
Abstract
Background:
Previous reports addressing morbidly obese patients grouped body mass indexes (BMIs) within wide ranges, such as >40 or 40–60 kg/m2. We aimed to investigate whether the effects of pneumoperitoneum differ in narrow ranged subgroups of BMI in morbidly obese patients.
Materials and Methods:
Eighteen to 65 year-old, ASA I-II 75 patients were included. The subgroups of BMI were 40 ≤ x < 45, 45 ≤ x < 50, and ≥50 kg/m2. Plato pressure (Pp), peak inspiratory pressure, and etCO2 were recorded beside vital parameters. Dynamic compliances (Cdyn = Vt/PIP-PEEP) were calculated. Arterial blood gases were obtained before pneumoperitoneum (t1), at the end of pneumoperitoneum before desufflation (t2), and after desufflation (t3).
Results:
Pneumoperitoneum caused similar alterations in hemodynamic parameters and respiratory mechanics in Group I (n = 24), II (n = 28) and III (n = 23). Pp at t1 and t2 was significantly higher in Group II and III (p < 0.017). Cdyn were significantly lower at t1 and t2 in Group III (p < 0.01). The number of patients who required adjustments during pneumoperitoneum was significantly higher in Group III (p < 0.01).
Conclusion:
The Cdyn and airway pressures in laparoscopic bariatric surgery revealed statistically significant difference between BMI ≥50 kg/m2 and BMI of 40 ≤ x < 45 kg/m2. We suggest that BMIs of 40 ≤ x < 45 and ≥50 kg/m2 should not be described in one group, but grouped separately in future studies addressing respiratory mechanics.
Introduction
Morbidly obese patients are known to develop physiologic changes pertaining to both hemodynamic and respiratory functions. Atelectasis was reported to develop immediately after anesthetic induction increasing the shunt, which impairs gas exchange leading to hypoxemia. Morbid obesity results in several pathophysiologic changes of respiratory system mechanics, tending toward development of intraoperative atelectasis, and exaggerates the impairment of gas exchange. Hence, oxygenation is expected to be inversely related to body mass index (BMI). 1
As laparoscopic bariatric surgery has rapidly gained acceptance, morbidly obese patients were investigated for the effects of pneumoperitoneum on those parameters, as they have already been physiologically altered in these patients. During pneumoperitoneum, hemodynamic and respiratory mechanics were reported to have changed significantly, whereas pulmonary gas exchange and PaO2 were reported not to have changed.2–6
Morbid obesity is described as BMI ≥40 kg/m2 or BMI ≥35 kg/m2 associated with obesity-related co-morbidity. Morbid obesity is more precisely defined as BMI between 40 and 60 kg/m2, whereas BMI ≥60 kg/m2 is defined as super obesity. 7 Previous reports most commonly enrolled morbidly obese patients in one study group, to reflect a wide range of BMI, such as >40 or 40–60 kg/m2. The primary objective of this study was to determine whether the alterations in hemodynamic and respiratory parameters during laparoscopic bariatric surgery differ in relation to the level of BMI in morbidly obese patients by subgrouping them into narrow ranges of BMI.
Materials and Methods
This observational study was approved by Institutional Ethical Committee (GO 14/170–26). Informed consent was obtained from the patients, whose data were to be recorded and analyzed for the study. Eighteen to 65 year-old, ASA I-II patients undergoing laparoscopic bariatric surgery between May and October 2014 were enrolled. Patients with history of surgery comprising diaphragm and lungs, hepatorenal disease, pathology in chest x-ray, lung disease, and electrolyte disorders, and patients who did not approve their data to be used for this study, were not included. Patients whose anesthetic management required alterations due to unanticipated difficult airway or switching to open surgery were excluded from the study.
The patients were assessed preoperatively and were given premedication for both aspiration and thromboembolic event prophylaxis. On arrival to the operating room, they were monitored for electrocardiogram, noninvasive blood pressure, and peripheral oxygen saturation (SpO2). After 3 min of preoxygenation, anesthesia was induced when the patients were in 15° head-up position. Anesthetic induction and maintenance were similar in all patients. Anesthetic induction was provided by propofol 2 mg/kg (ideal body weight [IBW]) and fentanyl 1–2 mcg/kg (IBW). Rocuronium 0.6 mg/kg (IBW) was used for neuromuscular blockade. After anesthetic induction, radial artery was catheterized for invasive arterial blood pressure monitoring. Anesthesia was maintained by sevoflurane in O2/air and 0.5 mcg/kg/min remifentanil infusion.
