
Abstract
Background:
Bariatric surgery has superior therapeutic outcomes compared with other existing treatments. Our aim was to evaluate the safety and efficacy of laparoscopic sleeve gastrectomy (SG) in adolescents with obesity.
Methods:
From February 2012 until March 2018, all adolescents who underwent SG for obesity were analyzed. Demographics were evaluated. The main outcomes measured were change in weight, body mass index (BMI), percentage excess weight loss (%EWL), complications, and reoperations.
Results:
Twenty-two adolescents (16/6, F/M) underwent SG. Mean age, preoperative weight, and BMI were 16.4 ± 2.1 years, 125.0 ± 30.2 kg, and 45.1 ± 8.1 kg/m2, respectively. The mean duration of operation and hospital stay were 54.7 ± 3.9 min and 2 ± 0 days, respectively. The median follow-up was 9 months. The mean weight loss, BMI loss, and %EWL were 36.4 ± 31.8 kg, 13.8 ± 10.5 kg/m2, and 50.9% ± 27.1%, respectively. One patient developed transient vitamin deficiency due to repeated vomiting. Two patients with type 2 diabetes mellitus had complete remission without medications.
Conclusions:
SG is effective and safe to treat obesity in adolescents. Further studies are needed to evaluate the long-term effects of SG in adolescents.
Introduction
Adolescent obesity prevalence is increasing worldwide. 1 Although the growth rate of obesity in U.S. children and adolescents has risen steadily since 2008, almost 1 in 10 children and adolescents is severely obese (body mass index [BMI] >35 kg/m2). 2 In one U.S. population study, overweight was seen in 35% of adolescents, whereas 21% had obesity (BMI ≥ the 95th percentile for age and gender). 3
The prevalence of overweight and obesity in children in Kuwait is increasing. In one cross-sectional study, 25.5% of Kuwaiti children were found to be overweight, whereas 36.5% were obese. 4 In another study, overweight and obesity were measured according to the definitions of the Centers for Disease Control and Prevention (CDC), International Obesity Task Force (IOTF), and World Health Organization (WHO) criteria. The prevalence of overweight was 17.7%, 23.3%, and 21.6% and the prevalence of obesity was 33.9%, 28.2%, and 30.5% according to CDC, IOTF, and WHO criteria, respectively. 5
The level of evidence regarding interventions combining diet, physical activity, and behavioral components to control weight in overweight or obese adolescents was low to moderate. 6 The long-term effects of such combined lifestyle interventions have been unsatisfactory, especially in extreme obesity with one Cochrane review (2009) indicating 1.7 kg/m2 BMI loss after 12 months. 7 Furthermore, the Evidence Report and Systematic Review for the US Preventive Services Task Force suggested that the clinical significance of medication use to treat obesity was unclear. 8
Obesity surgery has been found to provide better weight loss and reduce comorbidity but with higher risks when compared with lifestyle modification and pharmacotherapy. 9 However, an increasing number of studies have established the safety and efficacy of weight loss surgery for adolescents: after surgery, adolescents experience substantial weight loss, reduction in comorbidities, and improved psychological aspects.10–12
Surgical treatment of severely obese adolescents with type 2 diabetes mellitus (T2D) has been found to be associated with better glycemic control, weight loss, and reduced comorbidities, when compared with medical therapy. 13 Furthermore, Roux-en-Y gastric bypass (RYGB) was shown to reduce BMI and improved both insulin sensitivity and beta cell function in severely obese adolescents and young adults. 14
Our aim was to evaluate the safety and efficacy of sleeve gastrectomy (SG) in adolescents with severe obesity.
Materials and Methods
Our retrospective analysis included all consecutive morbidly obese adolescents (10–19 years) 15 with a BMI of at least 40 kg/m2 (or with a BMI >35 kg/m2 and multiple comorbid conditions) undergoing SG performed by a single surgeon in Kuwait between February 2012 and March 2018. Appropriate ethics committee approval was obtained.
The choice of procedure was based on patient and guardian's preferences after discussion on different surgical options and outcomes with the surgeon. Procedures were scheduled after a medical psychologist and pediatric endocrinologist had assessed the patients. Postoperative eating patterns were discussed with a dietician in the multidisciplinary team. The patient's family was involved actively in all the interviews and was clearly informed about the surgical plan and postoperative dietary instructions.
