All measures were done using a manometer connected to a nasogastric tube and to a normal saline bottle through an IV line set. Certain amounts of saline were instilled with every measurement, based on the gastric volumetric published figures, 9 to reach a state of gastric tumescence, but not overinflation, which may reflect a false high pressure. The manometer zero level was placed at the mid axillary line after saline was instilled and the IV line was disconnected from the saline bottle. All measures were in the supine position. After anesthesia and before any pneumoperitoneum or stomach manipulation, 500 mL saline was instilled in the stomach and the first pressure measurement was recorded. After gastric sleeve creation, 100 mL of saline was instilled into the stomach.
For Hybrid group patients, the second measure was recorded after the anastomosis. For LSG group patients the second measure was recorded after gastric sleeve creation (Fig. 3).
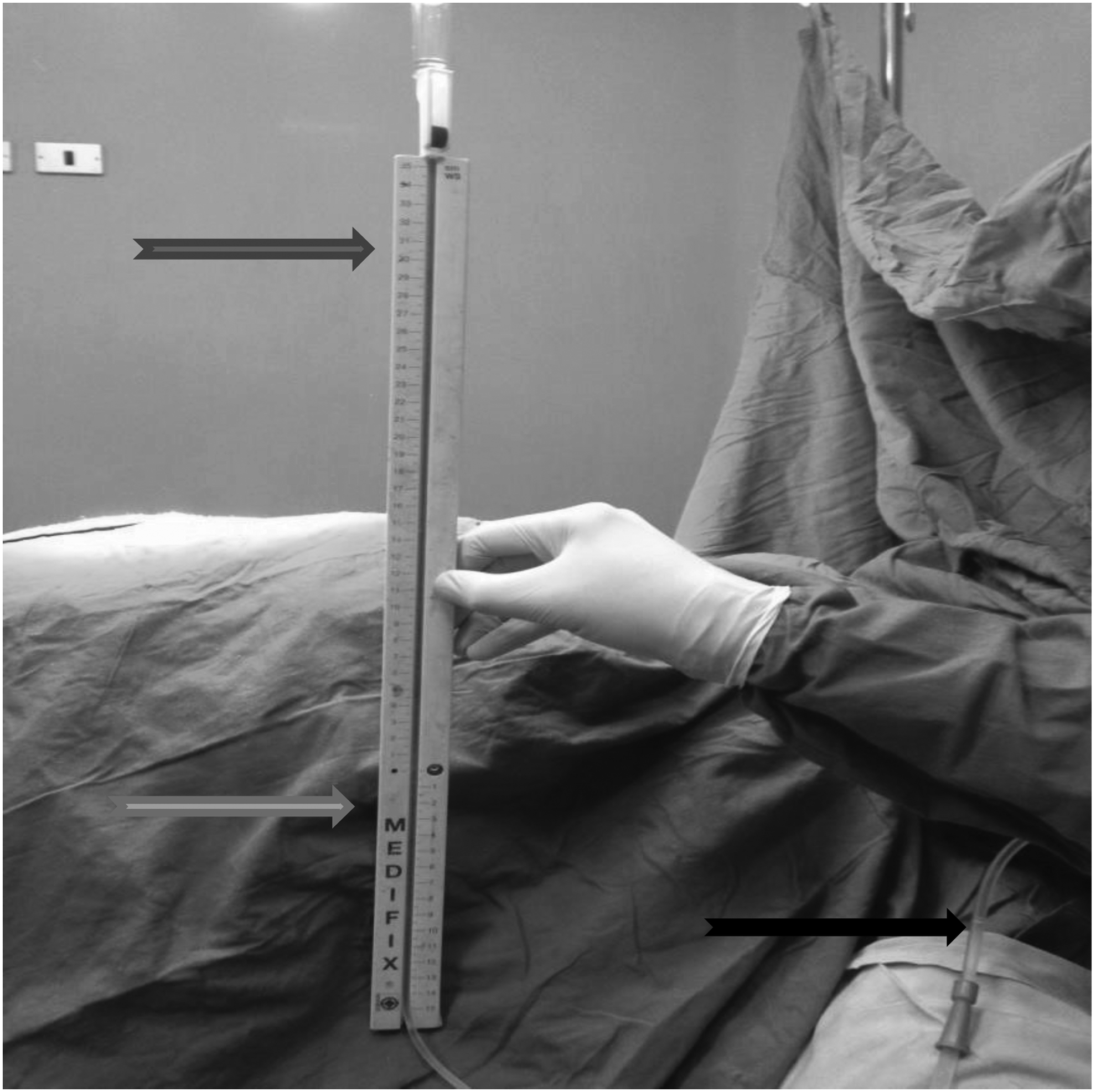
Measuring the gastric pressure using manometer. IV set attached to ruler scale (dark gray arrow), and to a nasogastric tube (black arrow), the zero level at MAL (light gray arrow). MAL, mid axillary line.