Ventilation was provided by volume control (VC) mode; tidal volume (TV): 8–10 mL/kg (IBW); and positive end-expiratory pressure (PEEP): 5–7 cmH2O. Ventilatory adjustments according to etCO2 and peak inspiratory pressure (PIP) alterations were at the attending anesthetist's initiative; all the adjustments were recorded as well.
At 5-min intervals, heart rate (HR), systolic blood pressure, diastolic blood pressure, mean arterial blood pressure (MAP), SpO2, TV, respiratory rate, PEEP, plato pressure (Pp), PIP, and etCO2 were recorded. Dynamic compliances (Cdyn = Vt/PIP-PEEP) were calculated. Duration of pneumoperitoneum and intra-abdominal pressures during pneumoperitoneum were recorded, as well. Arterial blood gases were obtained before pneumoperitoneum (t1) (supine position), at the end of pneumoperitoneum before desufflation (t2) (reverse Trendelenburg position), and after desufflation (t3) (supine position).
These parameters were compared among three different BMI subgroups, which were determined as 40 ≤ x < 45, 45 ≤ x < 50, and ≥50 kg/m2.
Statistical analysis
Data analysis was performed by using SPSS for Windows, version 11.5 (SPSS, Inc., Chicago, IL). The distribution of continuous variables was determined to be normal or not by Kolmogorov-Smirnov test. Homogeneity of variances was evaluated by Levene's test. Data were shown as mean ± standard deviation or median (interquartile range), where applicable. The means were compared by one-way analysis of variance (ANOVA) and medians by Kruskal-Wallis test. When one-way ANOVA or Kruskal-Wallis test statistics showed significant p-value, post hoc Tukey honest significant difference or Conover's multiple comparison test was used to determine which group was different from others.
The repeated measurements were analyzed by ANOVA and Friedman test. When the repeated measurements of ANOVA or Friedman test showed statistically significant p-value, Bonferroni adjusted multiple comparison test or Wilcoxon sign rank test was used to determine which measurement time was different from others. Categorical data were analyzed by Pearson's chi-square or likelihood ratio test. Degrees of association between continuous variables were evaluated by Spearman's rank correlation analyses. A p-value <0.05 was considered significant. For all possible multiple comparisons, the Bonferroni correction was applied for controlling type I error.
Results
Eighty patients were observed in the study period. Five patients were excluded; three of these patients had unanticipated difficult intubation and two patients' surgeries were switched to open surgery. Seventy-five patients were classified into three groups according to their BMIs. Group I, II, and III were defined as 40 ≤ x < 45 kg/m2 (n = 24), 45 ≤ x < 50 kg/m2 (n = 28), and ≥50 kg/m2 (n = 23), respectively. The groups were similar in terms of age and gender. The types of laparoscopic bariatric surgery were sleeve gastrectomy and minigastric bypass. In Group III (BMI ≥50 kg/m2), minigastric bypass was the type of surgery to be preferred, which led to longer periods of pneumoperitoneum (Table 1).
Demographical Data of the Patients and the Surgery Types with the Durations of Pneumoperitoneum
The difference between Group I and III was found to be statistically significant (p < 0.01).
The difference between Group II and III was found to be statistically significant (p < 0.01).
BMI, body mass index.
The HR and MAPs were similar in all groups. Also, pneumoperitoneum did not result in alterations in hemodynamic parameters in any of the three groups. SpO2 was also similar in all groups (within a range of 96–98%) and pneumoperitoneum did not result in any alterations in any of the groups.