Demographics, comorbidities, BMI, preoperative weight, operative time, and hospital stay were evaluated. Outcome measures included change in weight, BMI, percentage excess weight loss (%EWL), postoperative complications, reoperations, and resolution of comorbidities.
Preoperative evaluation
Preoperative blood tests, gastroscopy, and gallbladder ultrasound examination were performed in all patients. Patients were put on high protein diet 2–4 weeks before surgery. Cholecystectomy was performed simultaneously if gallstones were detected.
After gastroscopy, patients with Helicobacter pylori were treated with antibiotics.
Surgical technique
Low molecular weight heparin (enoxaparin) was administered preoperatively and continued for 10–14 days. Antibiotics were given and continued until discharge. After lithotomy positioning, pneumoperitoneum was established. The liver was retracted by a grasper inserted into the subxyphoid area.
Patients underwent either a multiport technique (3–4 ports, 5–12 mm, n = 13, Excell®; Ethicon Endosurgery, Cincinnati, OH) or reduced port technique (a 5 cm incision above the umbilicus to introduce 10 mm and 12 mm trocars and a 5 mm port in the left subcostal area; n = 9).
A 36 Fr bougie was inserted. Gastric division started 4 cm proximal from the pylorus and ran up to the left crus. Two green loads were used on the antrum whereas blue loads were used on the rest of the stomach. The staple line was oversewn with absorbable sutures. Methylene blue was injected into the stomach through the calibration tube to check for patency. Neither drains nor nasogastric tubes were left in the abdomen in any patient in this series. The resected stomach was extracted through the 12 mm port site, and the port sites were closed with the Endo Close device (US Surgical™).
Postoperative management
Patients were allowed to have clear fluids on the first postoperative day and were discharged on the second postoperative day. Contrast-enhanced computerized tomography (CT) scan was performed postoperatively when there was fever and tachycardia.
Postoperatively, patients were commenced on clear fluids and were slowly given puree food until 4 weeks when solid food was introduced. Proton pump inhibitor was given postoperatively for 3 months. Multivitamins, iron, and vitamin B12 were given 1 week after surgery.
During the first postoperative year, patients were told to see the bariatric surgeon and dietician, at 1 week, 1 month, 2 months, 3 months, and then once every 2 months until 1 year. Patients were then informed to be seen twice yearly afterward.
Data analysis
Analysis of data was performed by using SPSS 22.0 for windows (Statistical Package for Social Sciences, Chicago, IL). Data were recorded as mean ± standard deviation and/or range. The chi-square statistic or Fisher's exact test was used for categorical variables. The unpaired t-test was used to assess the significance between means of two continuous variables. A p-value of 0.05 or less was considered statistically significant.
Results
Data from 22 patients (16/6, F/M) undergoing SG were analyzed. The mean age, preoperative weight, and BMI were 16.4 ± 2.1 years, 125.0 ± 30.2 kg, and 45.1 ± 8.1 kg/m2, respectively. A total of 16 of 22 adolescents had a BMI >40 kg/m2 (Table 1).
Demographic Data
BMI, body mass index.
A total of 19 of 22 patients underwent preoperative gastroscopy. Gastroscopy revealed a small hiatus hernia (n = 1), esophagitis (n = 1), gastritis (n = 3), and duodenitis (n = 1). A total of 18 of 19 patients undergoing ultrasound examination of the liver had fatty liver, whereas none had gallstones (Table 2).
Preoperative Gastroscopy and Ultrasound Findings
The mean operative time and median hospital stay were 54.7 ± 3.9 min and 2 days, respectively (Table 1). No patient had postoperative bleeding or leaks, reoperation, conversion, or mortality in our series (Table 3). Long-term nutritional complications were seen in one patient who underwent SG in 2016. His initial BMI was 64.5 kg/m2. Four months after surgery, he experienced repeated vomiting and weakness in the lower limbs. He was not taking postoperative vitamin supplementation regularly. He was admitted to the hospital several times for vitamin supplementation, including thiamine injections and intravenous fluids. Upper contrast studies revealed a minor kink at the incisura. The kink was dilated endoscopically but without major benefits. He was referred for psychiatric evaluation since there was no gastric outlet obstruction and no reflux or hiatus hernia.
