
Abstract
Background:
Robotic sleeve gastrectomy (RSG) is a new and popular option for obesity surgery. This study aims to analyze our experience during the transition period from laparoscopic sleeve gastrectomy (LSG) to RSG.
Patients and Methods:
Sixty patients with sleeve gastrectomy (SG) were enrolled into the study. Last 30 patients in the LSG group and first 30 patients in the RSG group were included in the study. Total operative time (OT), docking time, complications (intraoperative and postoperative), hospital stay, and amount of postoperative drainage were recorded and groups were compared.
Results:
There were no complications during surgery. There was no mortality or conversions to another approach in any patient. There were no leaks. Hospital stay, complication rates, and excess weight loss rates were similar in both groups. OT was longer in the RSG group. Postoperative drainage was lesser in the RSG group.
Conclusion:
RSG is safe and feasible and might be considered as an initial procedure for surgeons who plan to move forward to more complex procedures in bariatric surgery. For an experienced surgeon, the learning curve seems shorter for this procedure.
Introduction
Obesity is a growing public health problem worldwide. Bariatric surgery has been shown to be more effective in the management of morbid obesity and other comorbidities such as diabetes as compared with medical treatments and has currently been included in many guidelines.1,2
Sleeve gastrectomy (SG) is a restrictive procedure in which partial left gastrectomy including corpus and fundus of the stomach is removed to create a long tubular sleeve along the lesser curvature. SG has recently been recognized by the American Society for Metabolic and Bariatric Surgery not only as a primary procedure but also as a first step of the staged procedures. 3 For the past 10 years, we performed numerous complicated operations by minimally invasive techniques in bariatric procedures, thanks to the arrival of “da Vinci Surgical System” (Intuitive Surgical, Sunnyvale, CA). 4 Robotic sleeve gastrectomy (RSG) is a popular surgical option with the general advantages of robotic approach including better view of the surgical field and more precision during surgery.5,6 This method does not come without its drawbacks, however, and a prolonged learning curve and serious cost issues make up the main negativities, 7 but we chose to use the da Vinci system because of its lesser requirements and the experience it promises in bariatric robotic surgery. 8
The present study aims to analyze our initial comparative experience during the transition period from laparoscopic sleeve gastrectomy (LSG) to RSG.
Patients and Methods
Between May 2016 and April 2018, 210 patients have undergone bariatric surgery and 60 patients with SG were enrolled into study. All procedures were performed by an experienced surgeon (M.M.O.) who performed over thousand LSGs and had just started performing robotic bariatric surgery. Last 30 patients in his LSG group and first 30 patients in RSG were included in the study.
All patients had body mass index (BMI) >40 kg/m2 or BMI >35 kg/m2 with obesity-related health conditions and were reviewed by the multidisciplinary team (surgeon, endocrinologist, psychologist, dietitian, and anesthesiologist) before surgery. Patients were given verbal and written information on both procedures and on the known advantages of the robotic over the laparoscopic approach, such as three-dimensional vision, better view of the surgical field, and more precise dissection. In addition, patients were informed of an extra cost to be paid to the hospital in case of choosing robotic surgery. Eligible patients were absolutely free to choose the approach they wanted to adopt.
All bariatric procedures were performed by a single primary surgeon (M.M.O.) who had been recognized as a surgeon of excellence by International Federation for the Surgery of Obesity-European Chapter (IFSO-EC) with the assistance of one of the two additional attending surgeons (E.G. or C.E.G.).
A survey was performed to identify and compare the performance variables during completion of the learning curve. Total operative time (OT), docking time (DT), intraoperative and postoperative complications, length of hospital stay and postoperative drainage (mL), percentage of excess weight loss (%EWL), and BMI were compared among the groups.