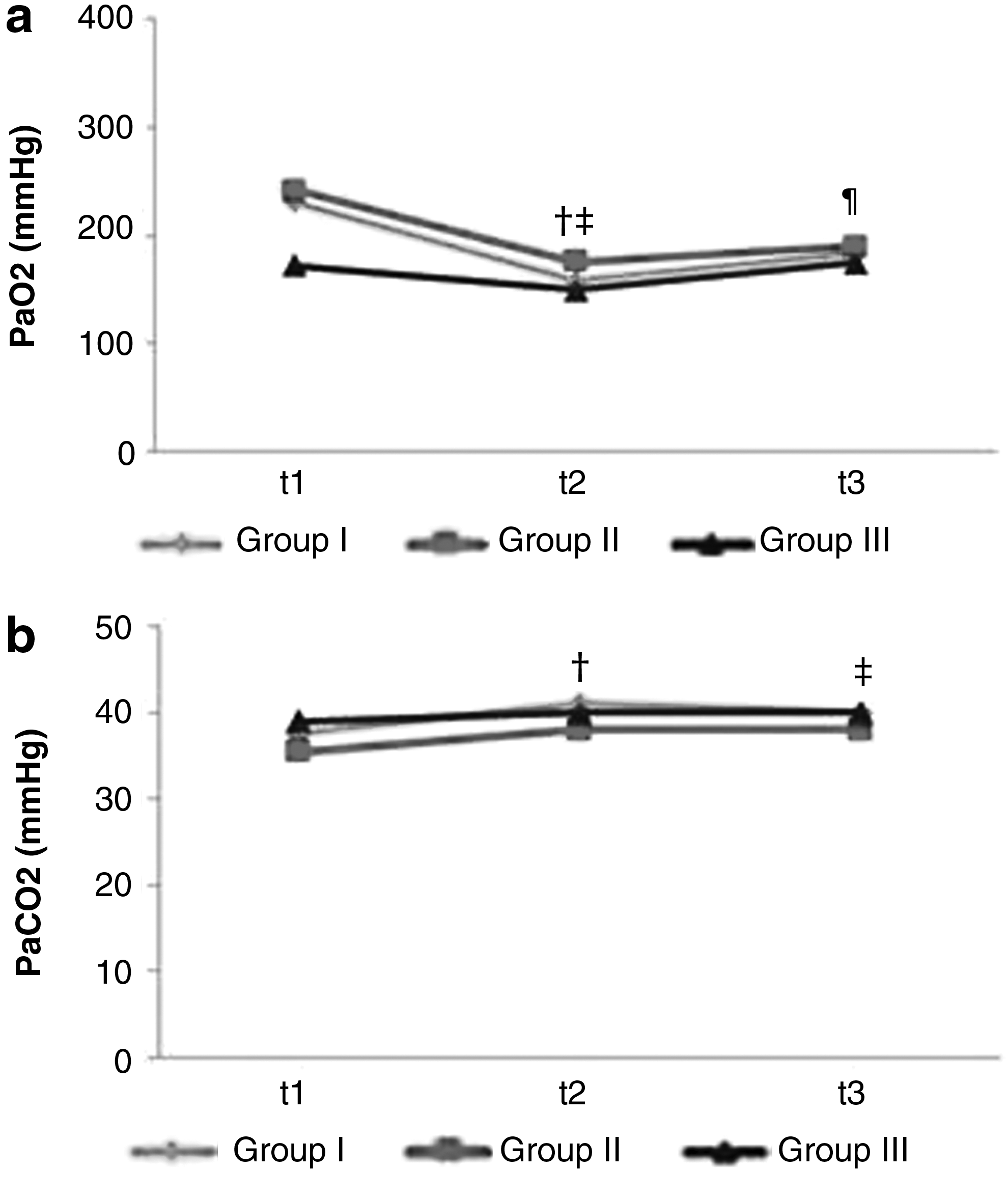
PaO2 at t1, t2, and t3 was similar in all groups. Despite statistical insignificance, the PaO2 at t1 in Group III revealed clinically significant lower measure, compared to Groups I and II. The decrease in PaO2 at t2 was significant in Groups I and II (Table 2 and Fig. 1a).
The Arterial Blood Gas Analysis and etCO2 Levels at Three Predetermined Times
The difference between t1 and t2 was found to be statistically significant (p < 0.01).
The difference between t1 and t3 was found to be statistically significant (p = 0.013).
The difference between t1 and t2 was found to be statistically significant (p = 0.003).
The difference between t1 and t3 was found to be statistically significant (p = 0.003).
The difference between t1 and t2 was found to be statistically significant (p < 0.0056).
The difference between t1 and t3 was found to be statistically significant (p < 0.0056).
At t1, PaCO2 values were higher in Group III. Pneumoperitoneum significantly increased PaCO2 in Group I; t2 and t3 were significantly higher than t1. The PaCO2 alterations during pneumoperitoneum were similar in Groups II and III (Table 2 and Fig. 1b).