Postoperative care
Patients were encouraged to move out of bed few hours after surgery. All patients were given Ampicillin–Sulbactam 3 gm, opioids, proton pump inhibitors, and antiemetics. Gastrografin meal was done to all patients on postoperative day 1 (Fig. 4).

Contrast study of a patient in the hybrid group.
All patients started oral fluids (if tolerated) after confirming that there is no leakage in the study.
Patients were observed for any general (i.e., pulmonary embolism or myocardial infarction) or procedure-related complication after surgery. Special attention was taken to staple line hemorrhage, leaks, and wound infection. The drain was removed before discharging the patients.
The patients were on a liquid diet only for 2 weeks that is then advanced to semisolid diet and mashed food for another 2 weeks. They are then advanced to a regular healthy diet.
Proton pump inhibitors were given for 2 months. Antihypertensive and oral hypoglycemic agents were continued and adjusted by a primary care physician. Patients were given twice daily multivitamins, vitamin D, and calcium supplements.
Follow-up and outcome parameters
All patients were followed up for early postoperative complications (<30 days) like bleeding, leaks, and infections. Patients were reviewed at 1, 3, 6, and 12 months postoperative for %EWL, GERD symptoms using the GERD score questionnaire, 10 and change in state of comorbid conditions. At 3, 6, and 12 months, patients' quality of eating was assessed by Suter Questionnaire 11 (Fig. 5).

Suter Questionnaire. 11
Statistical analyses
Data were coded and entered using the statistical package SPSS (Statistical Package for the Social Sciences) version 23. Data were summarized using mean, standard deviation, median, minimum, and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the nonparametric Mann–Whitney test. For comparing categorical data, chi-square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. Correlations between quantitative variables were done using Spearman correlation coefficient. p-Values less than 0.05 were considered as statistically significant.
Results
Patient demographics
This study was conducted on 40 morbidly obese patients at the Cairo University Teaching Hospital between December 2015 and November 2016. Out of those, 9 patients (22.5%) were males and 31 patients (77.5%) were females. The mean age was 32.3 ± 7.3 years for the hybrid group and 30.65 ± 8.55 years for LSG group. The mean BMI was 50.96 ± 7.6 kg/m2 for the hybrid group and 48.56 ± 6.4 kg/m2 for LSG group (Table 2).
BMI, body mass index.
Out of 20 patients in the hybrid group, 6 (30%) had diabetes mellitus, and 5 (25%) had hypertension, whereas in the LSG group, 5 (25%) had diabetes mellitus, and 6 (30%) had hypertension.
Operative time
The mean operative time was 139.25 ± 8.66 min for hybrid group, 87.05 min for LSG group, significantly (p = <0.001) longer in hybrid group.
Pressure measurements
Intragastric pressure following creation of the sleeve in the LSG group, with a mean of 15.95 ± 1.85 cm H2O, was significantly (p = <0.001) higher than intragastric pressure following anastomosing the sleeve to the jejunum in the hybrid group, with a mean of 10.50 ± 1.43 cm H2O.
Duration of hospital stay
The duration of hospital stay was significantly (p = <0.001) longer for the hybrid group with a mean of 4.05 days, whereas in LSG group was 2.40 days.
Postoperative complications
During the follow-up period, 7 (35%) out of 20 patients in the hybrid group developed complications in the form of port-site hernia, (3) cases that required reoperation, afferent loop syndrome (1) case that was managed conservatively, biliary gastritis (2) cases that resolved conservatively, and dumping (1) case. We had no leakage, bleeding, or mortalities in this group.
