
Abstract
Background:
Bariatric surgery has been considered one of the main interventions for patients with morbid obesity. Body image has been a relevant variable to access the patient's level of satisfaction and weight loss expectations. This systematic review has the aim of verifying the most used measures to evaluate body image of bariatric surgery patients, as well as the main results regarding body image changes after surgery.
Materials and Methods:
This study followed the PRISMA standards, and the search was made on Medline, PsycINFO, and Scopus databases, using “body image” AND “bariatric surgery” as descriptors.
Results:
The Body Shape Questionnaire (BSQ) was the most used instrument. Studies revealed a lack of measures that investigate relevant topics for the bariatric patient, for instance, excess skin. A negative perception of body image was associated with the presence of psychopathology, while the improvement of body image perception was related to a better quality of life after surgery.
Conclusions:
For multidisciplinary teams, it is important to use measures of body image evaluation, both specific and generic, to understand whether aesthetic motivations are such an important aspect of surgery expectations and eventually identify body image distortions that should be treated with psychological counseling.
Introduction
The reduction in quality of life caused by morbid obesity and the difficulty in losing weight through conventional treatments, such as nutritional/pharmacological strategies and physical activity, have made bariatric surgery one of the main interventions for patients with this condition. Several studies have proved the benefits of bariatric surgery for the health of obese people in the medium term and long term, such as lower mortality rates, when compared to obese people who have not received surgical treatment 1 ; greater weight reduction and maintenance of weight loss 2 ; as well as improvement or even resolution of clinical comorbidities related to cardiovascular risk, such as hypertension, diabetes, and hyperlipidemia.3,4
Several clinical indicators, such as 50–75% loss of excess weight, 20–30% loss of initial weight, and a reduction of body mass index (BMI) to <35 kg/m2, 5 have been described in the literature as success criteria for bariatric surgery. Together with objective measures related to weight, the assessment of the patients' psychosocial functioning has been the goal of several studies that aimed to investigate the influence of psychological variables before and after bariatric surgery. Among the measures evaluated in this population, body image has been the subject of particular research interest, seeking to reveal whether rapid weight loss after surgery is accompanied by a positive change in patients' relationships with their own bodies (i.e., an improvement in self-image). Body image, in fact, is one of the topics that healthcare providers should discuss with prebariatric patients to clarify what can be expected after surgery, since massive weight loss has potential negative effects. Issues such as distress caused by loose and hanging skin, concerns about weight and shape that persist even after weight loss, the desire for body-countouring surgeries, among others, must be addressed by the healthcare team to provide the prebariatric patient with an accurate understanding of the treatment outcome. 6
Body image is a complex, multidimensional concept, integrating components related to physical appearance, such as the mental representation of one's own size, shape, and facial characteristics, as well as personal attitudes towards one's own appearance, in which cognition, feelings, and behaviors are implicated. 7 Body image, therefore, refers to a person's perceptions, thoughts, and feelings about his or her body and outward appearance. Dissatisfaction with body image leads to disturbances in the several components that integrate this concept (perceptual, cognitive, affective, and behavioral), since they interact and influence each other. 8
Concerns with body image of the obese were initially described in the late 1960s, but it was only during the 1990s that empirical research about the association between body image and obesity expanded significantly, focusing on the prevalence and nature of body image dissatisfaction in this population. 9 According to Sarwer et al., 9 although some studies report greater body image dissatisfaction in obese women when compared to normal weight women, another set of studies has revealed no association between body image dissatisfaction and BMI in women who are overweight and obese. Such findings, according to these authors, are consistent with body image theories that suggest there is little association between what one thinks about one's own body and the objective reality of one's appearance.
Nevertheless, the same claim cannot be made about people with extreme obesity, especially bariatric surgery candidates, in whom the impairments resulting from excess weight can lead to a greater level of body image dissatisfaction. A study conducted by Libeton et al. 10 revealed that for 32% of bariatric surgery candidates, the main motivation for surgical treatment was related to discontentment with physical appearance and shame in social situations, second only to concerns about health and medical conditions, which were the main motivation for 52% of patients. Thus, we may infer that improvement in the relationship with one's own body is among the expectations that obese people have regarding bariatric surgery outcomes. Considering the psychological health of the patient, it is relevant to evaluate whether such expectations are realistic, that is, if expectations regarding body image can actually be achieved according to well-established clinical criteria.