Technique for LSG
The operative technique for LSG was standardized as explained by Özmen and Gagner. 9 Three trocars and a Nathanson liver retractor were used. The gastrosplenic omentum was divided from the greater curvature close to the stomach wall using ultrasound Harmonic Scalpel (Ethicon Endo-Surgery, Cincinnati, OH) or LigaSure (Covidien Medtronic, Minneapolis, MN) devices. This dissection was started at the middle of greater curvature that was completely dissected and the angle of His was fully delineated and mobilized. Both crura of the diaphragm were identified. Posterior adhesions to the pancreas were also freed. The sleeve of the stomach was created over a 36F gastric tube using linear stapler (i-Drive, Endo GIA; Covidien Medtronic), starting distally 2 cm from pylorus toward the 1 cm lateral from angle of His. The leak test was performed using methylene blue. The specimen of the stomach was removed and a Jackson–Pratt drain was placed. The drain was removed on the second postoperative day.
Technique for RSG
We used da Vinci Xi for robotic surgery in all our patients. Patients were put in supine position for RSG. We inserted the camera port through a point (2 cm lateral and 2 cm above) near the umbilicus. After insufflation to 12 mmHg to achieve pneumoperitoneum, patients were put in reverse Trendelenburg position. Following the placement of a Nathanson liver retractor from the epigastrium with direct visual monitoring, we inserted two bilateral hypochondriac ports of 8 mm size. Then, between the previous ports and in left side of the lateral abdomen, we placed another port of 12 mm size, and now patients had three robotic arms. Connecting these arms to the ports by moving the EndoWrist tools to the left side and next to the patients, we followed up by inserting the camera through the second arm. Finally, the console surgeon held the fenestrated bipolar forceps and the vessel sealer with robotic arms 1 and 3, respectively, and the surgical operation was carried out by completely complying with the description in LSG.
In the postoperative period the nasogastric tube was removed on postoperative day 1. All patients underwent a mandatory upper gastrointestinal tract series with contrast material on the second postoperative day. If this was normal, patients were started on liquid diet and were discharged on the postoperative third day after the removal of their drain. All patients received nutritional advice and were instructed to follow a liquid and semiliquid diet for 4 weeks. All patients were followed up in the first week, first month, and every 3 months in the outpatient clinic.
Statistical analysis
Descriptive statistics were presented as standard deviation and range for continuous variables and proportions for categorical variables. Comparisons between groups were performed using the χ2 test for proportions, Student's t-test for continuous variables, or a Mann–Whitney test when the distributions were significantly asymmetrical or the numeric variables ordinal; p < 0.05 was considered as statistically significant.
Results
This study evaluated a total of 60 patients; the last 30 LSG and first 30 RSG patients were included in the study. There were no cases of conversion to an open surgery for RSG and LSG or standard laparoscopic approach for RSG. In the LSG group 14 patients were men and 16 were women and in the RSG group there were 13 men and 17 women. The mean age was 38 (19–62) years in the RSG and 40 (24–63) years in the LSG groups. Mean BMI was 42.7 (36–50) kg/m2 in the RSG group and 41.6 (34–60) kg/m2 in the LSG group. Seven patients had type 2 diabetes mellitus (T2DM), 9 suffered from high blood pressure, 6 patients had dyslipidemia, and 12 had obstructed sleep apnea syndrome at the time of operation (Table 1). There were no differences between the two groups. There were no perioperative complications, mortality, or conversions to laparoscopic approach or open approach in any patient. There were no leaks in both groups.
Demographic Data and Comorbidities
BMI, body mass index; DM, type 2 diabetes mellitus; HT, hypertension; IR, insulin resistance; OSAS, obstructed sleep apnea syndrome.
Hospital stay was similar in both groups ranging from 3 to 4 days. The early and late complication rates, %EWL rates, and BMI were similar in the two groups. Total OT was longer for the RSG group (p < 0.05) (Fig. 1). Postoperative drainage (mL) was lesser in the RSG group (p < 0.05) (Table 2).