While in the LSG group, we had two cases (10%) with bleeding that were successfully managed conservatively. No leakage or mortalities were encountered in this group.
Weight loss
In terms of percentage of excess weight loss (%EWL), the hybrid group achieved higher %EWL than the LSG group at 3 months postoperatively (p = 0.003), 6 months postoperatively (p = 0.027), and 12 months postoperatively (p = 0.009) (Fig. 6).
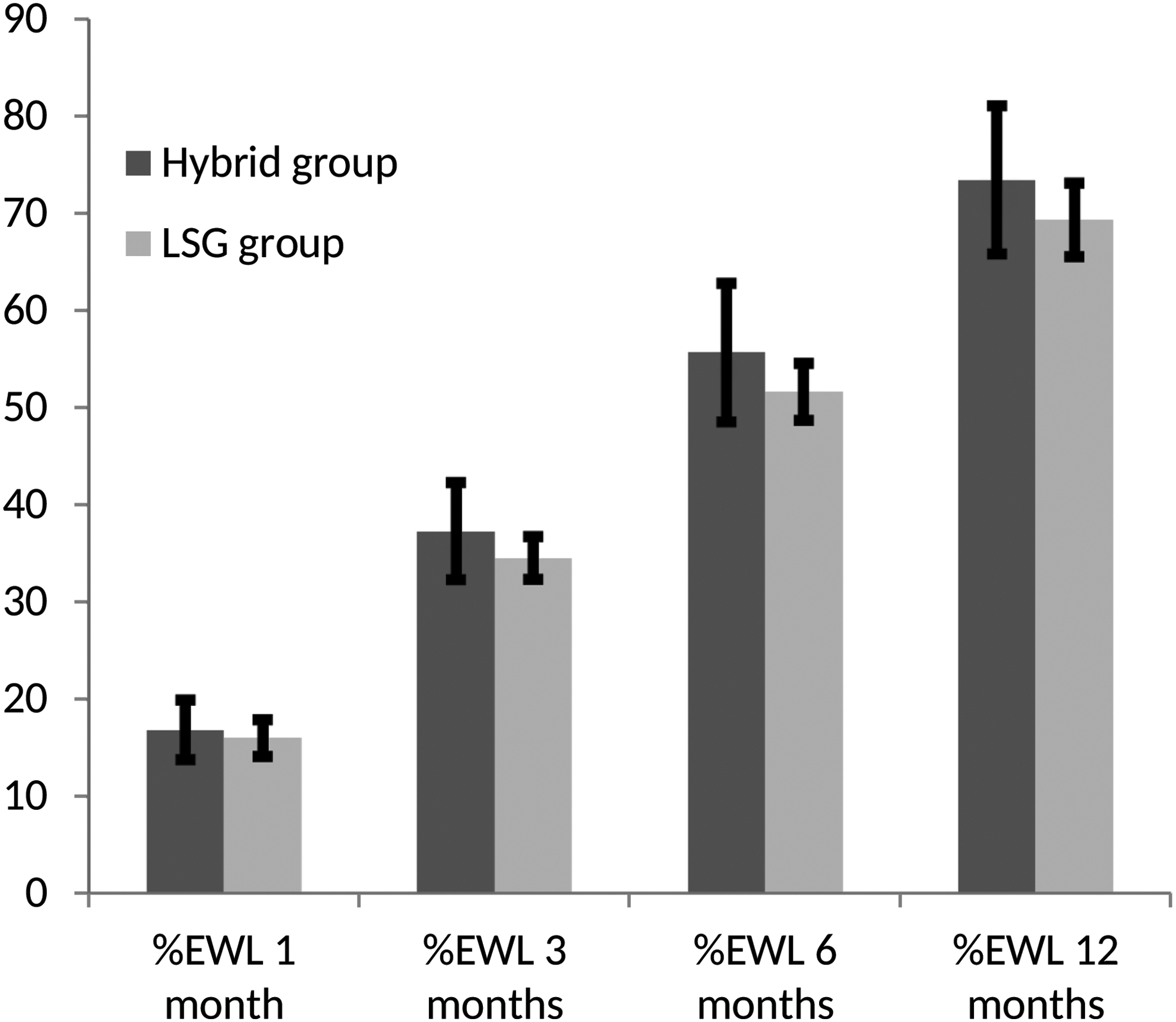
Bar chart comparing %EWL in both groups with error bars.