Also, it would be necessary to discuss body image expectations with the bariatric patient in terms of body functionality, 11 that is, appreciating what the body will be able to do after major weight loss and celebrating functional gains such as mobility and physical capacity, instead of focusing solely on physical appearance. Body functionality is a central component of positive body image, a construct that includes holding favorable views of one's body, accepting the body despite any imperfections, respecting the body by caring for its needs, and engaging in healthy behaviors. 12 Contemporary perspectives on positive body image understand it as a complex and multifaceted construct distinct from low leves of negative body image and extend beyond body satisfaction and appearance evaluation. Current research on body image in obese populations, however, is based mainly on appearance concerns such as body weight and shape (dis)satisfaction, positioning positive and negative body image as opposite ends of the same continuum. 12
Body image assessment among patients who are candidates for and those who have undergone bariatric surgery is relatively recent if compared to most other psychosocial aspects investigated in this population. The terminology used in the literature to refer to this concept varies, with terms such as body image, body dissatisfaction, and body esteem, and several instruments are available to evaluate it. In general, body image assessment measures differ both in perceptual measures, which refer to people's perception about their own body size, leading to a measure of body image distortion (the difference between actual and perceived body size), and in measures related to personal attitudes, which capture the level of one's satisfaction with one's own body, particularly regarding size and weight, identified by the discrepancy between actual and ideal body. 13
Despite the large number of existing instruments to assess body image, most were not developed specifically for obese people, nor validated for this population. Bariatric surgery centers throughout the world have received patients classified as superobese (BMI >50 kg/m2) for treatment. Generally, body image instruments have been developed for college-aged women with normal weight, aiming to evaluate eating disorders. This poses a particular methodological challenge to researchers seeking an adequate body image measure to be used in the context of bariatric surgery, considering that these patients have specific challenges related to weight loss outcomes, which most body image instruments are not able to evaluate more deeply.
Therefore, the general aim of this study was to conduct a systematic review of articles that investigate body image in obese people who are candidates for or have undergone bariatric surgery. As specific objectives, we sought to: (a) verify the adequacy of body image measures in this population, as well as identify the instruments most frequently used for this purpose; and (b) describe and compile results regarding body image changes after bariatric surgery and its relation to other investigated variables.
Methods
This study followed the PRISMA guidelines for systematic reviews. The MEDLINE, PsycINFO, and Scopus databases were searched on June 6, 2016, for articles published from January 1, 2006 through 2016, using the following combination of descriptors: “body image” AND “bariatric surgery.” We chose to search for these descriptors in all fields, according to the instructions provided in each database.
The inclusion criteria for this review were: (a) empirical articles, (b) written in English, Portuguese, or Spanish, which (c) used instruments for body image assessment in obese people who were candidates for or had undergone bariatric surgery, and (d) enrolled only adults (age 18 years and older). Articles using a qualitative method and duplicate records were excluded.