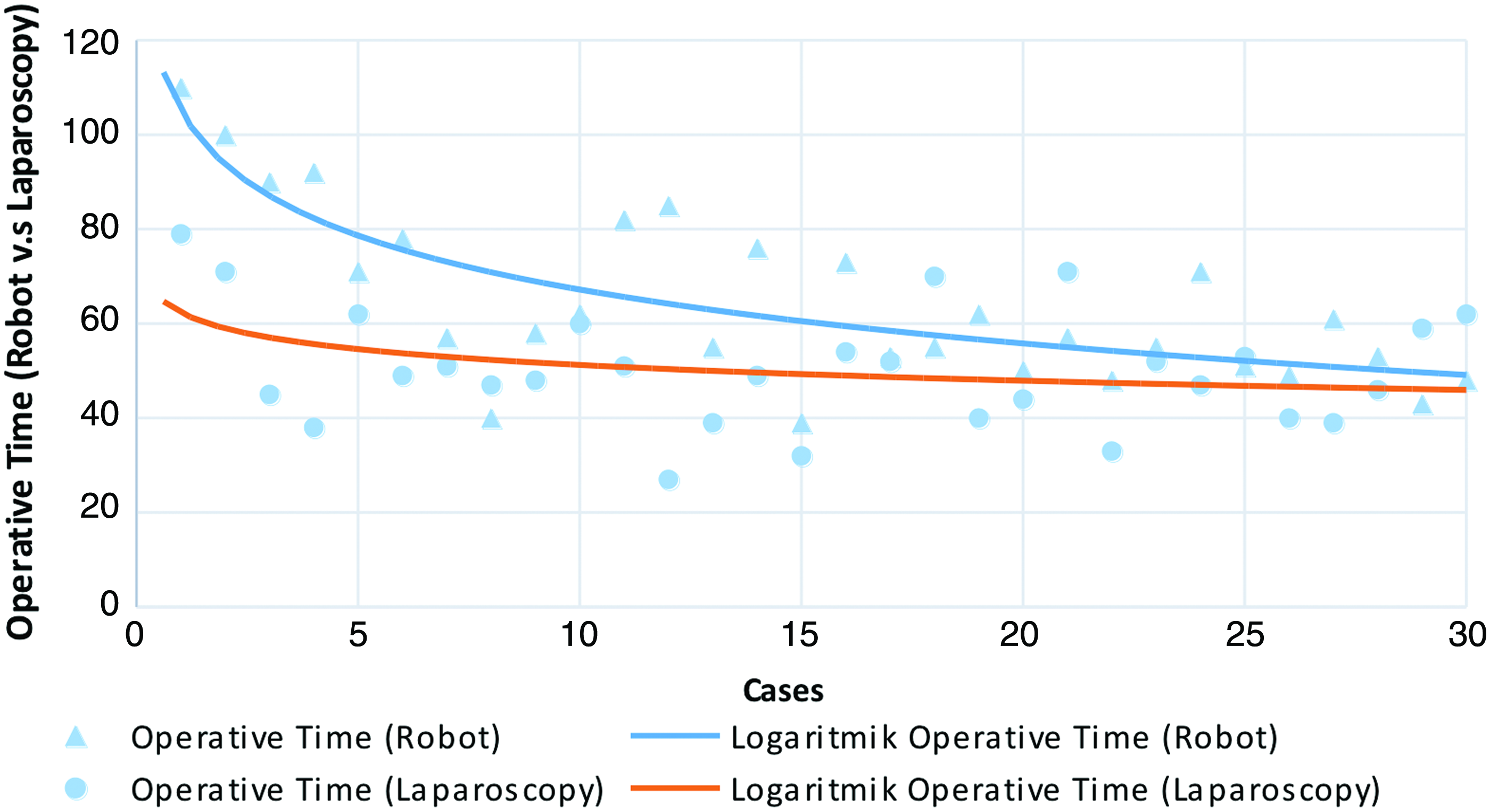
Operative time for LSG and RSG according to case number. LSG, laparoscopic sleeve gastrectomy; RSG, robotic sleeve gastrectomy. Color images are available online.
Operative Data, Surgical Complications, and Postoperative and Follow-Up Data
DVT/PTE, deep vein thrombosis/pulmonary thromboembolism; EWL, excess weight loss.
All patients in both groups experienced a decrease of their weight and BMI (Fig. 2A, B). All patients from both groups recovered from their comorbidities in high percentages after 6-month follow-up. T2DM resolved in all patients in both the RSG and LSG groups in early follow-up period.