Among the hybrid group, 5 (25%) patients had preoperative GERD symptoms and 5 (25%) patients had GERD symptoms at 6 months postoperatively. Within the five patients who had GERD symptoms at 6 months postoperatively, 2 (10%) patients did not have GERD symptoms before surgery (new onset), 3 (15%) patients with persistent symptoms, and two patients (10%) had relieved GERD symptoms (Fig. 7).
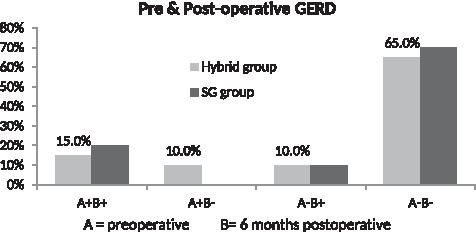
Bar chart showing GERD before and 6 m after surgery in both groups (A+, preoperative GERD; A−, no preoperative GERD; B+, postoperative GERD; B−, no postoperative GERD).
The two new-onset cases were diagnosed as having bile reflux gastritis on upper endoscopy.
Among LSG group, 4 (20%) patients had preoperative GERD symptoms and 6 (30%) patients had GERD symptoms at 6 months postoperatively. Within the six patients who had GERD symptoms 6 months postoperatively, 2 (10%) did not have GERD symptoms before surgery (new onset), and 4 (20%) patients had persistent symptoms (Fig. 7).
During the study period, the hybrid group achieved lower GERD questionnaire scores than the LSG group at 1 month postoperatively (p = 0.234), 3 months postoperatively (p = 0.293), and 12 months postoperatively (p = 0.118).
Food tolerance
There was progressive improvement of food tolerance in both groups during the study as evidenced by increase in Suter's food tolerance score (11); however, the hybrid group achieved higher food tolerance scores than the LSG group at 3 months postoperatively (p = 0.077), 6 months postoperatively (p = 0.169), and 12 months postoperatively (p = 0.068), yet the difference was not statistically significant (Fig. 8). The mean Suter's scores in the hybrid group at 3, 6, and 12 m were 16.5, 19.5, and 22.45, respectively, whereas in the LSG group were 15.40, 18.80, and 21.65.

Bar chart comparing Suter's scores in both groups with Error bars.
Correlation between postoperative intragastric pressure and postoperative GERD score
The GERD score was directly related to postoperative intragastric pressure. The GERD score increased significantly with increase in postoperative intragastric pressure as seen in Table 3.
Correlation between postoperative intragastric pressure and postoperative Suter's score
The Suter's score was inversely related to postoperative intragastric pressure. The Suter's score decreased significantly with increase in postoperative intragastric pressure as seen in Table 4.
Discussion
Laparoscopic sleeve gastrectomy has established itself as a definitive weight loss procedure across the globe. Recently, it has taken over the number one position from the current gold standard Roux-en-Y gastric bypass. 12 This is attributed to relative technical ease of this procedure, excellent efficacy with combination of restrictive and hormonal effects, and minimal anatomic changes and comparable outcome.
While the sleeve gastrectomy is generally a low-morbidity procedure, technical efforts to make the pouch smaller to improve weight loss and reinforcing the staple line to reduce dehiscence may yield an increase in obstructive type side effects and complications. As the pouch volume has decreased, the pouch has become a higher resistance gastric tube and the lower esophageal sphincter (LES) may be anatomically compromised by the disruption of the phrenoesophageal ligament. This may lead to more reflux, dysphagia, and food intolerance. 13
One of the proposed mechanisms of de novo or worsening GERD symptoms after LSG is that converting the large compliant stomach into a long and narrow tube with decreased gastric compliance will cause an increase in intraluminal pressure that correlates inversely with the diameter of the gastric tube and is increased when the pylorus is closed. 9 If this is combined with decrease in LES pressure as demonstrated by Braghetto et al., 13 the result will be an increase in gastroesophageal pressure gradient and GERD.