A database of abstracts was created, and the initial evaluation was performed by two independent raters. In case of disagreement between them, a third rater evaluated whether the abstract should be included, following the criteria defined above. Data extraction of the included articles was performed by the first author and discussed with the remaining authors. A flow diagram of study selection, from abstract screening up to final inclusion, is presented in Figure 1, according to the PRISMA statement. 14
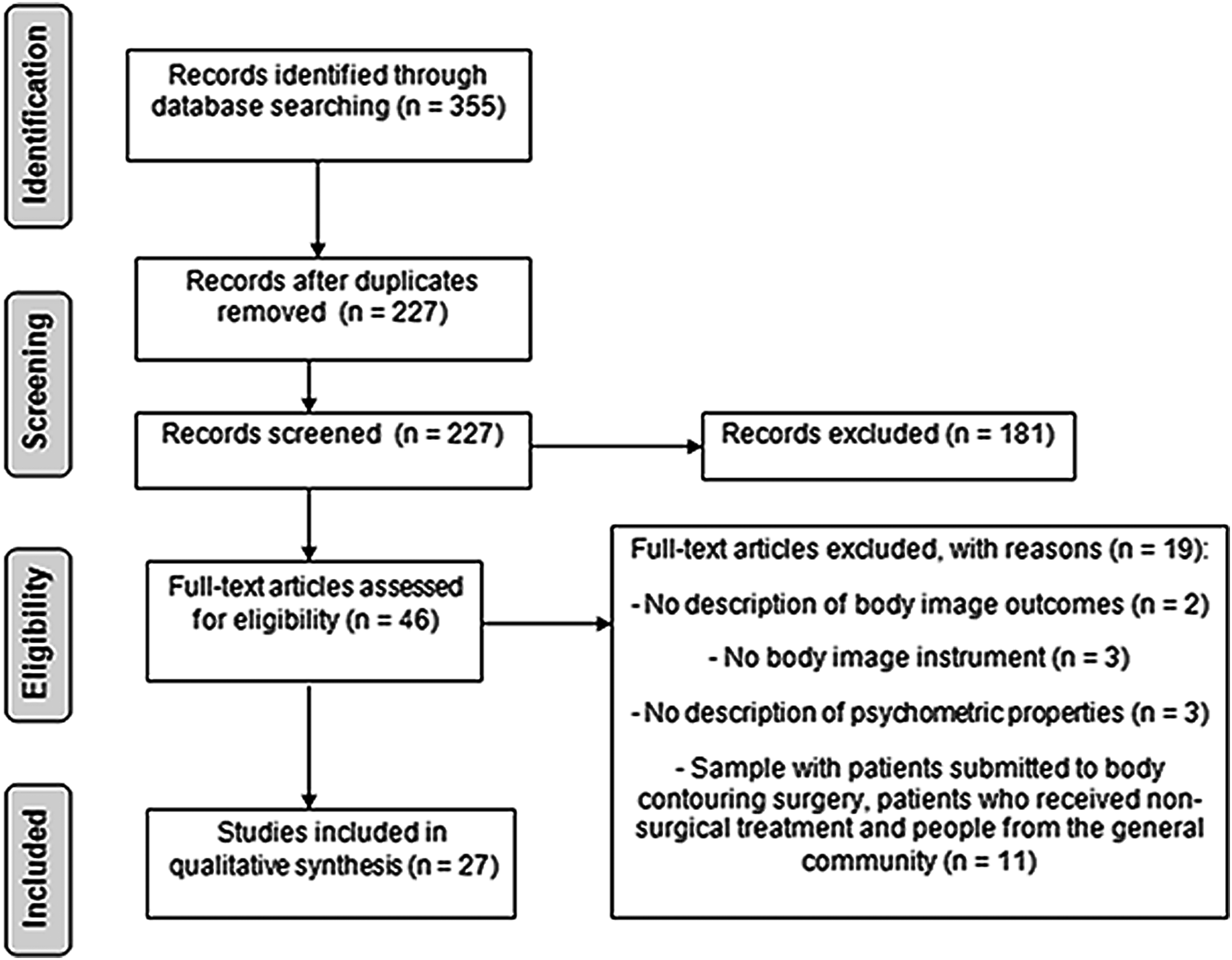
Flow diagram according to the PRISMA statement.
Results
We performed an evaluation of the methodological quality of the 27 included articles, according to the criteria used by García-Llana et al., 15 as shown in Table 1.
Methodological Quality of the Included Articles
Evaluated according to Garcia-Llana et al. 15
Selection and design of the study: (1) Inclusion and exclusion criteria of the participants are indicated. (2) Method of sample selection is specified. (3) Study design is presented. (4) Number of potentially eligible participants and/or initially selected and/or those who accepted and/or participated is reported. (5) If groups are compared, information of item 4 is presented for each group. Definition and evaluation of the studied variables: (6) Variables in the study are clearly defined. (7) Valid or normative instruments are for the main variables. Method and data analysis: (8) Sample sizes are n ≥ 30. (9) Statistical tests used are specified. (10) Participant loss and/or missing data are correctly treated (or at least it is indicated that data quality was reviewed before statistical analysis). Quality of results and discussion: (11) Results are clearly described according to the goals of the study. (12) Discussion presents practical implications of the results and potential benefits for the participants. Evaluation of overall quality: low (1–4 points); medium (5–8 points); high (9–12 points).