Complications
Weight loss
Multiple phone calls and appointments were made to optimize follow-up. Median follow-up was 9 (range 1–60) months. The mean weight loss, BMI loss, and %EWL were 36.4 ± 31.8 kg, 13.8 ± 10.5 kg/m2, and 50.9% ± 27.1%, respectively (Table 4). Mean postoperative %EWL at 3 (12/22), 6 (7/22), 9 (6/22), 12 (6/22), 24 (3/22), and 36 (2/22) months after surgery was 30.7% ± 10.4%, 53.2% ± 18.2%, 59.8% ± 12.8%, 61.8% ± 22.3%, 62.6% ± 37.1%, and 66.3% ± 1.9%, respectively. During this period, the mean BMI loss was −8.6 ± 5.3, −15.9 ± 6.9, −14.7 ± 8.2, −13.3 ± 5.2, −20.5 ± 22.6, and −15.5 ± 7.9 for the follow-up visits (Fig. 1).
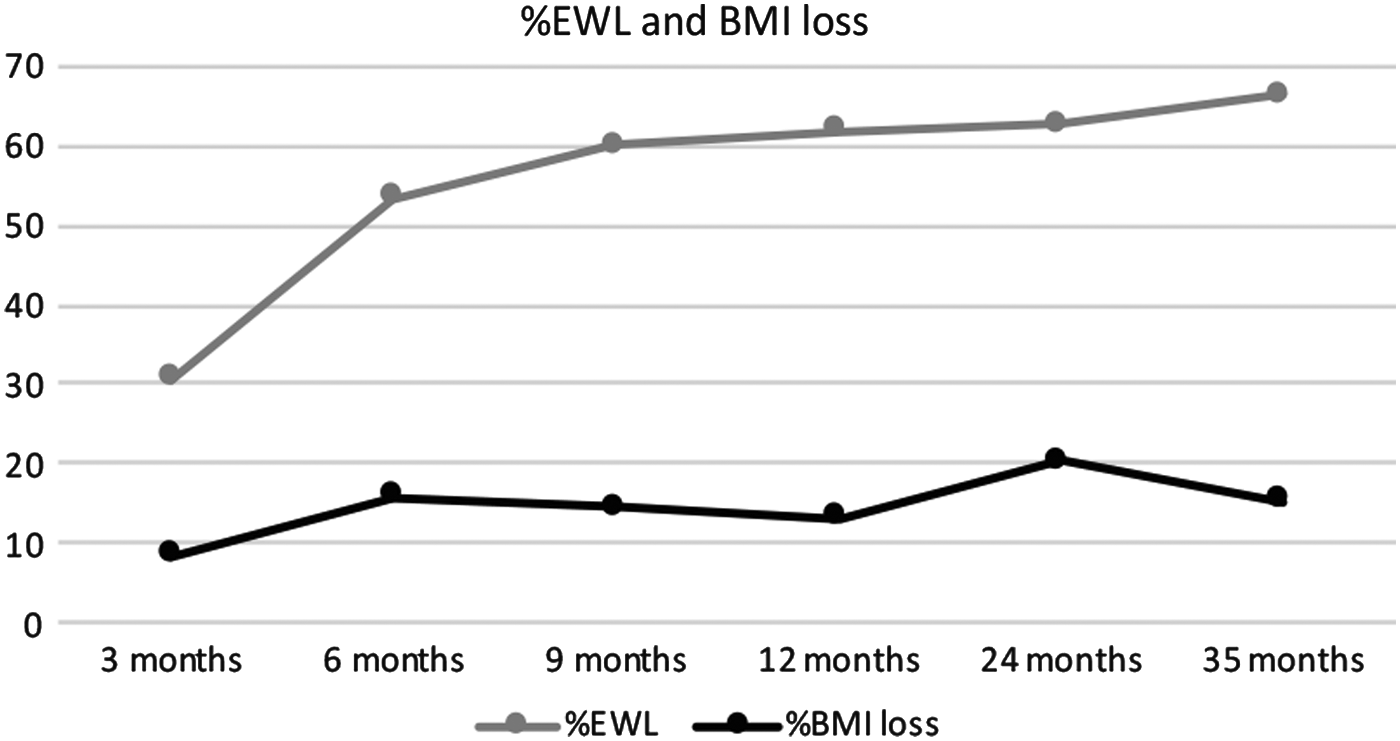
%EWL and BMI loss. BMI, body mass index; %EWL, percentage excess weight loss.