Hybrid operation emerged based on the idea that by anastomosing the sleeve tube to a jejunal loop, a lower intragastric pressure could be achieved. This could contribute to a decrease in GERD and improvement in food tolerance.
In our study, a manometer was used to measure intragastric pressure and we found that intragastric pressure following creation of the sleeve in the LSG group, with a mean of 15.95 ± 1.85 cm H2O, was significantly (p = <0.001) higher than intragastric pressure following anastomosing the sleeve to the jejunum in the hybrid group, with a mean of 10.50 ± 1.43 cm H2O.
Yehoshua et al. 9 measured and compared the volumes and pressures in the stomach before and after LSG. They found that the sleeve was 10 times less distensible than the resected section. They also found that the remaining sleeve had a greater luminal pressure and smaller volume, yet Yehoshua et al. in their study of the sleeve pressure did not study the correlation between the sleeve pressure and the prevalence of GERD.
We found significant positive correlation between postoperative intragastric pressure and GERD score postoperatively (r = 0.518) (p = 0.001) at 1 month, (r = 0.504) (p = 0.001) at 3 months, (r = 0.388) (p = 0.013), at 6 months, and (r = 0.525) (p = <0.001) 12 months postoperatively.
However, the study failed to demonstrate a significant difference in GERD prevalence between both study groups. At 6 months postoperatively, 5 (25%) patients had GERD symptoms in the hybrid group compared with 6 (30%) patients who had GERD symptoms in the LSG group. This could be attributed to development of biliary gastritis, a complication of the added gastrojejunostomy, in two patients in the hybrid group.
GERD prevalence following sleeve gastrectomy in the literature is a point of debate. In a systematic review of literature by Stenard, 14 worsening of GERD following sleeve gastrectomy was demonstrated by 13 studies that included 5953 patients. There was marked heterogeneity between the studies regarding several factors, including preoperative BMI, method of evaluating GERD, exclusion criteria, length of follow-up, and operative technique. Two studies, Arias et al. 15 and Braghetto et al., 16 excluded patients with GERD preoperatively and reported a 2.1% and 27.5% incidence of GERD after SG, respectively.
Carter et al. 17 presented data for GERD in two categories: early (occurring in the first 30 days), GERD prevalence was increased 14.4% from the preoperative value, and late (occurring after 30 days) was increased by 12.6%. Howard et al. 18 demonstrated a 14% increase with a mean follow-up time of 32 weeks.
Himpens et al. 19 described a triphasic response to GERD, an initial increase at 1 year, followed by a decrease at 3 years, and an increase at 6 years.
The work of Nocca et al. 20 and Lakdawala et al. 21 demonstrated an increase in GERD prevalence after SG of 5.7% and 4%, respectively. DuPree et al., 22 showed persistence of GERD in 84.1% of those who had GERD preoperatively and development of de novo GERD in 8.6%.
While all the previous studies used only clinical evaluation to assess the presence of GERD, other studies used investigation modalities in conjunction with clinical evaluation. Esophageal manometry and 24-h pH monitoring were done in two studies by Gorodner 23 and Burgerhart. 24 Both showed an increase in GERD prevalence of 64% and 43%, respectively.
The study by Sieber et al. 25 used upper GI endoscopy and esophageal manometry in conjunction with clinical evaluation. They demonstrated persistence of GERD in 44.1% and development of de novo GERD in 16%.
However, the opposing effect of sleeve gastrectomy on GERD was demonstrated by several studies in literature as in Stenard's 14 review of literature, in which improvement of GERD following sleeve gastrectomy was demonstrated by 12 studies that included 1863 patients. This improvement was also demonstrated by Daes et al. 26 and Weiner et al., 27 who showed a 20% decrease in GERD prevalence following sleeve gastrectomy. So did Melissas et al., 28 who demonstrated a decrease in GERD after SG at its terminal follow-up (24 months), whereas its 6-month analysis demonstrated a 21.7% increase in prevalence. Other studies showed improvement of pre-existing GERD, but with development of de novo cases as in Chopra et al., 29 Rawlins et al., 30 and Rebecchi et al. 31
We also found significant negative correlation between postoperative intragastric pressure and Suter's food tolerance score postoperatively (r = −0.595) (p = <0.001) at 3 months, (r = −0.568) (p = <0.001) 6 months, and (r = −0.563) (p = <0.001) 12 months postoperatively.