Discussion
SG is a purely restrictive operation that reduces the size of the gastric reservoir to 60–100 mL, permitting the intake of only small amounts of food, and imparting a feeling of satiety earlier during a meal. It has been performed laparoscopically with good results. 10
With the introduction of the da Vinci robotic systems into the surgery in 2000 after the approval, several surgical procedures were switched to the robotic system. Robotic surgery made several interventions much easier as a result of the better field of view and higher maneuverability of the EndoWrist instruments. Robotic surgery techniques were also introduced into the obesity surgery and it was demonstrated that it enables a more effective and perfect anastomosis and access to difficult fields in several complex interventions such as gastric bypass and duodenal switches compared with the laparoscopic surgery.11,12 However, it was also stated that the robotic surgery requires high level of experience even for experienced surgeons. 4
In our study, we compared the first 30 RSG operations of an experienced surgeon with his last 30 LSG. Our investigation did not reveal any significant difference between the groups regarding postoperative or perioperative complications including bleeding, leakage, stricture and duration of the hospital stay, and weight loss. However, duration of operation, volume of the drainage fluid, and cost were significantly different.
Considering the reason for the difference in the operative duration, we found that there was actually no difference between the console time for the robotic intervention and the total duration of the laparoscopic operation. But the DT of the robotic surgery caused the statistical difference between these two techniques. Similar results were also reported by the studies conducted by Diamantis et al. 13 In a study by Vilalonga et al., it was reported that the learning curve process may have a low impact on overall surgical time. 4 Urrego et al. compared LSG and RSG and concluded that the primary contributor for the longer duration of robotic cases was OT. 14
Vilalonga reported that the learning curve was 20 for the robotic surgery in the SG. 4 However, our study showed that there was no significant difference between the first robotic procedure and the last 30 LSG, for the experienced high-volume surgeon. Therefore, the mentioned learning curve time and number of cases might be ignored for high-volume surgeons. Ballantyne et al. compared the open and laparoscopic gastric bypass operations and reported similar results and suggested 10 cases for the learning curve. 15
Although SG was considered a simple intervention, fatal complications such as bleeding and leakage because of the increased intragastric pressure caused by the long staple line and decline of the gastric volume may be encountered. In addition, complications like strictures in the sleeve pouch and possible strictures because of the twists may occur. Regarding the literature, the complication rates are 0.4%, for hemorrhage 1.4%, for leakage 0.36%, and for stricture 0.2%.16–18 The esophagogastric junction is a critical site for the leakage and 95% of the leakages emerge at this site. 15 We believe that the robotic approach enables a safer dissection and resection because of the increased field of view and accessibility of the operation field. There are also studies reporting that there is a correlation between the experience of the surgeon and the early and late complications. 19
In our study, we did not encounter any perioperative or postoperative bleeding requiring major or medical treatment. This might be because our primary surgeon was very much experienced and recognized as a surgeon of excellence by IFSO-EC.
The comparison of RSG and LSG shows that the postoperative volume of the drained fluid is statistically less in the RSG. Bleedings and the bleedings at the staple line in respect of the volume of the drained fluid and the dissection at the site of arteriae gastrica breves are particularly important. We believe that the presence of the maneuverability of the robotic vessel-sealing instruments in all access enables a more effective hemostasis at that stage. Although there is no significant difference between RSG and LSG in respect of the perioperative and postoperative parameters, the financial analysis shows that RSG is much more expensive than LSG. Several studies in the literature confirm also that RSG is a more expensive procedure.
Conclusion
In conclusion, SG might be considered as a first step for introducing robotic surgery into bariatric surgery. The learning curve seems to be very short for the high-volume laparoscopic surgeons considering bariatric surgery. The comparison of RSG and LSG did not show any significant difference except the cost. The RSG is a safe method in suitable patients with the short learning curve, similar results to laparoscopy and with other advantages of the robotic technology. Although it seems as costly as all new technologies, cost issues will need to be more clearly evaluated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.