Follow-Up and Outcomes
%EWL, percentage excess weight loss.
Revisional surgery
Two patients required revisional surgery. One patient who had undergone laparoscopic adjustable gastric banding (LAGB) in 2010 when she was 17 years old had not lost weight and underwent laparoscopic band removal and SG 2 years later. She came to us in 2017 and her BMI was 44 kg/m2. CT volumetry and gastroscopy revealed a markedly distended stomach, measuring 895 cc. A repeat SG was performed; she lost 20 kg and her BMI dropped to 36.9 kg/m2 at 3 months but then was lost to follow-up. The second patient underwent intragastric balloon insertion in 2011 when she was 16 years old. She underwent SG a year later and her BMI dropped from 37.5 to 28.3 kg/m2. She regained weight and her BMI reached 31.4 kg/m2. LAGB on SG was performed 2 years later. On further follow-up, she maintained her BMI ∼30 kg/m2. Neither of the two patients had postoperative complications (Table 5).
Revisional Sleeve Gastrectomy
LAGB, laparoscopic adjustable gastric banding.
Reduced and multiport technique
Mean age, preoperative weight, BMI, operative time, or duration of hospital stay did not differ statistically significantly between patients undergoing reduced or multiport SG. The mean BMI loss was statistically significantly higher after the multiport technique (p = 0.03); however, there was no statistically significant difference in the mean %EWL (p = 0.4) (Table 6).
Multiport Versus Reduced Port Sleeve Gastrectomy
TBWL, total body weight loss.
Comorbidities
Preoperative comorbidities are indicated in Table 7. None of our patients was taking antidepressants.
Comorbid Conditions
ALT, alanine transaminase; OSA, obstructive sleep apnea; T2D, type 2 diabetes mellitus; TG, triglyceride.
Two patients had both hypertension and T2D and were on medications. Preoperative fasting blood sugar and hemoglobin A1C% for both patients were 6.5 mmol/L, 6.1 mmol/L and 6.7%, 7.2%, respectively. After surgery, both patients were allowed to discontinue medications for T2D. Postoperative fasting blood sugar and hemoglobin A1C% for both patients without medications was 4.6 mmol/L, 4.4 mmol/L and 6.6%, 5%, respectively. Only one patient discontinued treatment for hypertension. One patient with obstructive sleep apnea improved symptomatically after SG; however, he did not undergo objective assessment.
Discussion
In our study, we found that SG in obese adolescents reduced BMI by 13.8 ± 10.5 kg/m2 over a median follow-up of 9 months and improved comorbidities without substantial morbidity. This is comparable with other studies as summarized in three meta-analyses.16–18
In a survey published in 2010, almost half of 750 pediatricians and family physicians interrogated 3 years earlier said they would never refer adolescents for surgery, 19 mostly due to the absence of long-term data on efficacy and safety. One of the major concerns was vitamin and mineral deficiencies. There are no randomized studies comparing obesity surgery with another weight loss intervention for this population. There are also major ethical concerns with regard to who makes the decision to undergo surgery or not: the patients or their guardians.