NA, not applied.
Also, a table was created with the following information of the included articles: name of first author and year of publication, methodological design of the study, number of participants, mean preoperative BMI of the sample, body image instrument used, other variables of interest, and main results regarding body image, as shown in Table 2.
Studies Included in the Systematic Review
Percent gain in BMI.
Postop 1 and postop 2.
BAT, Body Attitude Test; BEESA, Body Esteem Scale for Adolescents and Adults; BI, body image; BIQLI, Body Image Quality of Life Inventory; BIQ-20, Body Image Questionnaire; BIS, Body Image Scale; BISS, Body Image State Scale; BMI, body mass index; BS, bariatric surgery; BSQ, Body Shape Questionnaire; BUT, Body Uneasiness Test; ED, eating disorders; EDE-Q, Eating Disorder Examination Questionnaire; EWL, excess weight loss; HRQoL, health-related quality of life; NR, not reported; postop, postoperative groups/time points of assessment; preop, preoperative groups/time points of assessment; QoL, quality of life; SA, social anxiety; SD, standard deviation; SexF, sexual functioning; SexP, sexual problems; WRQoL, weight-related quality of life.
Body image measures
The Body Shape Questionnaire (BSQ) was the most common instrument, used in 14 studies, followed by the Body Image Quality of Life Inventory (BIQLI), used in only 3 studies. Four studies used silhouette scales as a body image assessment method, with the main objective of evaluating the level of body image dissatisfaction as well as estimating body size (Table 1).
The BSQ aims to assess concerns regarding body shape, particularly the experience of “feeling fat.” The instrument is composed of 34 questions that are answered on a six-point Likert-type scale (Never, Rarely, Sometimes, Often, Very Often, and Always). Items are derived from interviews with patients diagnosed with eating disorders and women in general. The BSQ has demonstrated adequate psychometric properties; nevertheless, it is clear that its initial purpose was to evaluate the severity of body image concerns in women with anorexia and bulimia. Rosen et al. 16 subsequently conducted a study to test the validity of BSQ in other female and male samples, such as people with specific issues related to body image and obese people receiving treatment for weight loss, and demonstrated it to be a reliable measure.
The BIQLI was the second most widely used instrument, although employed in only three of the included studies.17–19 The BIQLI was designed specifically to evaluate the impact of body image-related experiences on quality of life, that is, to assess the extent to which body image influences aspects of psychosocial functioning such as self-esteem, mood, social relations, eating behavior, and sexuality. 20 There seems to be a trend in the studies of quality of life among bariatric surgery patients to include appearance as a construct of interest. In a systematic review about this issue, Park and Cozza 21 identified 12 instruments used to quantify the impact of appearance changes on patients' quality of life after bariatric surgery, in which body image is included as part of the psychological dimension of quality of life, together with self-esteem, mental health, emotions, and self-efficacy.
Silhouette scales, also known as figure scales, were used as body image assessment measures in four studies in this review.22–25 Such scales consist of a series of frontal views of a human body, ranging from very thin to very obese, and are the most widely used measures to evaluate dissatisfaction with body size. 13 Body dissatisfaction is measured by calculating the discrepancy between actual and ideal body size, as evaluated through the choice of the figure or silhouette that represents these estimates for the patient.