PEEP, PIP, and Pp were recorded at 5-min intervals throughout the operation, as well as during the period of pneumoperitoneum. The measures at t1 were obtained before pneumoperitoneum and the measures at t3 were obtained after desufflation. The measures at t2 were presented as the mean value of the measures that were recorded at 5-min intervals during pneumoperitoneum. Since these parameters did not show any difference throughout pneumoperitoneum, mean values were obtained for statistical analysis and Cdyn of t2 were calculated according to these mean values.
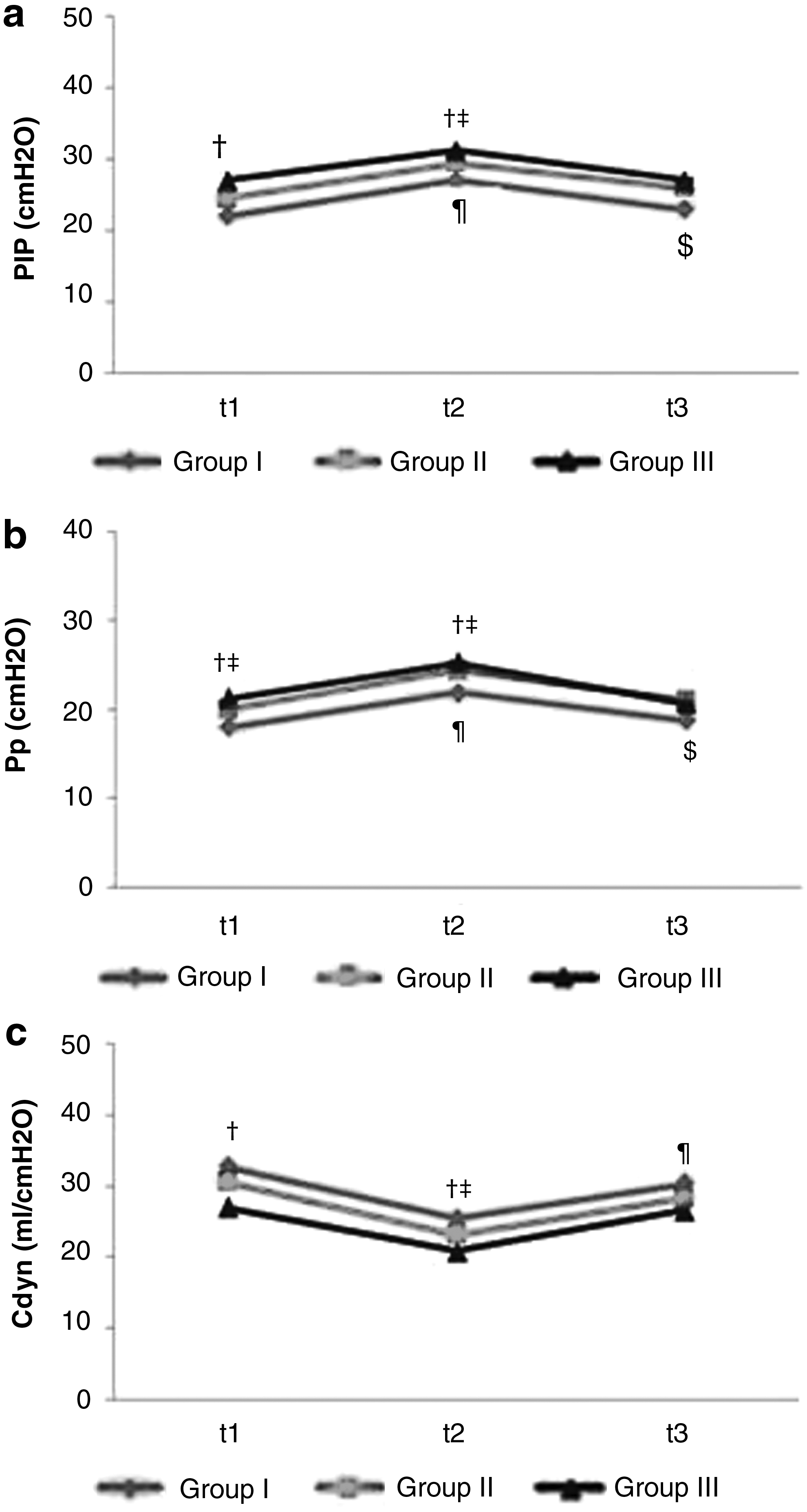
The PIP at t1 was significantly lower in Group I, compared to Group III. At t2, PIP in Group I was significantly lower than Groups II and III. At t3, the PIP was similar in all groups. The PIP alterations during pneumoperitoneum were similar in all groups. The PIP increased significantly during pneumoperitoneum in all groups (Table 3 and Fig. 2a).