An increasing number of studies have found that bariatric surgery was effective and safe in adolescents, as they experienced significant weight loss, reduction in morbidities, and improved psychological aspects.10–12
Weight loss outcomes are variable and studies on predictive factors remain sparse, especially among adolescents: of particular importance are social support, exercise, and binge eating. 20 Also, of note, improving family communication between adolescents and surrounding persons over time was found to be beneficial to optimize weight loss outcomes after surgery. 21
Bariatric surgery is effective to achieve short-term weight loss in obese adolescents.16,22 Conversely, long-term developmental and nutritional complications in this particular patient population are lacking. 17 However, one study from Qatar found that SG was associated with improved short- and long-term obesity comorbidity and decreased body image dissatisfaction among Qatari adolescent patients. 23 Another 7-year follow-up study found that RYGB in adolescents was safe, provided satisfactory weight loss, and cured comorbidities with a high degree of satisfaction. 24 Likewise, an Australian study found that BMI improved in the majority of adolescents and without specific postoperative morbidities. 25
Even though there were no randomized studies, a meta-analysis confirmed the effectiveness of SG for weight loss in obese adolescents. 22
Although several studies seemed to show that SG provided results similar to those of RYGB,10,18,26 others found that weight loss after SG was better than with LAGB.25,27
Obesity is associated with several comorbidities in adolescents and young adults.28,29 In our series, all of our patients with T2D had complete resolution without medications and one out of two for hypertension, similar to the outcomes reported by others.10,30,31 One patient with obstructive sleep apnea improved symptomatically after SG; however, he did not undergo objective assessment.
Eating habits and behavior patterns are particularly important to consider in the obese adolescent. RYGB is known to decrease food craving as well as other disordered eating symptoms in adolescents 32 compared with those treated with lifestyle modification. 33
Patient compliance in adolescents is important. Many adolescents referred for bariatric surgery do not follow the recommended bariatric programs before surgery, which usually consist of at least 6 months of behavioral and lifestyle education and this is certainly one of the contributing factors to low rates of adolescent bariatric surgery. 34 All our patients were referred to us after failure of lifestyle modification, explaining why we did not follow the recommended preoperative phase. However, adolescents who do not complete the preoperative phase of a bariatric surgery program are known to have clinically significant psychological symptoms. 35 We firmly believe that patients and their family must be educated regarding the benefits and risks, expected changes in eating habits, and the lifelong medical follow-up. Compliance with vitamin intake is important. In our series, one patient was not taking vitamins regularly because of intolerance, nausea, and vomiting even though both the family and patient had been correctly informed of the potential side effects. The patient was referred for psychiatric evaluation since there was no gastric outlet obstruction and no reflux or hiatus hernia.
Nonetheless, despite vitamin supplementation, nutritional deficiencies requiring hospitalization occur occasionally after SG and RYGB. According to Modi et al., 36 only 13–33% of adolescents are compliant with vitamin supplementation after bariatric surgery. Vomiting and noncompliance with medications are present in many of these patients, and 94% develop Wernicke encephalopathy within 6 months after surgery. 37 Recovery from Wernicke encephalopathy is incomplete in 49% of adults.37–39 SG may have less effects of malabsorption compared with RYGB. 40 Although RYGB is a reversible procedure, it may cause micronutrient deficiencies, especially iron, calcium, and vitamin B12.41,42 With low compliance rate after bariatric surgery in adolescents, RYGB remains a concern for us in adolescents. However, the drawbacks of SG include irreversibility and the need for long-term use of proton pump inhibitors. 43
The concern of growth interference after surgery is not a major issue, since most patients who underwent these procedures have attained their expected height at the time of surgery. 44 It has been shown that complications in pediatric patients undergoing bariatric surgery are lower than those in adult patients.45,46 In our series, the complication rate was 4.5% with no mortality.
Our study has several limitations. This was a retrospective study of 22 patients, a single surgeon's experience. Data were not always recorded and information on other comorbidities such as hyperlipidemia was not available. Although all diabetic patients were controlled without medications and one out of two patients with hypertension was no longer on medications, the follow-up was short (median, 9 months) and no formal conclusions could be drawn. Another limitation of this study was the incomplete follow-up of patients. However, it is also possible that those with the best outcome no longer saw any reason to continue follow-up and are among those lost to follow-up.
Conclusions
SG improved the BMI in the majority of our adolescents, without substantial postoperative morbidities. This procedure can be considered an effective and safe method to treat morbid obesity in adolescents as it can significantly decrease excess body weight and resolve comorbid conditions as shown in our series. Pre- and postoperative compliance is essential to minimize the risk of nutritional deficiencies and associated complications. Patients and family should be informed about the risks and benefits of bariatric surgery for this age group. Further studies are needed to investigate the long-term effects of SG in adolescents.
Footnotes
Author Disclosure Statement
No competing financial interests exist.