The main advantage of silhouette scales is their ease of administration and the possibility of gathering data collectively. In a review on existing figure scales, however, Gardner and Brown 26 identified several problems related to the application of these instruments, such as the restricted number of figures presented; drawings with unrealistic representations of the human body (e.g., arms and legs of disproportionate sizes); lack of validation and reliability of the majority of scales; presentation of the figures in ascending order, leading to elevated coefficients of reliability; and figures with facial and bodily characteristics representing only a specific ethnic group (generally Caucasian), among other limitations. 26
The Stunkard Silhouette Scale, used in two of the studies included in this review,23,24 consists of nine schematic figures (male and female) from thin to obese. Despite the limitations inherent to the use of figure scales, the Stunkard Scale seems to be very robust and highly correlated with the percentage of overweight and is thus expected to represent a reliable measure of the level of obesity. 27 A study conducted after the construction of the scale estimated the BMI associated with each figure in a sample of Caucasian women and men aged 18–100. This study established normative data that enable the estimation of BMI in cases where there is no access to weight and height data, as well as the empirical evaluation of body image distortion. The authors identified a mean BMI of 18.3 kg/m2 for women, corresponding to the first figure of the scale, and a mean BMI of 45.4 kg/m2 for the last figure; for men, they estimated a mean BMI of 19.8 kg/m2 for the first figure and 41.5 kg/m2 for the last one. 27
Body image changes after bariatric surgery
Regarding body image changes, we found some commonalities among the included studies. Concerns about body image, or a negative evaluation of body image by the patient, were associated with depressive symptoms,28–32 presence of psychiatric symptoms,28,33 greater functional inability due to excess skin, 34 loss of eating control,30,35 and experiences of social discrimination and bullying.36,37 In contrast, improvement in body image evaluation was associated with a decrease in compulsive eating symptoms, 38 reduction of BMI,25,39,40 and percent excess weight loss. 19 Other studies did not find such an association between body image improvement and weight loss.38,41,42
The consensus of the studies included in this review is that the evaluation of body image improves after bariatric surgery17–19,25,29,38,40–45, although this improvement may not occur equally across all evaluated dimensions of body image. 38 One study 45 had the objective of distinguishing two important dimensions of body image, the overevaluation of weight/shape and body image dissatisfaction, and its results suggest that these concepts are related but can be differentiated. Both dimensions improved substantially following surgery; however, while body image dissatisfaction was related to changes in both self-esteem and negative affect, overevaluation of weight/shape appeared to be a more stable marker that was not influenced by fluctuations in negative affect. 45
Some studies evaluated and compared specific groups such as patients with and without social phobia, 39 patients with and without diabetes, 33 and patients with and without a history of sexual abuse and other forms of maltreatment46,47; a comparative analysis did not show differences in body image evaluation between these groups. Nevertheless, the study that aimed to assess gender differences 22 found significantly different results between men and women, with higher levels of dissatisfaction and body image distortion among women. Another group of studies has shown that improvement in sexual functioning is associated with a decrease in body image concerns, revealing a negative correlation between these variables.29,34 Two studies by Sarwer et al.17,18 investigated sexual functioning of men and women and found that while men experienced no significant improvement during the first 4 years after surgery, women reported significant improvement both in sexual functioning and body image as soon as 2 years after surgery.
Discussion and Conclusions
This systematic review showed that body image is a relevant psychosocial variable that has been associated with several important bariatric surgery outcomes. Preoperative body image assessment can estimate the level of patients' dissatisfaction and expectations regarding their new body shape after surgery. We have observed, however, that most body image measures used in the studies do not evaluate specific issues that can be a source of distress for the patient after massive weight loss. Although the instruments have adequate psychometric properties, there is a lack of body image assessment measures that investigate questions pertinent to the reality of the bariatric surgery patient, such as excess skin, body transformations, and acceptance of one's new appearance.
Some recent instruments have been developed specifically for the bariatric population, aiming to evaluate the general perspective about treatment and relevant questions to be addressed after surgery. The Sahlgrenska Excess Skin Questionnaire (SESQ), developed by Biörserud et al., 48 includes 29 questions/statements about the level of daily activities, physical symptoms, mobility limitations, problems in specific body areas due to excess skin, and body image, such as the feeling of not being attractive. The BODY-Q, 49 developed for bariatric patients and those undergoing body-contouring surgery, assesses perceptions regarding the effects of weight loss and/or cosmetic surgery on appearance dimensions (e.g., “My body is not perfect, but I like it,” “I am happy with my body”), quality of life, and experience with healthcare. The benefits of using them together with other generic measures of body image must be recognized, as they can assess items specifically relevant to the bariatric surgery patient. Excess skin, for instance, is a common occurrence that is aesthetically unpleasant for the patient and can seriously damage physical, social, and psychological functioning, negatively impacting body image evaluation after surgery.