Peak Inspiratory Pressure, Plato Pressure, and Dynamic Compliances at Predetermined Periods
The difference between Group I and Group III was found to be statistically significant (p < 0.017).
The difference between Group I and Group II was found to be statistically significant (p < 0.001).
The difference between Group I and Group III was found to be statistically significant (p < 0.01).
The difference between t1 and t2 was found to be statistically significant (p < 0.0056).
The difference between t2 and t3 was found to be statistically significant (p < 0.001).
The difference between t1 and t2 was found to be statistically significant (p < 0.01).
The difference between t1 and t2 was found to be statistically significant (p = 0.003).
Cdyn, dynamic compliance; PIP, peak inspiratory pressure; Pp, plato pressure.
The Pp at t1 and t2 were significantly lower in Group I compared to Groups II and III. In all groups, the Pp significantly increased at t2 compared to t1 and decreased at t3 compared to t2. At t3, Pp was similar in all groups. The alterations during pneumoperitoneum were similar in all groups (Table 3 and Fig. 2b).
The Cdyn were significantly lower at t1 and t2 in Group III, compared to Group I. In all groups, the Cdyn altered significantly at t2 and t3 compared to t1 and t2, respectively. The alterations were similar in all groups (Table 3 and Fig. 2c).
Ventilator adjustments were required due to CO2 load or the excessive rise in PIP during pneumoperitoneum. The number of patients who required adjustments during pneumoperitoneum was significantly higher in Group III compared to Group I (Table 4).
The Number of Patients who Required Ventilatory Adjustments During Pneumoperitoneum
The difference between Group I and Group III was found to be statistically significant (p = 0.004).
There was no correlation between hemodynamic and respiratory parameters with the duration of pneumoperitoneum.
Discussion
In our study, we observed that pneumoperitoneum altered the respiratory mechanics similarly in morbidly obese patients with BMI of 40 ≤ x < 45, of 45 ≤ x < 50, and ≥50 kg/m2. Pneumoperitoneum caused a significant decrease in PaO2 in patients with BMI of 40 ≤ x < 45 and 45 ≤ x < 50 kg/m2. The respiratory mechanics, including Cdyn, PIP, and Pp, were significantly different before and during pneumoperitoneum in patients with BMI of 40 ≤ x < 45 kg/m2 compared to patients with BMI ≥50 kg/m2.
In previous studies addressing morbidly obese patients in terms of respiratory and hemodynamic parameters during laparoscopic or open surgery, the patients with BMI of 40–60 kg/m2 were enrolled as one group, and in many studies, the patients with BMI ≥60 kg/m2 were included in that same group as well.3–5,8
However, in Salihoglu et al.'s study, the morbidly obese patients were enrolled in two groups with respect to their BMIs: <50 and ≥50 kg/m2. It was reported that PIP significantly increased and Cdyn significantly decreased with pneumoperitoneum. The rate of rise in PIP was similar, but the rate of decrease in Cdyn was reported to be higher in patients with BMI ≥50 kg/m2. The reduction in Cdyn with pneumoperitoneum was reported as 22.91% and 28.26% compared to that after anesthetic induction in patients with BMI <50 and ≥50 kg/m2, respectively. 3
Our study demonstrated that the rate of decrease in Cdyn was 22% in patients with BMI of 40 ≤ x < 45 and BMI ≥50 kg/m2; and 24% in patients with BMI of 45 ≤ x < 50 kg/m2. Pneumoperitoneum resulted in a similar decrease in our patients; however, the Cdyn revealed a significant difference between patients with BMI of 40 ≤ x < 45 kg/m2 and BMI ≥50 kg/m2 before pneumoperitoneum and during pneumoperitoneum. In Salihoglu et al.'s study, the Cdyn of patients with BMI <50 kg/m2 were reported to be 48 ± 12, 38 ± 11, 37 ± 12, and 40 ± 15 mL/cmH2O at predetermined periods of 10 min after anesthesia induction, 10 min after pneumoperitoneum, 10 min after terminating pneumoperitoneum, and immediately before extubation, respectively. Also, in patients with BMI ≥50 kg/m2, the Cdyn were reported as 46 ± 17, 35 ± 13, 33 ± 13, and 37 ± 15 mL/cmH2O at those predetermined times. 3
The Cdyn in our study were lower compared with Salihoglu et al.'s study, in which the TVs were calculated as 10 mL/kg according to corrected body weight. This calculation actually resulted in higher TV than those calculated according to IBW. We applied TV 8–10 mL/kg according to IBW, which may have resulted in lower Cdyn in our study. The rate of rise in PIP in Salihoglu et al.'s study was higher than in our study, which could have resulted due to higher TV as well.