Progressive improvement of food tolerance in both groups was observed during our study as evidenced by increase in Suter's food tolerance score. The study showed that the hybrid group achieved higher food tolerance scores than the LSG group at 3, 6, and 12 months postoperatively, yet the differences were not statistically significant.
The progressive improvement in Suter's food tolerance score postsleeve gastrectomy was demonstrated in other studies.
In the study by Sioka et al., 32 110 patients who underwent LSG were divided into six groups according to the timing point of assessment. Group 1 (<3 months) achieved a mean value of Suter's score of 15.0 ± 5.87, Group 2 (3–6 months) showed marked improvement and in Suter's score with a mean value of 20.3 ± 7.07, whereas Group 3 (6–12 months) achieved the highest score with a mean value of 26.2 ± 1.54.
Schweiger et al. 33 studied the impact of different bariatric procedures on quality of eating and food tolerance. In patients who underwent SG, food tolerance score increased from 16.36 ± 6.6 (at 3–6 months) to 22.27 ± 4.66 (at 6–12 months postoperatively). They also found that laparoscopic adjustable gastric band patients had the significantly lowest total score.
Another study by Overs et al. 34 compared food tolerance ∼2 to 4 years after different bariatric procedures and showed that food tolerance was best after sleeve gastrectomy (median score = 24.0), followed closely by Roux-en-Y gastric bypass (median score = 22.0). The median score of the laparoscopic gastric banding group was significantly lower than all other groups (15.5, p < 0.001).
The hybrid group, as a combined restrictive and malabsorptive procedure, achieved higher %EWL compared with the LSG group. Weight loss achieved after LSG is variable, but most studies report that it is comparable to that achieved by gastric bypass and better than the weight loss achieved following gastric banding. 35
Preservation of antrum in our technique, in contrast to MGB and LRYGB, maintains access to biliary tree through endoscopic retrograde cholangiopancreatography. The indications for accessing the biliary tree postbariatric surgery include sphincter of Oddi dysfunction, common bile duct stones, pancreatic mass evaluation, and treatment of bile leak postcholecystectomy.
This is of particular importance due to increased prevalence of gallstone disease following various bariatric procedures. Asymptomatic gallstones are reported in 26.5% in gastric banding patients, although only 6.8% of patients become symptomatic. 36 In addition, asymptomatic gallstones ranged from 30% to 52.8% after 6 to 12 months postoperatively, whereas symptomatic gallstones occurred by 7–16% in gastric Roux-en-Y bypass patients. 37
Another advantage in our technique, compared with LRYGB, is to avoid the controversy in detecting gastric cancer arising from excluded remnant stomach as RYGB precludes screening for a stomach. Although this risk appears theoretical, this could be of value in countries with high incidence of gastric cancer.
The operative time for the hybrid group was significantly longer than LSG group, but this could be accepted considering the time needed for the added anastomosis and the learning curve required for the new procedure.
The added gastrojejunostomy in the hybrid group not only prolonged the procedure, but also led to the development of related complications. We had one case (5%) of afferent loop syndrome that was managed conservatively as conversion into Roux-en-Y was considered, yet the patient improved dramatically after 3 days after resolving of edema of the efferent loop, two cases (10%) of biliary gastritis that resolved conservatively by diet modification and medical treatment (ursodeoxycholic acid, bile acid sequestrants, and proton pump inhibitors), and one case (5%) of dumping that also improved on conservative measures.
Musella et al., 38 in their series of 974 MGB, reported biliary gastritis as an endoscopic finding in eight patients (0.9%), whereas Kim et al., 39 in their series of 172 MGB, reported a 5% incidence of biliary gastritis.
We suggest that the incidence of biliary gastritis could be lowered by adding one or two suspension sutures between the afferent loop and the gastric sleeve higher than the stoma (Bagua modification). 40
We also suggest that our technique could be an option for revision of failed sleeve gastrectomy; however, this issue needs further evaluation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.