Silhouette scales are a useful instrument to evaluate possible distortions of the patient's own perception of body size, as well as expectations of weight loss after surgery. Nevertheless, we have observed that, when silhouette scales are used in samples of candidates for bariatric surgery, the BMIs of patients can surpass the maximum estimated BMI of the last figure of the scale substantially, which can jeopardize the reliability of such results for this population. It is important to develop scales with a larger amplitude of figure sizes (with BMIs >50 kg/m2) for administration to bariatric surgery patients; only then can such scales be assessed to determine whether they provide relevant data on body shape expectations after weight loss.
Price et al. 23 used the Stunkard Scale in female candidates for bariatric surgery and found that expectations related to body shape after surgery corresponded to smaller silhouettes than the silhouette that was clinically expected, overestimating how much weight they will lose and underestimating improvement or resolution of medical comorbidities. Therefore, it is crucial to discuss with the patients presurgically that they do not have to achieve the ideal body shape to experience significant improvements in health status, energy level, and quality of life. 6 Providing to the patient a more clear definition of long-term success regarding weight loss and improvements in health status will help to ensure treatment adherence and maintenance of positive behaviors.
After surgery, body image is part of a broader assessment of the patient's quality of life, in which other variables that are indicative of mental health should be investigated. We found that part of the included studies have associated a negative evaluation of body image with the presence of psychopathology and discriminatory experiences, while body image improvement after surgery was related to a better quality of life as a whole. In contrast, it is important to highlight that there is no consensus in the literature as to whether a direct correlation exists between weight reduction and body image improvement, corroborating theories about the fragile association between the mental representation of one's body and one's actual appearance. The rapid change in body shape achieved with bariatric surgery may not be accompanied by immediate psychological changes related to body image, especially in patients who were obese throughout their lives. The presence of potential mediating variables of body image evaluation after bariatric surgery, such as self-esteem, mood, the influence of sociocultural patterns related to appearance, expectations of weight loss, and social support, should be considered and such variables evaluated.41,42
Another important issue that was observed in the results is the intersection of body image with other relevant components of life after surgery, such as sexual functioning and marital satisfaction, a theme that has not yet been explored in most studies of bariatric patients. Persons with morbid obesity who are deeply dissatisfied with their bodies may be reluctant to undress in front of their partners and thus become very limited during sexual activity. Furthermore, extreme obesity is frequently associated with comorbidities that make sexual activity uncomfortable, difficult, and sometimes impossible. Such studies that evaluate different dimensions of body image in persons who underwent bariatric surgery can enhance research into sexual functioning after weight loss, since these constructs are intrinsically related.
For practicioners and multidisciplinary teams that work directly with patients before and after surgery, it is important to use measures of body image evaluation, both specific and generic, to understand whether aesthetic motivations are such an important aspect of surgery expectations, and eventually identify body image distortions that should be treated with psychological counseling. The occurrence of eating disorders after surgery, for instance, can be related to body image issues such as fear of weight regain leading to a greater vigilance in food intake, which can jeopardize adherence to positive and healthy behaviors in the long term. Identifying those body image issues related to eating disorders, as well as weight regain, through the use of appropriate body image measures is crucial and can detect patients who need specific psychological intervention.
It is important to mention that this systematic review is limited to a period of time, presenting the production of articles published in three languages (English, Portuguese, and Spanish), which comprises only part of the literature relating to this theme. Future studies on body image and bariatric surgery patients should extend beyond appearance evaluation and weight/shape satisfaction and start focusing on contemporary perspectives of positive body image, especially body functionality, a much broader concept that encompasses functions related to physical capacities, bodily senses and perceptions, creative endeavors, communication with others, and self-care. 11 Evaluating the body image of bariatric patient in terms of appreciating what the body will be able to/can do after major weight loss would be helpful to obtain a more complete and comprehensive understanding of body image, focusing not only on appearance but also on body capabilities and functional gains.
Footnotes
Author Disclosure Statement
No competing financial interests exist.