In Demiroluk et al.'s study, respiratory mechanics and oxygenation were reported to be similar during both open and laparoscopic surgeries in morbidly obese patients with BMI of 43–65 kg/m2. In laparoscopic surgery group, Cdyn were reported as 55 ± 14 mL/cmH2O after anesthetic induction, 34 ± 8 mL/cmH2O after pneumoperitoneum, 36 ± 8 mL/cmH2O after gastric band placement, and 49 ± 10 mL/cmH2O after desufflation. 5 The Cdyn were higher compared with our patients. The TV (10 mL/kg) they applied was higher than ours and was kept constant throughout the operation; hence, the Cdyn might have been resulted in higher measures. The authors reported a 38% decrease in Cdyn with pneumoperitoneum. It was previously reported that pneumoperitoneum decreased Cdyn by 35% in morbidly obese patients. 9 In a similar study, addressing morbidly obese patients with BMI of 40.9–66.8 kg/m2 reported a decrease in Cdyn by ∼28% with pneumoperitoneum. 8
Another study, addressing morbidly obese patients with BMI of 40–60 kg/m2 in terms of respiratory mechanics during open and laparoscopic gastric bypass, reported 42% decrease in Cdyn during laparoscopic surgery. 2 In our study, we observed that Cdyn decreased by 22% with pneumoperitoneum irrespective of BMI levels. The Cdyn were low in all groups. Although the alterations with pneumoperitoneum were similar, the Cdyn before and during pneumoperitoneum were significantly lower in patients with BMI ≥50 kg/m2 compared to patients with BMI of 40 ≤ x < 45 kg/m2.
In Nguyen and Wolfe's study, comparing the effects of open and laparoscopic surgery to establish the effects of pneumoperitoneum, compliances significantly decreased and PIP and PaCO2 significantly increased in laparoscopic surgery group. PIP levels increased from 29.7 ± 5.3 cmH2O at baseline to 33.8 ± 4.5 cmH2O 2 h after insufflation. EtCO2 levels increased from 34.9 ± 4.7 mmHg at baseline to 40.0 ± 4.6 mmHg 2 h after insufflation. 2 The rises were reported to be significant, which were also significant in our study. However, the actual measures were lower in our study, which may have been the result of shorter durations of pneumoperitoneum in our patients.
In Demiroluk et al.'s study, the PIP was reported to increase by 20–22% with pneumoperitoneum; similar to that, we also observed that PIP increased by 20% with pneumoperitoneum. 5 Despite lower levels of Cdyn, PIP, and Pp in our study, we maintained these parameters within normal ranges (PIP <35 cmH2O and Pp <30 cmH2O) by ventilator adjustments as needed during pneumoperitoneum. The number of patients who required ventilator adjustments during pneumoperitoneum was significantly higher among the patients with BMI ≥50 kg/m2. This may also reveal that this group of patients was significantly affected by pneumoperitoneum, while the ventilator adjustments provide safe and effective period of pneumoperitoneum.
In Nguyen and Wolfe's study, PaO2 was reported not to have altered significantly and pulmonary gas exchange was reported to be similar in two different surgical techniques. It was suggested that in morbidly obese patients, laparoscopic surgery is generally well tolerated if the level of hypercapnia is maintained within normal ranges by ventilator adjustments during surgery. 2 In our study, the number of patients requiring certain ventilator adjustments increased as the BMI increased. PaCO2 was maintained within normal range, provided the patients tolerate surgery despite different levels of BMIs. In our study, all the respiratory mechanics after desufflation returned to similar levels compared with before insufflation groups.
In Demiroluk et al.'s study, PaO2 values were 180 ± 51 mmHg, 175 ± 43 mmHg, 170 ± 40 mmHg, and 170 ± 45 mmHg, after anesthetic induction, after pneumoperitoneum, after gastric band placement, and after desufflation, respectively. 5 The BMI within such wide range may have resulted in such lower measures. In our study, the PaO2 before pneumoperitoneum was higher in patients with BMI of 40 ≤ x < 45 and 45 ≤ x < 50 kg/m2, whereas, despite statistical insignificance, it was lower in patients with BMI ≥50 kg/m2. The subgrouping of morbidly obese patients according to their BMIs may prevent overlooking such difference. Since PaO2 was already lower before pneumoperitoneum in BMI ≥50 kg/m2, pneumoperitoneum did not seem to affect this parameter in those patients. This result may have been due to higher intra-abdominal pressures of morbidly obese patients. This higher intra-abdominal pressure may provide sufficient pressure for laparoscopic surgery with lower volume of CO2 insufflation. The insufflation of a lower volume may prevent further worsening of oxygenation in those patients.
We recorded intra-abdominal pressures during pneumoperitoneum, but we did not have a record of basal measure and also the volume of CO2 insufflated. Hence, it is not possible to make any suggestion on the definitive cause, but pneumoperitoneum decreases PaO2 significantly in patients with BMI of 40 ≤ x < 45 and 45 ≤ x < 50 kg/m2.
As previously reported, the morbidly obese patients mostly tolerate laparoscopic surgery, provided the respiratory parameters are maintained within acceptable limits. Besides certain adjustments in ventilator settings, the compensatory effect of reverse Trendelenburg position leading to a rise in functional residual capacity was also suggested to be a beneficial contributing factor for this tolerance.5,8 Permissive respiratory acidosis and hypercapnia were suggested to be beneficial as well. 8
Limitations
In our study, we aimed to compare the effects of pneumoperitoneum in morbidly obese patients with different BMI levels and we performed our observational study in patients undergoing bariatric surgery. Thus, we did not have patients with lower BMI. The effect of pneumoperitoneum to be investigated in patients with lower BMI levels would have required different surgical procedures other than bariatric surgeries. In future studies, a group of patients with lower BMI may be considered to be included, but it was not one of our aims in this study.
In our patients, we preferred VC ventilation (VCV) with TV: 8–10 mL/kg (IBW), frequency: 12–14 bpm, and PEEP: 5–7 cmH2O as the standard ventilation technique. There are several studies addressing various ventilation strategies in morbidly obese patients. 10 VCV and pressure control ventilation were reported to be similar; none of them was found to be superior.
When the use of PEEP alone or PEEP with recruitment maneuver (RM) were compared, PEEP with RM was found to improve PaO2/FiO2 ratio and increase the compliance compared to PEEP alone. 11 Similarly, Futier et al. also found that PEEP with RM was more effective in improving pulmonary gas exchange than the use of PEEP alone. 12 PEEP with RM was reported to prevent atelectasis and beneficial within the first 30–40 min of the operation. 13 On the other hand, the use of RM is still contradictory, due to the development of barotrauma and association with more postoperative complications. 14 In our study, RM may have resulted in higher compliances; however, we preferred VCV with PEEP, without employing any RM.
We did not record the angles of the operating table during the operation, which may have an influence on the respiratory mechanics. However, operations were performed by the same surgical team with the same surgical approach. On the other hand, the type of surgery of patients with BMI ≥50 kg/m2 was different, which may also have influence on respiratory mechanics. However, the indication for a certain type of procedure is different in patients with different levels of BMIs, so it may not be possible to compare patients with different BMIs undergoing the same type of operation. This can only be possible by enlarging the sample size to include patients with different levels of BMIs undergoing the same type of operation.
The intra-abdominal pressures during pneumoperitoneum were recorded and found to be similar in all groups. However, we did not record the opening intra-abdominal pressures or the sufficient insufflation volume required for the surgery, which may both have influence on respiratory mechanics. The intra-abdominal pressures of morbidly obese patients were reported to be higher compared with patients with normal BMI (2). In future studies, the opening pressures and the sufficient insufflation volume should also be considered to investigate whether there is also a difference between subgroups of morbidly obese patients.
Conclusion
In our study, we observed that pneumoperitoneum caused similar changes in subgroups of morbidly obese (BMI of 40 ≤ x < 45, 45 ≤ x < 50, and ≥50 kg/m2) patients. The Cdyn and airway pressures in laparoscopic bariatric surgery revealed a clinically relevant difference as the BMIs rise. This difference was statistically significant in patients with BMI ≥50 kg/m2, compared to patients with BMIs of 40–45 kg/m2. We suggest that BMIs of 40 ≤ x < 45 and ≥50 kg/m2 should not be described in one group, but grouped separately in future studies addressing respiratory mechanics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.